
Abstract
Objective
Macroglossia is a common feature of Beckwith Wiedemann Syndrome (BWS). Tongue reduction surgery (TRS) is advocated to overcome, or reduce, the secondary effects of macroglossia. Macroglossia may affect a child's cosmetic appearance, feeding, and drooling function. However, no study has systematically reported on feeding, drooling, or psychosocial outcomes preoperatively and postoperatively in this group. This study aimed to describe the presurgical and postsurgical psychosocial, feeding, and drooling outcomes of children with macroglossia associated with BWS and to determine the effect of TRS on these areas.
Design
Clinical cohort study.
Participants
Ten consecutively admitted children with BWS (age at surgery from 9 months to 4 years, 9 months [4;9]; mean, 2;7) were assessed preoperatively, 3 months postoperatively, and at long-term follow-up.
Main Outcome Measures
A parental report questionnaire, the Brodsky drooling scale, and a feeding rating scale.
Results
Parents reported that macroglossia had a negative impact cosmetically that was ameliorated following surgery. Macroglossia caused a range of feeding difficulties presurgically by preventing lip seal and bolus manipulation during the oral preparatory phase. Excessive drooling was present in all cases presurgically. This resolved partially across the group postsurgically, with almost complete recovery at longer-term follow-up assessment.
Conclusions
Presurgically, children show a common profile of feeding and drooling impairment with negative effects on cosmetic appearance. Our preliminary results demonstrate that TRS has a positive impact on these features with good outcomes for children with BWS.
Beckwith Wiedemann Syndrome (BWS) is a congenital overgrowth syndrome with an estimated frequency of approximately 1:13,700 births, affecting both males and females (Engstrom et al., 1988). Features of the condition include prenatal and childhood overgrowth (high weight and height), macroglossia (enlarged tongue), hemi-hypertrophy (asymmetric growth), anterior abdominal wall defects including exomphalos or umbilical hernia, ear lobe creases and posterior ear pits, neonatal hypoglycemia, and predisposition to childhood tumors, particularly Wilms tumor of the kidney (Elliott et al., 1994; Weksberg et al., 2005). A number of different genetic and epigenetic abnormalities at the imprinted 11p15 growth regulatory region cause BWS and are identifiable in 80% of individuals who fulfill the classical diagnostic criteria (Elliott et al., 1994; Weksberg et al., 2005). The cause in the remainder is not known.
Since the advent of molecular testing for 11p15 defects, it has emerged that many children with the condition manifest with milder features of the condition and would not fulfill the originally proposed diagnostic criteria. For example, 20% of children with isolated hemi-hypertrophy have 11p15 abnormalities (Merks et al., 2005). The frequency of each clinical feature in unselected individuals with 11p15 defects is not currently known. Among those fulfilling the classical diagnostic criteria, macroglossia is the most common feature, being present in 82% to 100% of cases (Table 1; Engstrom et al., 1988; Elliot and Maher, 1994; McManamny and Barnett, 1985; Pettenati et al., 1986; see Fig. 1).
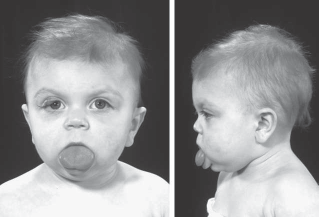
A and B: Front and side views of an 18-month old child with BWS who has unoperated macroglossia. The tongue is in a rest position in both pictures. Reprinted with permission from Shipster C, Oliver B, Morgan A. Speech and oral motor skills in children with Beckwith Wiedemann syndrome: pre- and post-tongue reduction surgery. Adv Speech Lang Pathol. 2006;8:45–55.
Comparison of the Clinical Features of Beckwith-Wiedemann Syndrome †
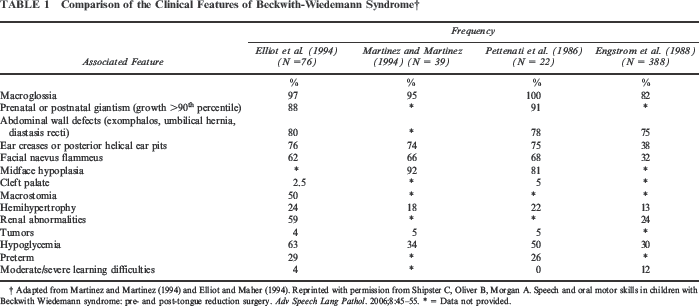
Adapted from Martinez and Martinez (1994) and Elliot and Maher (1994). Reprinted with permission from Shipster C, Oliver B, Morgan A. Speech and oral motor skills in children with Beckwith Wiedemann syndrome: pre- and post-tongue reduction surgery. Adv Speech Lang Pathol. 2006;8:45–55.
= Data not provided.
Enlargement of the tongue results from hyperplasia of muscle fibers, and while the tongue is generally increased in all three dimensions (Sokoloski et al., 1978; Vogel et al., 1986), there may also be individual variation in the presentation of the tongue (Shipster et al., 2006). To date, there are no objective techniques routinely used in the clinical diagnosis of macroglossia, and the diagnosis is based on subjective criteria including the degree of tongue protrusion and the clinical signs and symptoms that occur secondary to the macroglossia (Vogel et al., 1986; Wolford and Cotrell, 1996; see Table 2).
Functional Signs and Symptoms of Macroglossia *
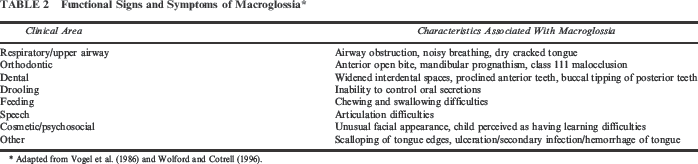
Adapted from Vogel et al. (1986) and Wolford and Cotrell (1996).
Tongue reduction surgery (TRS) has been cited by several authors as an effective means of overcoming or reducing secondary effects (Table 2) of the macroglossia (Murthy and Laing, 1994; Wolford and Cottrell, 1996; Kacker et al., 2000). The aim of surgery is to reduce the length, width, and central tongue bulk. Some have reported, however, that TRS may have a negative effect on speech and chewing skills secondary to a hypoglossal nerve injury or scarring (Egyedi and Obwegeser, 1964; Wolford and Cottrell, 1996). Despite several reports in the literature describing surgical techniques for TRS in this population (Kveim et al., 1985; Mixter et al., 1993; Davalbhakta and Lamberty, 2000; Kacker et al., 2000), there remains a dearth of literature reporting on cosmetic/ psychosocial and functional outcomes such as speech, oral-motor skills, feeding, and drooling following surgery.
Only one study has systematically investigated functional oral-motor and speech outcomes before and after tongue reduction surgery in children with BWS (Shipster et al., 2006). In this study, which included 10 children, distinct articulatory errors caused by macroglossia were present preoperatively, and these errors were subsequently eliminated by TRS. Normal oral motor skills were present preoperatively, and functional oral motor skills were found following surgery, with the exception of one case who had co-occurring neurological impairment.
With regard to feeding skills in children with macroglossia related to BWS, Van Borsel et al. (1999) conducted a parent questionnaire in which it was reported that 21 of the 40 children had eating and swallowing difficulties. Unfortunately, the nature of the feeding difficulties was not described, nor was the age of the children at the time they presented with the difficulties, nor whether the feeding problems had resolved following surgery. A limited number of further studies have reported on the presence of feeding difficulties in infancy and have advocated surgery in infancy for children showing signs of eating and drinking problems (Weng et al., 1995; Elliot et al., 1994; Kacker et al., 2000). Again, however, little detail is provided on the nature of the feeding impairment, and no systematic postsurgical outcome data are reported indicating whether TRS was effective in relieving feeding problems.
Unrelated to surgical outcome, the enlarged tongue has been associated with impaired posterior movement of the tongue and the associated propulsion of the bolus as required for oral transit of food or fluids (Rizer et al., 1985). Salman (1988) also reported failure to thrive and the need for nasogastric feeding prior to tongue reduction surgery. These studies highlight the critical need for further investigation into presurgical feeding issues and the potential impact of BWS on nutrition in this population.
Drooling (i.e., “spilling of saliva from the mouth onto the lips, chin, neck, and clothing”; Brodsky, 1997), normally occurs in infants and young children, particularly when a child is learning a new motor skill or cutting a new tooth. Although occasional drooling may persist in the neurologically intact child throughout the preschool years, drooling during wakefulness beyond 3 or 4 years of age is considered abnormal (Crysdale, 1989).
Consequences of drooling include irritated facial skin, increased oral and perioral infections, hygiene problems, frequent changes of clothing, and dehydration (Cotton and Richardson, 1981; Lew et al., 1991; Crysdale and White, 1989). However, the most unfortunate consequence of drooling may be social isolation. This is because drooling is unsightly and produces an unpleasant odor, people may avoid individuals who drool, and physical contact may be reduced. Isolation, in turn, can have devastating effects on self-esteem (Blasco and Allaire, 1992).
Several studies state that drooling is a commonly associated problem preoperatively in BWS (McNanamny et al., 1985; Vogel et al., 1986; Rizer et al., 1985; Murthy and Laing, 1994; Elliot and Maher, 1994; Van Borsal et al., 1999). Siddiqui and Pensler (1990) and Wolford and Cottrell (1996) stated that drooling is reduced following TRS. No study, however, provides details about the age of the children, and hence it is impossible to determine whether the problem had persisted beyond the age of developmentally appropriate drooling, nor is the severity of drooling reported. Therefore, to date, there are no studies that have systematically evaluated the presence and severity of drooling preoperatively and postoperatively in the same cohort.
Thus, despite the potential deleterious impact that the macroglossia may have on psychosocial development, feeding, and drooling, there have been no systematic studies investigating outcomes in these areas. It is therefore the aim of this preliminary investigation to describe the preoperative and postoperative psychosocial, feeding, and drooling outcomes of children with macroglossia associated with BWS and to determine the effect of TRS on these areas.
Method
Participants
The sample consisted of a consecutive series of five boys and five girls with a genetically confirmed diagnosis of BWS, who were recruited and underwent TRS at Great Ormond Street Hospital (GOSH), London, United Kingdom, between 1996 and 2003.
This cohort has been previously examined in a study documenting oral-motor and speech outcomes following TRS in children with BWS (Shipster et al., 2006). All participants were native English speakers. Ethical approval was obtained for the study from the Research and Development Committee for the Institute of Child Health and Great Ormond Street Hospital for Children NHS Trust; the ethic approval number was 02-NS-02.
Procedure, Data Collection Points, and Age at Data Collection
A clinical protocol systematically used for patient evaluation in the GOSH craniofacial clinic was used for data collection across the participant group. Although the children are seen for regular clinical appointments, for the purpose of the present study, data are reported from the following three time points only:
Time 1 (T1): at the preoperative assessment, which occurred at 0 to 3 months prior to surgery. The age of the participants ranged from 8 months to 4 years and 9 months (4;9), with a mean of 2;6 years and a standard deviation of 1;3 years. The purpose of this assessment was to establish a baseline evaluation prior to surgery.
Time 2 (T2): at the postoperative assessment, which occurred at 3 months following surgery. The age of the participants ranged from 11 months to 5;0 years, with a mean of 2;10 years and a standard deviation of 1;3 years. The purpose of this assessment was to evaluate changes following surgery when sufficient time had occurred for healing to be complete.
Time 3 (T3): at the long-term postoperative follow-up assessment. This was most recent clinical evaluation following surgery. The age of the participants ranged from 4;6 years to 11;5 years, with a mean of 6;5 years and a standard deviation of 2;3 years.
The age at TRS and the surgical technique performed were documented from the medical notes. The age at surgery ranged from 0;9 months to 4;9 years, with a mean of 2;7 years and a standard deviation of 1;3 years. The time between surgery and T3 ranged between 1;8 years and 6;8 years, with a mean of 3;8 years and a standard deviation of 1;7 years. One of two tongue reduction techniques was performed: (1) anterior wedge excision (AWE) or (2) keyhole (KH) reduction. The AWE procedure entails a pie-shaped wedge being removed from the anterior of the tongue, and the incision edges are sutured together. The KH procedure involves a midline elliptical excision combined with the AWE, and the incision edges are sutured together in a straight line. Gestational age was also recorded. Seven participants (1, 2, 3, 4, 6, 7, 10) were born prematurely, with one of these falling into the severely premature category of <27 weeks (participant 10). Participant 10 also had comorbid cerebral palsy. See Table 3 for participants' individual ages at the three assessment time points, age at surgery, type of surgery performed, and gestational age.
Biographical Information of the 10 Participants With Beckwith-Wiedemann Syndrome *
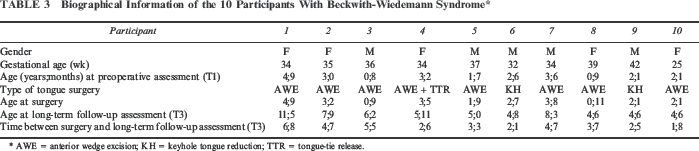
AWE = anterior wedge excision; KH = keyhole tongue reduction; TTR = tongue-tie release.
Procedure
The outcome measures and analysis methods used in the study are reported below.
Psychosocial
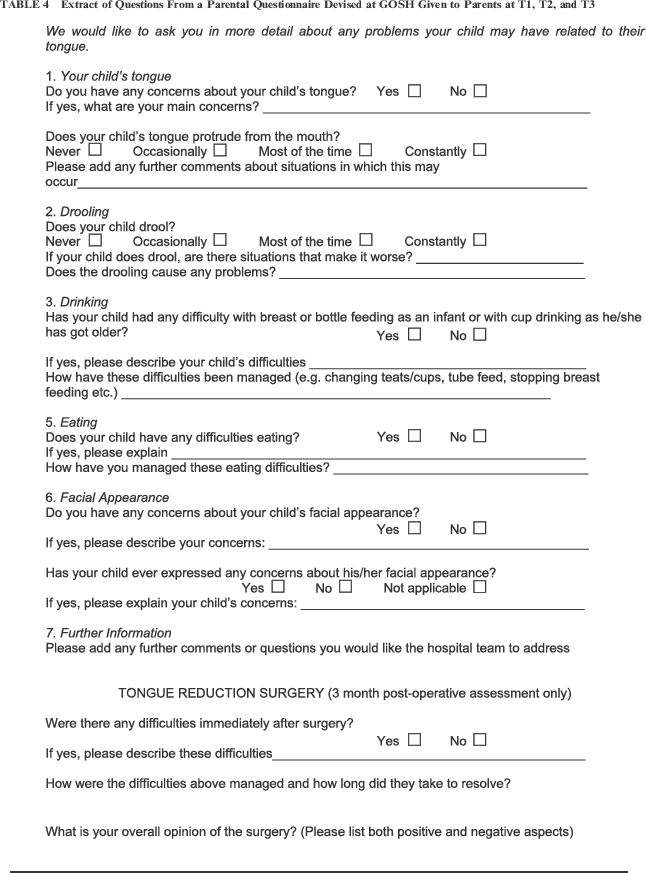
Questionnaires were administered to parents preoperatively and at the routine follow-up assessments postoperatively. The questions asked of the parents are given in Table 4. All responses made by parents on the questionnaires were evaluated to identify common themes at the three time points as follows:
T1: Parental comments regarding the cosmetic and functional impact of the macroglossia
T2: (a) Positive outcomes of surgery, (b) negative outcomes of surgery
T3: Parental comments regarding cosmetic and functional outcomes
Extract of Questions From a Parental Questionnaire Devised at GOSH Given to Parents at T1, T2, and T3
Feeding and Drooling
Feeding assessment
A feeding history was obtained via the medical records and parental report. This included factors of early feeding development (e.g., breast- and bottle-feeding), transitional feeding milestones (e.g., self-feeding and cup drinking), and a history of gastrointestinal, respiratory, or behavioral issues associated with feeding. See Table 5 for difficulties reported. A systematic evaluation of the oral preparatory, oral, and pharyngeal phases of feeding using an informal checklist of eating and drinking abilities was carried out at the three assessment points. This documented the key characteristics of the oral preparatory phase (e.g., presence of consistent lip closure without any anterior spillage, presence of efficient and coordinated mastication), oral phase (e.g., presence of efficient and coordinated posterior propulsion of the bolus through the oral cavity without oral residue remaining), and pharyngeal phase (e.g., presence of cough, choke, or signs of pharyngeal discomfort). Children were assessed using a range of foods and fluids that were part of each child's normal diet that the parents had been asked to supply at the three assessment points. The parental psychosocial questionnaire also documented feeding difficulties preoperatively and associated changes in feeding postoperatively.
Summary of the Key Eating Features at the Three Assessment Points
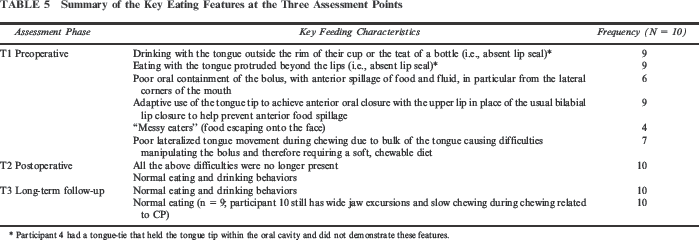
Participant 4 had a tongue-tie that held the tongue tip within the oral cavity and did not demonstrate these features.
Drooling assessment
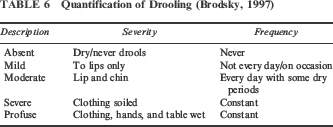
A parental report of the history of drooling was documented in addition to the use of a structured rating scale. Drooling was evaluated in functional terms using an adapted nonstandardized quantification scale originally devised by Brodsky (1997), which had been modified from Crysdale and White (1989). Adaptations to the Brodsky (1997) version of the scale included minor terminology adaptations. Five categories are used on this adapted scale in terms of severity and frequency of drooling (Table 6). A parental interview was used to rate the participants on this scale. Clinical observation was made of the participants during the assessment both at rest and while carrying out a free-play table-top activity to rate the drooling. The degree and frequency of open-mouth posture was also noted as this structural problem may be contributing or causing the saliva management difficulties in this group. The parental psychosocial questionnaire also documented the presence of drooling preoperatively and associated changes in drooling postoperatively.
Quantification of Drooling (Brodsky, 1997)
Interrater reliability scoring
The feeding and drooling assessments were video-recorded at each time point. The videotapes were later reviewed and analyzed independently by the principal investigator and another speech and language therapist to provide interrater reliability scores for the drooling scale, feeding checklist, and the degree and frequency of open-mouth posture.
Results
Psychosocial Outcomes
The psychosocial outcomes for the children are reported below in key themes as outlined in the methodology.
T1: Parental Comments on the Cosmetic and Functional Impact of the Macroglossia
All of the parents reported that their main concern regarding the macroglossia was the negative effect it had on the child's appearance. Nine of the 10 participants' parents concluded that the large protruding tongue and its effects were taken negatively as a visible indication that there was something wrong with their child, for example, stating that people had questioned whether their children had learning difficulties or a particular condition such as Down Syndrome. The three most frequent reactions included people staring at their child in public places, people making comments about the tongue's protrusion or size, and being asked to provide an explanation for the cause of the enlarged tongue. One parent commented, “She gets a lot of stares as her tongue is always hanging out and she dribbles constantly. Some strangers have asked me why it is sticking out or if she has Down's syndrome.”
Parents also reported their concerns about potential future negative effects in terms of appearance such as the child being unattractive to others, having to deal with teasing, or being self-conscious or unhappy about his or her appearance.
All voiced concerns regarding the functional impact of the macroglossia, and these included drooling, restricted tongue movement, and eating problems. A smaller percentage of parents reported that their child frequently bit his or her tongue (3 of 10).
In relation to potential future negative effects, all parents were concerned about the effect of the macroglossia on speech and the structure of the jaws and teeth. All parents sought information as to what to expect both cosmetically and functionally if they opted for surgery or if their child remained unoperated.
T2: Key Themes as to Positive Outcomes of Surgery
All 10 participants' parents stated that the most positive outcome of the surgery was the change in the child's facial appearance as the tongue was no longer protruding. Examples of parents' positive views regarding their children were as follows: “She looks completely normal,” and “He's really handsome now.”
All parents had also noted the positive reactions of close family and friends and commented that in society in general, people reacted to their children normally. Examples of parents' quotes regarding these findings included, “Other family members and close friends have commented on the improvement,” “Nobody made comments about his tongue any more, and he gets less reaction from strangers as to his appearance.” The parents of the oldest child (aged 5 years at T2) reported that she was more confident and outgoing since the surgery had taken place.
In addition to improvements in cosmetic appearance, parents also noted that functional difficulties such as the drooling and feeding problems noted preoperatively were either markedly reduced or no longer present. A further positive outcome was that the children no longer bit their tongue. Although not commented on presurgically, the parents of four children reported that their child snored less at night and slept more peacefully following surgery. Parents of six of the children commented on the improvement in speech production.
T2: Key Themes as to Any Negative Outcomes of Surgery
All parents reported an increase in the quantity of drooling immediately postoperatively, but this did subside within 2 weeks. Parents of four participants felt that the recovery from surgery had been uncomplicated and rapid. However, in the other six cases, some negative outcomes were reported in the short term (i.e., 2 to 3 weeks following surgery): The surgery made eating and drinking difficult, the children experienced pain and soreness, and the children had some healing difficulties. Examples of comments by the parents included the following: “She was upset that she could not drink from her bottle for a few days following surgery because it hurt when she tried to suck the bottle,” and “It was distressing how he looked when he came back from theatre.”
The parents acknowledged that these were short-term issues and overall were pleased that the surgery had been conducted.
T3: Parental Comments Regarding Cosmetic and Functional Outcomes
All parents had positive opinions about their child's outcomes from TRS. All stated that their children's appearance had been normalized by the operation, providing quotes such as, “He looks just like any other child,” and “He looks completely normal.”
Some parents perceived their child to be more attractive after the surgery, for example, “She's a really pretty little girl now,” “He looks very handsome,” and “He's gorgeous.”
All reported that they no longer had comments from others about the tongue, with the exception of two parents stating that they had received comments on the thickness of the tongue.
Feeding and Drooling
Interrelater Reliability Scoring
There was 100% agreement on the degree and frequency of open-mouth posture, 95% agreement for the feeding assessment, and 80% agreement for the drooling assessment. Items of disagreement were viewed again simultaneously until a consensus was reached.
Feeding Outcomes
Six participants had a history of difficulties. The following features were reported: constant protrusion of the tongue beyond the lips during bottle-feeding; poor anterior lip seal around the teat for bottle-feeding; difficulties sustaining prolonged coordinated sequences of suck, swallow, breath; and anterior spillage of milk from the lip corners. Colic was frequently reported. Once solids were introduced, there was anterior spillage of puree during the oral phase and difficulty propelling the bolus posteriorly during oral transit in order to trigger a swallow. Participant 10, born prematurely at 25 weeks, was fed via nasogastric tube for the first 5 months and then successfully transferred to a normal diet. All children had been referred to a speech and language therapist specializing in dysphagia for management of these difficulties. In all six cases, the difficulties were managed effectively with adaptive techniques, and there was no history of failure to thrive.
Key feeding characteristics at the three assessment points are outlined in Table 5. There were no episodes of choking or coughing noted during the presurgical feeding assessments of the children, clinically indicating nil pharyngeal-phase difficulties. Postoperatively, and at subsequent longer-term follow-up, drinking and feeding difficulties related to the previous macroglossia-associated problems were no longer present. All children were able to achieve lip closure around the teat of a bottle/rim of a cup and spoon.
Drooling Outcomes
In relation to drooling history, all parents reported that their children had experienced severe constant drooling as infants/toddlers. Parents reported that their children wore bibs throughout the day and/or frequent changes of clothing were required to keep their children dry. At T1, all children experienced drooling with a range of severity seen across the group (two mild occasional, four moderate constant, and four severe constant). At T2, drooling was no longer present in five children. The frequency and severity of the drooling were reduced and rated as mild and occurring occasionally for four participants and moderate and constant for participant 10, who had cerebral palsy. Of further note, two children within this group were infants aged between 11 months and 14 months, where some degree of drooling is age appropriate.
At T1, all participants had a consistent open-mouth posture at rest. At T2, they continued to maintain an open-mouth posture, but to a lesser degree than at T1, despite the fact that the tongue was no longer protruding over the lip margins. However, lip closure was achieved during production of bilabial sounds and was achieved around the teat of a bottle/the rim of a cup and a spoon. Lip closure was occasionally observed at rest during the swallowing of saliva. At T3, all children had appropriate mouth and lip closure, apart from participant 10, who had slight open-mouth posture and mild perioral wetness.
Discussion
Tongue reduction surgery is advocated in the literature for children who have macroglossia associated with BWS, in order to overcome the secondary effects of the macroglossia, which include feeding, drooling difficulties, and an altered facial appearance. This was the first study to systematically examine these outcomes preoperatively and postoperatively in the same cohort and was the first to examine psychosocial outcomes in this group.
Psychosocial Outcomes
All parents reported a range of concerns about the impact of the macroglossia on their child's facial appearance, which included their perception that their child's looks were adversely affected, the negative reaction of others to their child, and their fears for their child's future. The parental belief that children with facial disfigurement are likely to be at a psychosocial disadvantage is a frequently reported finding in other studies of children with facial disfigurements (Noar, 1991; Hunt et al., 2007; Berger and Dalton, 2009).
Following TRS, however, parental report of psychosocial outcomes was overwhelmingly positive. Of particular note, all parents reported the normalization of facial appearance and improvement or resolution of the functional difficulties related to the macroglossia postoperatively. Parental satisfaction with surgical outcome following TRS has not hitherto been reported in previous studies of BWS. Indeed, all parents reported that they were pleased their children had the surgery, despite the short-term difficulties that ensued. This consecutive cohort represents the first 10 children attending our unit for TRS. As a consequence of parental feedback on the outcomes, changes have occurred in presurgical counseling. The children and their families receive preparation and support for the difficulties that may arise following surgery, specifically for this procedure. All the parents requested information on the long-term outcomes if their children underwent surgery or remained unoperated. The need for information about the condition to reduce parental anxiety and stress and management techniques for the functional difficulties that may arise are well documented in the literature for other groups with facial disfigurement such as cleft lip and palate (Young, 2001; Knapke et al., 2010; Berger and Dalton, 2011).
Feeding Outcomes
The entire cohort had feeding difficulties, and this finding concurs with other studies reporting the presence of feeding difficulties preoperatively (Elliot and Maher, 1994; Weng et al., 1995; Van Borsel et al., 1999; Kacker et al., 2000). Prior to the surgery, a consistent profile of feeding impairment during the oral preparatory phase was noted, characterized by persistent tongue protrusion throughout bottle/cup drinking and spoon feeding and difficulty manipulating the bolus. These feeding patterns are consistent with Rizer et al. (1985), who provide the only comment as to the nature of the difficulties in this population presurgically.
Furthermore, while children were unable to manage firmer textures preoperatively, they were able to manage all textures following surgery, and there were no ongoing concerns for feeding. The reduced bulk of the tongue as a consequence of TRS, reducing its length and width, is likely to have facilitated improvements in the ability to eat, in particular by enabling lip closure, creating enough space for the tongue to lateralize during eating, and enabling enhanced posterior propulsion of the bolus. Lateral tongue movements are an essential component of rotary chewing, facilitating the child's ability to manage a normal diet including challenging consistencies such as meat. All changes in feeding patterns occurred without direct intervention for feeding difficulties in the first 3 months following surgery. This marked change in feeding function postsurgery indicates that the presurgical feeding issues were due to the macroglossia disrupting the feeding process rather than being consistent with a neurological profile. This is an important observation as there were a number of children in this cohort who were born preterm and who may have potentially had neurologically related feeding difficulties.
This is the first study to provide a detailed description as to the nature of the feeding difficulties preoperatively and to report that the problems are effectively eliminated following surgery. These are significant data that can be used to highlight to parents during presurgical counseling that there are positive outcomes for feeding after surgery. None of this cohort had a history of failure to thrive, which is in contrast to one report in the literature (Salman, 1988) that cites this as a problem for children with BWS who have unoperated macroglossia. In the present study, children who presented with early feeding problems had received input from a speech and language pathologist who specialized in dysphagia management, thereby possibly helping to prevent failure to thrive from occurring in our cohort. The management had consisted of recommending a modified diet and selecting different feeding utensils (i.e., changing the shape and flow of the teat to suit the child's needs). In addition, parents were advised to modify their child's diet immediately postoperatively due to the pain and edema that occurs following surgery, but no direct intervention was provided. The parents gradually introduced more textured foods as the children recovered. Such support is an important component of care, and children with macroglossia should be routinely monitored for feeding difficulties presurgically and given feeding management advice following surgery.
Drooling Outcomes
All of the children had a history of severe constant drooling as infants and toddlers even when they were not teething. The reported history and findings of the study indicate that young children with macroglossia have an increased rate and severity of drooling than that which would be expected in normally developing young children. Our findings are consistent with other reports of increased drooling in children with unoperated macroglossia (McManamny and Barnett, 1985; Rizer et al., 1985; Vogel et al., 1986; Elliot and Maher, 1994; Murthy and Laing, 1994; Van Borsal et al., 1999). The two oldest children in the study had mild occasional drooling at the time of the preoperational assessment and no co-occurring neurological impairment that would contribute to the drooling. This finding suggests that although children with macroglossia improve their ability to control their secretions as they get older, drooling can be an ongoing problem for children with unoperated macroglossia.
Apart from an initial increase in drooling during the initial postoperative recovery period, by 3 months postsurgery, drooling was no longer present in five children and there was a marked reduction in the frequency and severity of drooling for the remaining five children. This improvement so soon after surgery suggests that TRS is effective in reducing drooling and is in agreement with other reports (Siddiqui and Pensler, 1990; Wolford and Cottrell, 1996). Open-mouth posture is documented as a contributory factor in the presence of drooling (Van De Heyning et al., 1980); therefore, it is perhaps obvious that once the structural problem of macroglossia is ameliorated, the child can finally achieve mouth closure and lip seal and hence prevent spillage of saliva from the mouth.
At 3 months postoperatively, all children still had a degree of inconsistent open-mouth posture. Taken together with the young age of some of the children, these factors are likely to explain the mild occasional drooling observed in four children. No drooling was observed at long-term follow-up, with the exception of the child with cerebral palsy who had mild inconsistent drooling. The presence of drooling in children with cerebral palsy is well documented (Van De Heyning et al., 1980; Lespargot et al., 1993; Gisel and Alphonce, 1995) and thus unlikely directly related to BWS. The remaining nine children no longer demonstrated drooling. This improvement in saliva management may have been in relation to the children being able to consistently achieve lip closure at this time point.
Limitations of the Present Study and Future Research Directions
A key limitation of the present work is the small number of participants included in the sample. This research should be expanded upon in the future to examine a much larger cohort of children to confirm whether these findings are replicable and generalizable to a larger proportion of children with BWS who undergo surgery. Two different surgical techniques were performed on the children in this study with no differences in outcome between the two procedures. Again, a much larger sample is needed to statistically determine whether there are different outcomes for the techniques used.
Another unavoidable limitation in this instance is the use of nonstandardized rating scales for examining drooling and feeding. Some standardized tools exist to examine feeding function, but these are typically for limited age ranges only, and no standardized tool was available to cover the wide age range required for our present population. It is also critical to note that this issue of poor or absent psychometric data for drooling and feeding tools exists across the field of speech and language pathology and is not a problem specific to this study nor to the population of children assessed here. Finally on this point, each child acted as his or her own individual control in that the same assessments were administered at all three time points, with the key question being whether change occurred for drooling and feeding function before and after surgery.
Conclusion
This was the first study to systematically describe the pre-TRS and post-TRS psychosocial, feeding, and drooling characteristics of children with macroglossia associated with BWS. It expanded on a previous article reporting on speech and oral-motor characteristics in this group. This preliminary study provided evidence for a distinctive profile of deficits associated with macroglossia in BWS across all three domains. Specifically, in relation to psychosocial outcomes, the visibly enlarged tongue had a negative effect cosmetically. There are distinctive feeding difficulties, including poor anterior containment and posterior propulsion of food and fluid and increased drooling preoperatively. TRS and the amelioration of tongue protrusion resulted in functional improvements in all areas immediately postsurgery (i.e., as rapidly as 3 months post-TRS), with some skills (e.g., drooling) taking slightly longer to show complete amelioration, which was eventually witnessed at the longer-term follow-up. Most importantly, in terms of overall prognosis, findings suggest that TRS has a positive impact on psychosocial, feeding, and drooling outcomes for children with macroglossia associated with BWS.
Footnotes
Acknowledgments
The authors are extremely grateful to the families who participated in this study. They also wish to thank Richard Scott, Hannah Goudge, and Jane Benton who contributed to the manuscript preparation. Angela Morgan is supported by National Health and Medical Research Council grant 607315.