
Abstract
Objective
This study was conducted to review the changes in airways after maxillary anterior advancement by distraction osteogenesis in patients with cleft lip and palate.
Materials and Methods
Several electronic databases were searched. The selection criteria were set to include clinical trials and at least 1 year of postsurgical data. The original articles were then retrieved and evaluated by two investigators to ensure that they met the selection criteria. The references were also hand searched for possible missing articles.
Results
Forty-three abstracts were found in the electronic searches. After the first set of selection criteria was applied to these abstracts, 14 articles were retrieved. After the final selection criteria, only four articles were finally selected. However, sample sizes of the selected articles were small, and the methodological quality of the studies was inadequate. All selected articles were consistent in that upper airway sizes increased and nasal resistance was reduced after distraction osteogenesis.
Conclusions
Despite the consistency of increasing the upper airway size and reducing nasal resistance in the only four found articles, limitations of the studies merit caution in interpreting these findings. We conclude that there are insufficient prospective randomized controlled clinical trials to confirm these results.
Distraction osteogenesis (DO), first described for orthopedic surgery, is an essential technique for treatment and management of several craniofacial deformities by oral surgeons and orthodontists (Polley and Figueroa, 1997). The technique of DO takes advantage of the development of bone that occurs when an osteotomized segment of bone is slowly moved, allowing new bone formation within the gap (Ilizarov, 1990). The gradual and incremental separation of bone segments is facilitated by the application of an appliance (internal or external), producing continuous bone formation parallel to the direction of distraction (Snyder et al., 1973). Historically, this technique was initially used to lengthen long bones; however, the principles have been applied to the treatment of craniomaxillofacial deformities (McCarthy et al., 1992). In addition, the surrounding tissue appears to adapt to this gradual tension, producing adaptive changes in all surrounding tissues, including muscles, tendons, nerves, cartilage, blood vessels, and skin. Because the adaptation involves a variety of tissue types in addition to bone, this process has also been called distraction histogenesis (Crago et al., 2003).
It has been suggested that DO offers several advantages over conventional orthognathic surgeries in the treatment of patients with cleft lip and palate (CLP). There are at least two advantages in maxillary DO over conventional orthognathic surgery in subjects with CLP. First, the soft tissue is remodeled in harmony with the hard tissue. This may counteract relapse of the maxillary bone more effectively than conventional surgical intervention. Second, the maxilla can be moved forward to a greater extent than what can be obtained by orthognathic surgery. The greater anterior displacement of the maxilla may induce more dramatic changes in the upper airway structure and function, including an enlargement of the upper-airway caliber and a reduction in airway resistance.
DO relapse is the piecemeal recurrence of the abnormality that the distraction was intended to correct. Relapse associated with DO has been an area of extensive research, owing to its multifactorial etiology (Grassmann et al., 1990; Simmons et al., 1992; Yen, 1997; Davies et al., 1998; Taylor and Stal, 1998; Mobarak et al., 2001). The occurrence of relapse is influenced by several factors that can be related to either the patient or the surgical procedure. Patient-related factors include gender, preoperative mandibular plane angle (Arnett and Tamborello, 1990) degree of advancement, and presence of pre-existing temporomandibular joint dysfunction. Surgery-related factors include fixation type and condylar positioning (McDonald, 1990; Longaker and Siebert, 1996; Gateno et al., 2005; Bartlett et al., 2006; Jayade et al., 2006). Some of these factors can be controlled, but some obviously cannot.
However, only a few studies have investigated morphological and functional changes in the upper airway longitudinally in subjects with CLP who underwent maxillary DO (Ko et al., 1999). In these previous studies, the authors demonstrated longitudinal changes in velopharyngeal function by measuring cephalometric parameters at the level of the palate (Harada et al., 2002). Velopharyngeal function depends on three-dimensional (3D) movements of the velum and pharyngeal walls and has an important role in speech. In patients with cleft palate, palatal repair is performed during infancy primarily to close the cleft palate and to attain normal velopharyngeal function. It is therefore important to study how the stability of velopharyngeal function after palatal repair is related to growth-associated changes in the nasopharyngeal characteristics such as the posterior maxilla, pharyngeal depth, and velar length (Satoh et al., 2004).
Although many comprehensive reviews on the applications of craniofacial DO have been published, neither respiratory function nor cephalometric measurements of upper airway variables below the soft palate were evaluated in these studies. Also, it is unclear from the current literature, regardless of the fact that maxillary DO can lead to soft tissue expansion, whether DO can lead to improvement of airway. Therefore, the objective of this study was to systematically review the evidence in the current literature regarding the possible changes in airways after maxillary anterior advancement by DO in cleft palate patients as evaluated cephalometrically.
Materials and Methods
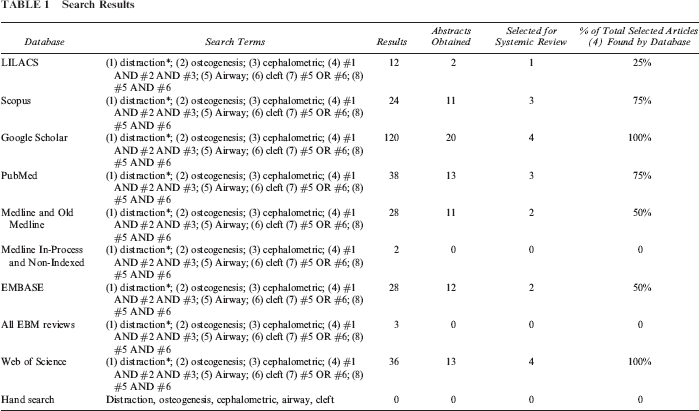
A computerized database search was conducted using Google Scholar (all available articles until week 4 of January 2011), LILACS (all available articles until week 4 of January 2011), Scopus (all available articles until week 4 of January 2011), Old Medline (1950 to 1965), Medline (1966 to week 4 January 2011), Medline In-Process and Other Non-Indexed Citations (up to week 4 of January 2011), PubMed (1966 to week 4 of January 2011), Embase (from 1988 to 2011, week 4), Web of Science (1945 to week 4 of January 2011), and all EBM reviews (Cochrane Database of Systematic Reviews, ACP Journal Club, DARE, and CCTR) up to January 21, 2011. Terms used in the literature search were distraction, osteogenesis, cephalometric, airway, and cleft. The selection and specific use of each term with their respective truncation, if applicable, inside every database (Table 1) were performed with the help of a senior librarian specializing in health sciences database searches.
Search Results
The following inclusion criteria were chosen to initially select potential articles from the published abstract information: human clinical trials or series of consecutively treated cases (no individual case reports), follow-up for 1 year or more, and no postsurgical complications.
Figure 1 presents the flowchart of the searching and selection procedure of the abstracts/articles. Interexaminer agreement was performed as follows: The selection process was followed independently by two researchers (H.S. and T.E.), and their selection results were compared to settle discrepancies through discussion. Cohen's kappa coefficient, a statistical measure of interrater agreement for qualitative (categorical) items, was used to evaluate the selection process. It is generally thought to be a more robust measure than simple percentage agreement calculation, since κ (Kappa coefficient equation [Fig. 2]) takes into account the agreement occurring by chance (Brennan and Prediger, 1981; Siegel and Castellan, 1992; Randolph, 2005). Figure 2 shows Kappa scores. The following provides a detailed explanation of how the Kappa score was calculated: number of articles initially retrieved, 43; number of categories, two (to be included versus not to be included); and number of raters, two (H.S. and T.E.). Pr(a) is the relative observed agreement among raters, and Pr(e) is the hypothetical probability of chance agreement, using the observed data to calculate the probabilities of each observer randomly saying each category. If the raters are in complete agreement, then κ = 1. If there is no agreement between the raters (other than what would be expected by chance), then κ ≤ 0. Thus, the observed percentage agreement is Pr(a) = (14 + 28)/43 = 0.98. In calculating Pr(e) (the probability of random agreement), we note that (1) reader S.H. said “Yes” to 15 applicants and “No” to 28 applicants. Thus, reader S.H. said “Yes” 35% of the time. (2) Reader T.E. said “Yes” to 14 applicants and “No” to 29 applicants. Thus, reader T.E. said “Yes” 33% of the time. Therefore, the probability that both of them would say “Yes” randomly is 0.33∗0.35 = 0.12, and the probability that both of them would say “No” is 0.65∗0.68 = 0.44. Thus, the overall probability of random agreement is Pr(“e”) = 0.12 + 0.44 = 0.56. So now, applying our formula for Cohen's Kappa, we obtain κ = (0.98 - 0.56)/(1 - 0.56) = 0.95
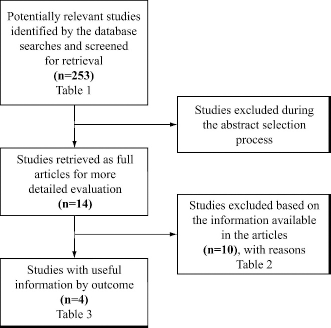
Flow diagram.
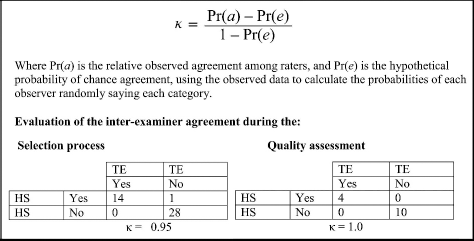
Kappa score calculation for interexaminer agreement.
In evaluation of the interexaminer agreement of the quality assessment, the number of selected articles was 14, the number of categories was two (to be included versus not to be included), and the number of raters was two. The same above steps were followed, and a Kappa score of one was obtained.
If the abstract did not provide sufficient information on which to base a sound decision, then the actual article was obtained to ensure that all possible available studies were considered. Any abstracts that did not specifically mention the time of follow-up were automatically included at this stage as well. The articles ultimately selected were chosen with the following additional inclusion criteria applied to the full article: only cases in which measurements were taken soon after the surgery and then again 1 year or more after surgery. Because of the severity of the CLP deformity and limited number of cases treated with DO, randomization and blinding were considered unattainable. Although higher methodological studies were lacking, case studies were not included in the articles selected for final evaluation.
Reference lists of the selected articles were also hand searched for additional relevant publications that may have been overlooked in the database searches. In cases in which specific data were necessary for the discussion and were not specified in the article, efforts were made to contact the authors to obtain the required extra information.
Results
From the database searches, a total of 43 different abstracts were initially retrieved. The details for the searches, as well as the number of abstracts selected from each database produced, are given in Table 1. Of the 43 abstracts, only 14 articles were retrieved after the first set of selection criteria were applied. Once the final selection criteria were applied on these 14 articles, only four articles were finally selected. No articles were found during the hand searches of the reference lists of the selected articles that did not appear in the electronic database searches.
Comparing the database results, Web of Science had the greatest diversity of finally selected abstracts (100%). The other databases obtained significantly fewer finally selected abstracts (<50%). The different databases repeated most of the abstracts.
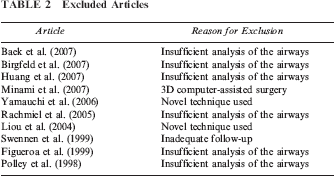
At the final selection stage, from the 14 potential articles, a total of 10 were excluded. One because of an inadequate follow-up period (Swennen et al., 1999), six because there was insufficient analysis of the airways (Polley and Figueroa, 1998; Figueroa and Polley, 1999; Swennen et al., 1999; Rachmiel et al., 2005; Baek et al., 2007; Birgfeld et al., 2007; Huang et al., 2007; Minami et al., 2007), one because of 3D computer-assisted surgery, and two because a novel technique was used (Liou et al., 2004; Yamauchi et al., 2006). Table 2 provides details about the reasons why these 10 articles were excluded at this stage.
Excluded Articles
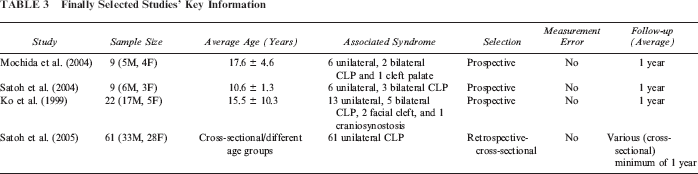
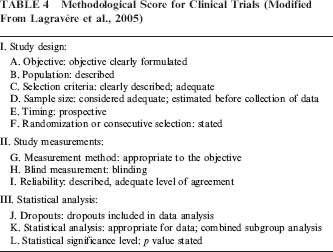
Finally, only four articles that met all of the inclusion criteria remained. Table 3 summarizes the sample size, follow-up period, and associated syndrome or condition for each selected article. A methodological quality checklist developed to evaluate the selected articles is shown in Table 4, and an application of the methodological quality checklist is illustrated in Table 5.
Finally Selected Studies’ Key Information
Methodological Score for Clinical Trials (Modified From Lagravère et al., 2005)
Methodological Score of Selected Articles ∗
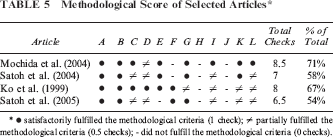
• satisfactorily fulfilled the methodological criteria (1 check); ≠ partially fulfilled the methodological criteria (0.5 checks); - did not fulfill the methodological criteria (0 checks).
Figure 2 gives a detailed explanation of how the Kappa score, used to evaluate interrater agreement, was calculated. In the Kappa scoring system, if the raters are in complete agreement, then κ = 1. If there is no agreement between the raters (other than what would be expected by chance), then κ ≤ 0.
A score of .95 for interexaminer agreement during the selection process means that there is very high agreement (error is statistically insignificant) between the two readers (H.S. and T.E.), with an error of less than 5%. The two readers differed only on the inclusion of one abstract retrieved by the searching mechanism. The disagreement was settled via obtaining the article, which has clearly settled the dispute in favor of not including the article based on the above-mentioned criteria. A score of 1 for interexaminer agreement of the quality assessment means complete agreement from the both authors on which articles are to be included in the final systematic review.
Discussion
It has been widely accepted in the literature that DO can improve skeletal and soft tissue expansion in the affected bone and surrounding tissues. To better understand the interaction between the changes in the upper airway and function in CLP following DO, we have carried out this systematic review. To the best of our knowledge, only a few studies have compared the structure of the craniofacial skeleton, distracted length, and articulation in association with DO (Cohen et al., 1998; Guyette et al., 2001). It has been shown that subjects with upper-airway obstruction gained airway sufficiency after DO in the mandible (Cohen et al., 1998; Denny et al., 2001; Perlyn et al., 2002.)
Nevertheless, there is little information available on how maxillary DO alters the upper-airway structure. Warren et al. (1969) reported that nasal resistance in subjects with CLP is 20% to 30% higher than that in age-matched non-CLP subjects. Hairfield and Warren (1989) reported that there are dimensional and physiologic differences in the nasal airway between surgically repaired subjects with CLP and individuals without CLP.
In this study, we systematically reviewed the changes in airways after maxillary anterior advancement by osteodistraction in CLP patients using cephalometric evaluations.
As discussed, velopharyngeal function involves three dimensions of the posterior and lateral pharyngeal walls and the vellum and therefore velopharyngeal function should be assessed three dimensionally.
However, in all of the four studies selected for inclusion in this systematic review, velopharyngeal morphology was assessed using lateral cephalometric films. Lateral cephalograms provide two-dimensional data in the midsagittal plane. From the morphological viewpoint, velar length and pharyngeal depth are crucial factors influencing velopharyngeal closure. Pharyngeal depth is the distance between the posterior end of the hard palate and the posterior pharyngeal wall at the level of the velopharyngeal closure. Mochida et al. (2004) reported that the anteroposterior dimension of the superior part of the upper airway increased and nasal resistance decreased in association with maxillary distraction osteogenesis. They also found that the decrease in nasal resistance in subjects with CLP who underwent maxillary DO was significantly correlated with the increase the upper airway. This suggests that there is a critical relationship between the gradual change in upper airway and function. Although the sample size was small (nine patients) and the studied patients were not similar in CLP deformity, their results suggested that maxillary advancement by DO was stable after 1 year. This study lacks control individuals as they compared variables before and after treatment for each subject without comparing their results to non-DO CLP patients or to healthy individuals. Also, as the authors mentioned in their discussion, another limitation of that study was that nasal resistance measurements were not performed at the same time the cephalometric radiographs were obtained.
Therefore, it might be hard to draw a conclusion about the correlation between cephalometric changes and nasal resistance; consequently, a solid conclusion about airway improvement and stability may be questionable.
Satoh et al. (2004) also studied airway changes in nine CLP patients treated by DO. Regardless of the fact that the sample size was small, it was not also homogenous, as three patients presented with bilateral CLP and six patients presented with unilateral CLP. The postsurgical records were taken 3 months after surgery, which does not reflect long-term stability of the reported results.
The authors used the ratio of velar length to pharyngeal depth to assess changes in the airway, and their findings showed a small but consistently significant increase in velar length. This suggests the importance of the velum in closing the pharyngeal depth. Again, this study did not have control subjects to enable the researchers better to draw a conclusion between DO and velopharyngeal function changes.
Ko et al. (1999) also reported an increase in the nasopharyngeal depth and velar angle; however, the values obtained were not statistically significant. Satoh et al. (2005) have shown that irrespective of the different patterns of growth-related changes in morphological characteristics, adequate ratios derived from velar length and pharyngeal depth, which have profound effects on velopharyngeal function, indicated that the relation between these two variables in the cleft group was as well balanced as that in the control group. The shorter velar length in the cleft group may compromise velopharyngeal closure. The posterosuperior position of the posterior maxilla, resulting in reduced pharyngeal depth, was suggested to have a compensatory role in facilitating velopharyngeal closure.
Although not the objective of this study, Ko et al. (1999) assessed changes in speech that accompany the maxillary anterior advancement by osteodistraction in cleft palate patients. This is helpful in giving an insight into how DO affects function. They showed that for articulation (as experienced by an experienced speech pathologist), most patients had improved 57%, 28% remained the same, and 14% showed an increase in articulation errors.
On the other hand, orthognathic surgery comprises several surgical procedures that allow the repositioning of the entire midface, mandible, and the dentoalveolar segments to their desired locations. These procedures are carried out as isolated osteotomies or in various combinations. The surgical procedures that reposition the facial skeleton alter the soft tissues that are attached to the bone in order to produce the facial changes. The orthognathic surgical movement of the jaws will result in positional changes of the structures directly attached to the bone and changes in the tension of the attached soft tissue and muscle. The differences between maxillary advancement by orthognathic surgery and distraction osteogenesis on speech and velopharyngeal status were previously addressed.
Chanchareonsook et al. (2006) conducted a review to study the impact of maxillary advancement by orthognathic surgery and distraction osteogenesis on speech and velopharyngeal status based on the literature of the past 30+ years. Thirty-nine published articles on the effect of craniomaxillofacial osteotomies and distraction osteogenesis on speech and velopharyngeal status were identified and analyzed. A total of 747 cases of cleft and noncleft patients were selected, which included craniofacial deformities and syndromes mainly involving maxillary hypoplasia. Their review showed that there was no clear difference in outcome between distraction and conventional orthognathic surgery. They concluded that none of the 39 reviewed studies compared conventional orthognathic surgery and distraction by including both groups in a single study and that randomized controlled trials with an adequate number of subjects and follow-up duration are needed.
In summary, there are few published long-term studies on the stability of changes in airways after maxillary anterior advancement by osteodistraction in cleft palate patients. All of the selected studies are of not high methodological quality (i.e., inappropriate design, small sample size, insufficient presentation of sufficient anatomic landmarks). Based on the limited evidence found, it can be suggested that velar length to pharyngeal depth increases following DO.
From the viewpoint of morphology, velar length and pharyngeal depth are crucial factors influencing velopharyngeal closure (function). High-quality clinical trials are needed to obtain more conclusive results and to evaluate the correlation between the long-term and short-term changes in airways after maxillary anterior advancement by DO in cleft palate patients and other variables such as associated syndromes, amount of distracted bone, patient age and gender, technique, and amount of distraction.
Our systematic review of the various databases has shown that there are only four articles meeting the inclusion criteria of (1) human clinical trials or a series of consecutively treated cases (no individual case reports), (2) follow-up for 1 year or more, and (3) no postsurgical complications. It is worth mentioning that the inclusion criteria for this systematic review are not as rigorous as in other systematic reviews of long-term stability following DO in CLP patients (Al-Daghreer et al., 2008); for example, a follow up of 3 years or more rather than just 1 year should give a better insight into the long-term stability of the changes in airway in CLP following distraction osteogenesis.
Conclusion
Despite the consistency of increasing the upper airway size and reducing nasal resistance in the only four found articles, we conclude that there is lack of evidence in this specific field of research in the form of higher-quality clinical trials (prospective, randomized controlled clinical trials) regarding the long-term effectiveness of DO with CLP patients in increasing the upper airway size and reducing nasal resistance.
Higher-quality clinical trials (prospective, randomized controlled clinical trials) are needed to obtain more conclusive results and to evaluate the correlation between the long-term and short-term stability of changes in airways following DO in CLP patients and the other variables such as associated syndromes, amount of distracted bone, patient age and gender, technique, and amount of distraction.
Footnotes
Acknowledgments.
This work was made possible through the generous Canadian Institute of Health Research (CIHR) Health Professional Research award.