
Abstract
Objective
Objective measure of scarring and three-dimensional (3D) facial asymmetry after surgical correction of unilateral cleft lip (UCL) and unilateral cleft lip (UCLP). It was hypothesized that the degree of scarring or asymmetry would be correlated with poorer psychological function.
Design
In a cross-sectional design, children underwent 3D imaging of the face and completed standardized assessments of self-esteem, depression, and state and trait anxiety. Parents rated children's adjustment with a standard scale.
Setting
Glasgow Dental School, School of Medicine, College of Medical, Veterinary and Life Sciences.
Patients
Fifty-one children aged 10 years with UCLP and 43 with UCL were recruited from the cohort treated with the surgical protocol of the CLEFTSIS managed clinical network in Scotland.
Methods
Objective assessment to determine the luminance and redness of the scar and facial asymmetry. Depression, anxiety, and a self-esteem assessment battery were used for the psychological analysis.
Results
Cleft cases showed superior psychological adjustment when compared with normative data. Prevalence of depression matched the population norm. The visibility of the scar (luminance ratio) was significantly correlated with lower self-esteem and higher trait anxiety in UCLP children (P = .004). Similar but nonsignificant trends were seen in the UCL group. Parental ratings of poorer adjustment also correlated with greater luminance of the scar.
Conclusions
The objectively defined degree of postoperative cleft scarring was associated with subclinical symptoms of anxiety, depression, and low self-esteem.
Craniofacial disfigurements such as cleft lip and palate (CLP) have been associated with psychological disturbance in some children and adolescents. The present study applies three-dimensional (3D) imaging procedures to define objective parameters of facial asymmetry and scarring in children who have had surgical repair of CLP in order to examine the relationship between those parameters and psychological status.
A recent systematic review has concluded that it is difficult to establish a consistent association between CLP and psychological morbidity because of the different methodologies applied across a wide range of research studies (Hunt et al., 2005). While many children are reported to have relatively few psychological difficulties (e.g., Persson et al., 2002; Gussy and Kilpatrick, 2006; Berger and Dalton, 2009), some studies have shown evidence of depression, anxiety, low self-esteem, and externalizing behaviors, which are symptomatic of distress and poor adjustment (Cheung et al., 2007; Kramer et al., 2008). The overall prevalence of poor adjustment has been estimated to be 30% to 40% (Endriga and Kapp-Simon, 1999), but Turner et al. (1998) suggested that such figures are an underestimate because only a relatively small number of clinical teams routinely assess psychological morbidity.
The relationship between the physical nature of the CLP and psychological status reflects the broad literature on disfigurement, which shows that the nature and degree of a disfiguring condition does not necessarily correlate in a linear way with the psychological distress reported (Thompson and Kent, 2001; Rumsey and Harcourt, 2004; Moss, 2005). The factor of residual scarring after cleft repair is an example in that it is visible to the child (who may be self-conscious) and to others whose reactions may be unsympathetic: Logically, then, the visibility of the scar might be assumed to correlate with poor psychological adjustment. However, while psychological disturbance has been ascribed to the degree of visibility of the cleft repair to the child and others (Broder and Strauss, 1989; Kapp-Simon et al., 1992; Broder et al., 1994; Thomas et al., 1997; Hunt et al., 2005), the association is not straightforward. For example, while Broder and Strauss (1989) found lower self-esteem in children with cleft lip, they noted that children with invisible defects also reported low self-esteem. Similarly, Spelz and Richman (1997) concluded that there were few differences in psychosocial outcome between those with visible, versus invisible, disfigurement.
The fact that the type, extent, and severity of the cleft disfigurement fail reliably to predict adjustment (Rumsey and Harcourt, 2004) would imply that there is interpatient variation in reaction to the physical nature of the cleft repair. Berger and Dalton (2011) have observed that an individual's social experience as a function of the reaction of others to the disfigurement may have consequences for the individual's satisfaction with his or her appearance and hence self-perception and adjustment. As the effects of such social experiences are likely to vary between individuals according to diverse factors such as coping skills and family and peer support (Thompson and Kent, 2001; Rumsey and Harcourt, 2004), the impact on adjustment may also vary from one person to another. In this context, it is relevant that some 60% of cleft children report being teased or bullied about their appearance and speech (Turner et al., 1997). Such reactions may be instrumental in influencing children's dissatisfaction with their appearance and inhibiting their social interaction (Tobiasen and Hiebert, 1993; Thomas et al., 1997; Hunt et al., 2005, 2006) and, for some, may have further consequences of anxiety, low self-esteem, and externalizing behaviors (Millard and Richman, 2001; Hunt et al., 2006; Hearst, 2007).
The precision in defining the nature and extent of the cleft is a further factor that may introduce variability to the assessment of the relationship between psychological adjustment and cleft disfigurement. While systematic investigations have shown that clinicians have generally good levels of agreement in their judgments of the nature and severity of various facial features, the correlation coefficients show that such agreement is not perfect and that there is both interrater and intrarater variation in making such judgments (Ritter et al., 2002; Edler et al., 2006; Kuipers-Jagtman et al., 2009). Moreover, it is known that clinical ratings of the degree of cleft-related disfigurement are not reliably associated with the psychological difficulties reported by the patient (Kapp-Simon et al., 1992). To reduce such variability and provide a greater measure of objectivity in assessment, the present study investigates the salience of the visibility of the disfigurement to psychological status by applying 3D imaging procedures to describe the appearance in objective numerical terms of facial asymmetry and the luminance, or visibility, of scarring. It is hypothesized that if psychological status is associated with the visibility of the disfigurement, then scores on assessments of psychological morbidity will be positively correlated with the objective degree of that disfigurement.
Methods
Ethical Approval
Approval was granted by the West Glasgow Ethics Committee (REC No. 05/S0709/81). Patients and their parents received an information sheet and signed a consent form.
Participants: Recruitment and Exclusions
Two groups of 10-year-old cleft children participated: 51 had unilateral cleft lip and palate (UCLP) and 43 had unilateral cleft lip (UCL). All cases had been treated following the same surgical protocol that has been adopted by the managed clinical network in Scotland, CLEFTSIS. Children were excluded if English was not their first language, as this would have impeded their completion of the self-report psychological assessments (described below). In addition, 68 noncleft children living in the same geographic area were recruited as a control group for the 3D imaging component of the study. The control children did not complete the psychological assessments because this was deemed inappropriate by the ethical committee on the grounds that it would be unnecessarily intrusive and that published normative data were available for comparison purposes with the two cleft groups.
Study Design and Power
It was anticipated that 100 cleft children would be recruited, 50 having UCL and 50 UCLP. In addition to comparing the psychological status of the two groups, it was of interest to examine the association between psychological status and measurements of soft tissue deformity and scarring. Under the assumption of normality, when the UCL and UCLP groups are combined to give a sample size of 100, a test of the null hypothesis of zero correlation gives power of 85% when the true correlation coefficient is .3. For a sample size of 50, this test gives power of 82% when the true correlation coefficient is .4. The sample size therefore provided adequate power to detect moderate degrees of correlation.
3D Imaging
For each case, the face was captured using a high-resolution stereophotogrammetric 3D imaging system (Di3D). The 3D facial images were taken of each child in a rest position and with maximal smile. Only rest images are analyzed here. The output was in the form of an onscreen colored photorealistic image of the participant in virtual reality modeling language. For right-sided clefts, the 3D images of the face were reflected to the left side to create a homogenous group for statistical analysis. A custom-written computer program allowed the construction of 3D facial models and the placement of facial landmarks (Fig. 1).
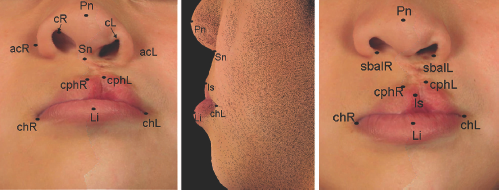
Digitized anatomical landmarks of one of the UCLP cases.
Psychological Assessment
Children completed the following standardized and well-validated assessments of self-esteem, depression, and anxiety, which have been shown to be sensitive outcome measures in previous research (Broder and Strauss, 1989; Turner et al., 1998; Rumsey and Harcourt, 2004; Hunt et al., 2006).
Culture-Free Self-Esteem Inventory version 2 (CFSEI-2).
The CFSEI (Battle, 1992) provides a total self-esteem score composed of subscales concerning the child's rating of the esteem in which they are held by their parents, at school, and socially and their general self-perception (Cronbach's alpha = .71; test-retest reliability range = .81 to .89; concurrent validity range = .71 to .80; Battle, 1992). The inventory includes a so-called lie scale to detect children who may be responding in what they believe to be a socially desirable way as a defensive mechanism or in deference to clinical staff: Such a tendency has been suspected in children with CLP (Thomas et al., 1997; Hunt et al., 2005).
Children's Depression Inventory (CDI).
The CDI (Kovacs, 1992) derives a total score for self-reported depressive symptoms from subscales of negative mood, interpersonal problems, ineffectiveness, anhedonia, and negative self-esteem (Cronbach's alpha = .86; test-retest reliability range = .66 to .83; concurrent validity = .72; Kovacs, 1992).
State-Trait Anxiety Inventory for Children (STAI-C).
The STAI-C (Spielberger et al., 1973) assesses self-reported current anxiety (state anxiety) and chronic anxiety (trait anxiety; Cronbach's alpha range = .78 to .87; test-retest reliability range = .16 to .62; concurrent validity = .75; Spielberger et al., 1973).
Parents completed the Revised Rutter Parent Scale for School-Age Children (RRPSS-AC; Rutter, 1997), which obtains parents’ ratings of their children on a range of behaviors that are indicative of emotional and behavioral disturbance. A “total difficulties” score is derived from the sum of subscales of “emotional difficulties,” “conduct difficulties,” “hyperactivity/inattention,” and “prosocial behavior” (test-retest reliability = .74; Rutter, 1997).
Imaging
Assessment of residual dysmorphology following cleft repair involved measurement of lip scarring and facial asymmetry.
Lip Scarring
The magnitude of facial scarring was measured using a custom-written program to detect differences in color content between the area of scarring and the surrounding region. For this preliminary analysis, only a single 2D image was used of each participant, taken from the camera with the most orthogonal view of the scar. The CIELAB color coordinates were extracted from the images using standard techniques of digital colorimetry (Westland and Ripamonti, 2004). CIELAB color coordinates decompose each color image into three separate images: a luminosity (L*) image, an image based approximately on the relative redness (as opposed to greenness; a*), and an image based approximately on the amount of yellowness as opposed to blueness (b*; Ayoub et al., 2011). For each facial image, a region of interest (ROI) was extracted (by hand), which included the base of the nose and the vermilion regions of the lips. This image was then segmented automatically, using the color information, to remove the vermilion section of the lip from the image, so that the ROI was restricted to the region between the base of the nose and the top of the vermilion border. The entropy (an image measure related to the variability of the image across space) of the a* image within the ROI was then determined, and the closed region with highest entropy was identified. This was taken to be the candidate “scar” region. The color coordinates of this scar region were then compared with those of the surrounding skin.
Facial Asymmetry
Asymmetry was measured by a validated algorithm. First, the geometric centers of the two configurations (original and reflected) were found. They were then translated so that they were superimposed on their geometric center using Procrustes analysis.
The squared distances between landmarks in the original and reflected configurations were expressed as general facial asymmetry scores for each subject. The calculated asymmetry scores are expressed in millimeters; the perfect symmetric face would have a score of zero. The higher the score, the more asymmetric is the face. Higher asymmetry scores indicate increased facial asymmetry. The overall asymmetry score was also decomposed into scores for subfeatures of the face. The technical details are described in Bock and Bowman (2006).
Statistical Analysis
To compare the mean questionnaire scores of UCL and UCLP groups to the normative means (where available), the data were required to be normally distributed. Scores on the CDI, STAI-C, and RRPSS-AC questionnaires were positively skewed, while scores on the CFSEI-2 questionnaire were negatively skewed. A square-root transformation improved normality on all score distributions (the CFSEI-2 scores were reflected before transforming). Appropriate calculations were performed to compute the variance of the transformed normative data from the mean and variance of the original untransformed normative data. As the analysis involved multiple comparisons between the two groups and the normative means, a more conservative α value of .005 for statistical significance was therefore set to reduce the risk of type I error.
Regression was used to relate psychological scores to measures of facial shape and scarring. Specifically, a multiple linear regression model was used, with covariates for scar luminosity (L*) and redness (a*), asymmetry (lip, nose, and global) and the first principal component of shape. The use of multiple regression allows the relationship between psychological outcome and each variable of interest to be assessed while adjusting for the possible presence of other relationships. The asymmetry scores were expressed on a log scale to reduce skewness. As particular interest lies in the relationships between the psychological measurements and scarring, and as 10 P values were computed for these within each group (UCL and UCLP), statistical significance was again set at .005 to control the type I error.
In the absence of a control group (see above), comparisons were made between the UCL and UCLP groups and the normative data available with the standardized psychological assessments. The latter data provided means, standard deviations, and sample sizes, which allowed statistical comparisons to be conducted with the study data.
Results
Table 1 summarizes the demographic data and shows that the UCL and UCLP groups were comparable in terms of gender and socioeconomic background.
Demographic Summary Statistics by Subject Group *
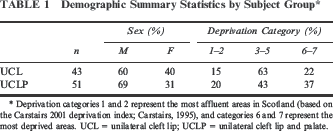
Deprivation categories 1 and 2 represent the most affluent areas in Scotland (based on the Carstairs 2001 deprivation index; Carstairs, 1995), and categories 6 and 7 represent the most deprived areas. UCL = unilateral cleft lip; UCLP = unilateral cleft lip and palate.
Table 2 shows the original untransformed mean scores of the two groups on the five psychological assessments and normative data in the form of mean performance and/or cut points denoting clinical significance.
Mean Psychological Assessment of the Original Untransformed Variables (SD Shown in Parentheses) for the Groups Having Unilateral Cleft Lip (UCL) or Unilateral Cleft Lip and Palate (UCLP) *
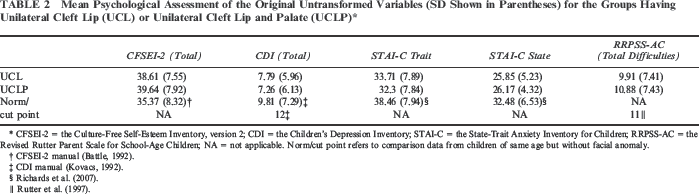
CFSEI-2 = the Culture-Free Self-Esteem Inventory, version 2; CDI = the Children's Depression Inventory; STAI-C = the State-Trait Anxiety Inventory for Children; RRPSS-AC = the Revised Rutter Parent Scale for School-Age Children; NA = not applicable. Norm/cut point refers to comparison data from children of same age but without facial anomaly.
CFSEI-2 manual (Battle, 1992).
CDI manual (Kovacs, 1992).
Self-Esteem (CFSEI-2)
Mean total self-esteem did not differ between the two groups, and nor did it differ on any subscale. However, both groups scored higher in self-esteem than the normative mean, the difference being significant in the case of UCLP children (P < .001) and of marginal significance for the UCL group (P = .008). Boys and girls did not differ on any measure of self-esteem.
The lie scale of the CFSEI-2 detects those children who may attempt to answer in a way to portray themselves in a socially ideal or acceptable light. Scores of 5 or more (in a range from 0 to10) have been proposed to “indicate a lack of defensiveness when responding to lie items” (Battle, 1992): That is, the higher the score, the less the tendency to socially-ideal portrayal. For the UCL and UCLP groups, respectively, 68% and 81% scored 5 or more: The difference between the groups was not significant. Most children therefore showed no tendency to represent themselves in an ideal way.
Depression (CDI)
The UCL and UCLP groups did not differ significantly in their total depression scores nor on any CDI subscale, and nor were there differences between males and females. However, the average total depression score was lower than the normative mean both for the UCLP (P = .01) and UCL (P = .055) groups, neither being significant according to the corrected α level noted above. A cutoff score of 20 has been established to denote clinical levels of depression (Kovacs, 1992): Only 3 children in the whole cohort (3%) scored above the cutoff (two being UCL and one being UCLP).
Anxiety (STAI-C)
The groups did not differ significantly in state or trait anxiety, and nor were there significant differences as a function of gender. There are no formal UK norms for the STAI-C, and the North American norms derive from 1973, but data from Richards et al. (2007) provide a relevant comparison as they represent a similar sample of UK children to those of the present study. The mean state and trait anxiety scores of the UCL and UCLP groups were significantly lower than those of the study by Richards et al. (state anxiety, both P < .001; trait anxiety, P = .005 and P < .001 for the UCL and UCLP groups, respectively).
Behavioral Problems (RRPSS-AC)
The mean total difficulties score did not differ significantly between the groups. A total behavioral difficulties score of 11 or more denotes disturbance that is of clinical significance. The percentage of UCL and UCLP children who were rated by their parents as scoring above the criterion was 38% and 44%, respectively, with the between group difference being nonsignificant. The groups did not differ on any of the questionnaire subscales, nor were there differences due to gender.
Correlations Between the Psychological Measures
Table 3 shows the correlations between the parent-rated RRPSS-AC and the children's scores on the CFSEI-2, CDI, STAI-S, and STAI-C. The RRPSS-AC total behavioral difficulties score was significantly and negatively correlated with the child-rated measure of self-esteem only in the case of UCLP children (P = .002). Thus, the lower the children's self-esteem, the greater was the parental perception of behavioral difficulties.
Correlations Between the Parental Ratings on the Revised Rutter Parent Scale for School-Age Children (RRPSSA-C) and the Child Self-Ratings on the State-Trait Anxiety Inventory for Children (STAI-C State and STAI-C Trait), the Culture-Free Self-Esteem Inventory, version 2 (CFSEI-2), and the Children's Depression Inventory (CDI) *
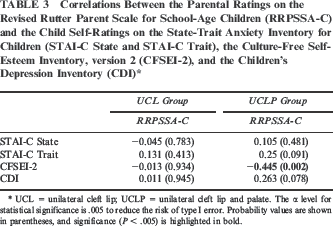
UCL = unilateral cleft lip; UCLP = unilateral cleft lip and palate. The α level for statistical significance is .005 to reduce the risk of type I error. Probability values are shown in parentheses, and significance (P < .005) is highlighted in bold.
Regression Analysis: Psychological Status and Scarring and Facial Asymmetry
Table 4 shows the regression coefficients describing the relationship between psychological status and the visibility of scarring. The L* and a* ratios denote the luminance and redness of the scar, respectively.
Regression Coefficients for the Relationship Between the Psychological Assessments and Imaging Parameters in the UCL and UCLP Groups *
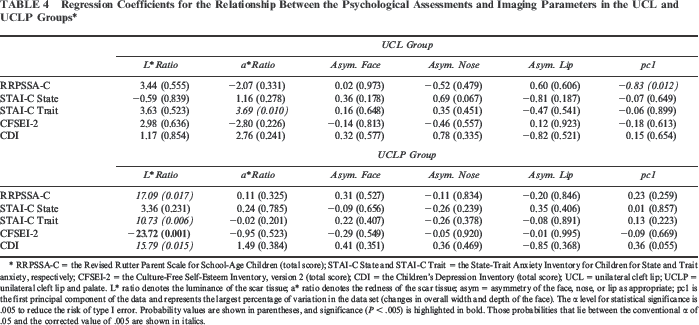
RRPSSA-C = the Revised Rutter Parent Scale for School-Age Children (total score); STAI-C State and STAI-C Trait = the State-Trait Anxiety Inventory for Children for State and Trait anxiety, respectively; CFSEI-2 = the Culture-Free Self-Esteem Inventory, version 2 (total score); CDI = the Children's Depression Inventory (total score); UCL = unilateral cleft lip; UCLP = unilateral cleft lip and palate. L* ratio denotes the luminance of the scar tissue; a* ratio denotes the redness of the scar tissue; asym = asymmetry of the face, nose, or lip as appropriate; pcl is the first principal component of the data and represents the largest percentage of variation in the data set (changes in overall width and depth of the face). The α level for statistical significance is .005 to reduce the risk of type I error. Probability values are shown in parentheses, and significance (P < .005) is highlighted in bold. Those probabilities that lie between the conventional α of .05 and the corrected value of .005 are shown in italics.
Table 4 shows that the visibility of scarring was associated with the children's self-reported psychological status. Within the UCLP group, the L* ratio was negatively associated with self-esteem (P = .001) and positively associated with trait anxiety (marginal significance: P = .006) and nonsignificantly with CDI depression (P = .015). In other words, greater luminance of the scar was associated both with significantly lower self-esteem and greater reporting of symptoms of anxiety and with a trend to greater reporting of depressive symptoms. Within the UCL group, while the associations did not reach the corrected level of significance, the a* ratio was positively associated with trait anxiety (P = .01) and negatively with self-esteem (P = .226). There were no significant associations between measures of facial asymmetry and the children's self-report measures.
Parental ratings of behavioral problems in UCLP children (RRPSS-AC total difficulties score) were positively associated with the L* ratio (P = .017), indicating that the greater the luminance of the scar, the greater were the parentally perceived behavioral problems. In the case of the UCL group, parental ratings were negatively associated with the pcl component reflecting changes in the overall width and depth of the face (P = .012). Neither association was, however, significant according to the adjusted α level and must therefore be regarded as trends.
Discussion
The present results provide little evidence of significant psychological disturbance in this cohort of Scottish children who, overall, had higher self-esteem and fewer self-reported symptoms of depression and anxiety when compared with valid reference data. The results are therefore consistent with earlier findings of Berger and Dalton (2009), Gussy and Kilpatrick (2006), Millard and Richman (2001), and Persson et al. (2002) and with the overall conclusion of the systematic review by Hunt et al. (2005). In the case of depression, the finding that 3% of the sample scored above the threshold value denoting possible clinical depression is largely consistent with the estimated prevalence of 1% to 2% in pediatric and adolescent populations (Ryan, 2005). The fact that the psychological profiles of the UCLP and UCL groups were similar is also consistent with evidence that the type and severity of the cleft has little effect on overall psychological function (Hunt et al., 2005).
There was therefore little overall evidence of emotional disturbance in terms of the number of children whose scores were above the clinical cut points. Importantly, however, the range of the data distributions of the psychological assessments indicated that there was variation between children in their self-reported (nonclinical) symptoms of depression, anxiety, and low self-esteem, which reflect the normal everyday concerns of children. These distributions are important with respect to their covariation with the objective measures of scarring. The regression analyses indicated that, even within this cohort of children whose overall psychological status was good, there was a relationship between the visibility of residual scarring and scores, reflecting a greater number of psychological symptoms. The relationship was strongest in the case of UCLP children, in whom the objective visibility of the scar (L* ratio) was associated with a lowering of self-esteem and more reported symptoms of trait anxiety. It is notable that the significant negative association between scar visibility and self-esteem seen in the UCLP group replicates findings of lower self-concept scores in such children when compared with other cleft types (Broder and Strauss, 1989). A similar pattern was observed in UCL children in whom the redness of the scar (a* ratio) was associated with higher trait anxiety and lower self-esteem, although the associations failed to reach the corrected α level for significance.
The results also replicate findings that parental ratings of their children's psychological state after correction of a cleft are often more negative than those of the children themselves (Hunt et al., 2007; Kramer et al., 2008). While some 40% of the parents rated their children as having psychological difficulties of clinical significance, the children's self-ratings were not generally consistent with this view. There was an exception, however, in the case of UCLP children, in whom there was a significant association between the parental rating of behavioral problems and the children's reporting of low self-esteem. The association might imply that while self-esteem was generally high in UCLP children, parents were sensitive to lower levels of the emotion in their children and rated them accordingly. However, an alternative explanation is that children's awareness of their parents’ negative view of their behavior might cause them to be more conscious of their appearance and view it either as responsible for their parents’ attitude or as a further confirmation of their (the children's) “negative” qualities. The consequence might then be an adverse effect on children's self-perception and self-esteem (see Bull and Rumsey, 1988, cited by Thomas et al., 1997).
Parents perceived more behavioral problems as a function of increased visibility of scarring (UCLP children) and reduction in the width and depth of the face (UCL children), although these associations were not statistically significant when adjusted for multiple comparisons. Nonetheless, a cautious interpretation might be that the parents’ ratings were influenced by the visibility of the after effects of the cleft repair and thus how noticeable they believed them to be to their child and to others. Parents might then draw the implication—correct or otherwise—that there would be adverse consequences for their child through teasing, or by the child's sensitivity to stigma, so that the parents then ascribed negative connotations to any behavioral or emotional change in the child.
It is possible that children with severe residual facial scarring or asymmetry would show greater psychological disturbance or that those with preexisting higher levels of trait anxiety and depression would react more strongly to lesser degrees of scarring. These hypotheses could not be examined in the present study, first because none of the children had any marked residual disfigurement. Second, the number of children scoring in the extreme ranges of anxiety, depression, and low self-esteem was insufficient for any meaningful analysis (only four UCL and two UCLP children were within the upper quartile on the STAI-C and CDI and within the lower quartile on the CFSEI-2).
The study has a number of limitations. Its cross-sectional design precludes analysis to determine whether psychological status is subject to change over time and particularly before and after correction of the cleft. Furthermore, the study did not assess the children's satisfaction with their facial appearance, although, as noted above, dissatisfaction with appearance has been shown to be associated with poorer adjustment (Millard and Richman, 2001; Rumsey and Harcourt, 2005; Hunt et al., 2006; Hearst, 2007). Therefore, while the regression analyses showed significant relationships between objectively defined scarring and adjustment, it is possible that the inclusion of a measure of satisfaction with appearance would have explained further variance in the relationship between the former two variables. It would also have been preferable methodologically to have collected psychological data from the control group, but as explained, this was precluded on ethical grounds. This omission was, however, mitigated in part by the fact that it was possible to compare the two cleft groups with valid normative data in order to determine their psychological status. Moreover, the outcome of interest concerned the association between objective measures of scarring and psychological status, which clearly would be impossible to measure in the control children who, by definition, had no scarring.
Conclusion
The present study confirms earlier findings that children may sustain a good psychological adjustment after surgical correction for cleft lip and palate. While there was a range of scores on measures of depression and anxiety, there was no evidence that the incidence of problems exceeded their prevalence in the population. The results indicate that the use of 3D facial imaging has proved an effective and objective way of demonstrating associations between the visibility of postoperative scarring and increases in reporting of (nonclinical) symptoms of depression, anxiety, and low self-esteem, hence demonstrating the sensitivity of children, and their parents, to subtle residual disfigurement.