
Abstract
Objective
To review available published literature in order to obtain a more comprehensive assessment of the association between infant mortality and oral clefts, overall and isolated.
Design
A wide-ranging search of published studies relating infant mortality rates to oral clefts and congenital malformations was conducted, yielding applicable data sets. Settings of the included studies varied to a limited extent, although all were conducted within high-income countries with superior health indicators. These results were tabulated and meta-analyzed. Random effects odds ratios comparing each data set with its respective population have been used to account for differing settings and specific infant mortality rates.
Results
Nine articles with relatable data were included in these meta-analyses. The calculated odds ratio of infant mortality associated with oral cleft cases, including those with associated malformations, was substantial: 9.466 (95% confidence interval, 6.153 to 14.560). Excluding oral cleft cases with associated malformations, the odds ratio, although lower, was still significant: 2.073 (95% confidence interval, 1.390 to 3.092).
Conclusions
Compared with the overall population, infants with oral clefts have nine times the odds of dying within the first year of life. Furthermore, even without additional malformations, infants with oral clefts are still twice as likely to die before 1 year of age. Current research points to a substantially higher relative risk of infant mortality among oral cleft cases in developing countries. Additional research is essential to determine the sources of these raised infant mortality rates and possible interventions to decrease them.
In recent decades, infant mortality has decreased substantially around the world (Centers for Disease Control and Prevention [CDC]–Office of Minority Health and Health Disparities, 2011). During this time, though, infant mortality due to congenital malformations has proportionally increased (Berry et al., 1987; Rosano et al, 2000). Cleft lip and/or cleft palate, also known as orofacial clefts or oral clefts (OCs), is one of the most common congenital anomalies, affecting approximately 1 in 700 infants (Mossey and Castillia, 2003). The term oral cleft is defined as a range of disorders affecting the lips and oral cavity (Mossey et al., 2009). It is always inclusive of, and in nearly all considered publications has been limited to, cleft lip and/or cleft palate. Thus, OC will be used here synonymously with cleft lip and/or palate.
Over the past 60 years, there have been several studies conducted to evaluate the infant mortality rate (IMR), the standard percentage of infant deaths (at 1 year of age or younger) or the number of deaths of infants under age 1 per 1000 live births, of OC cases. In these studies, additional congenital malformations have been reported to play a major role in mortality rates of infants with OCs. The objective of this paper is to review and compare the individual results of these studies in order to consolidate the available information on the subject and develop a metaanalysis with more robust statistics on the IMRs associated with inclusive OC cases, which include all infants with cleft lip and/or palate, and isolated OC cases, which exclude those with additional malformations.
Method of Literature Search
The literature search and overall evaluation for this metaanalysis has been compiled in line with the guidelines described in the PRISMA guidelines for reviews and meta-analyses (Moher, 2009). Studies published in English and available through MEDLINE, JSTOR, standard Google search, and follow-up exploration under key words cleft, orofacial, infant mortality, death, congenital anomaly, malformation, and craniofacial were considered in this review. This broad search yielded more than 600 publications, only 14 of which were found to have specific data on mortality rates in OC cases. In order to have relatable data among all of the studies included in this meta-analysis, eligibility criteria were formed to limit studies to only those with explicit data specifically regarding infant mortality in cleft cases. Publications that did not have a follow-up period and accompanying data on the entire first year of life were not included. Similarly, studies including deaths occurring after the first year of life were excluded. No publications were excluded due to the date of the study. Furthermore, the eligibility criteria also limited reviewed studies to those of liveborn infants. Studies inclusive of still births were excluded or, when possible, subtracted from the reported figures.
Nine of the 14 studies met our eligibility criteria (see Table 1). Two studies were excluded for presenting data on only perinatal and neonatal mortality in cleft cases, and three others were excluded for including OC case deaths occurring after 1 year of age. As mentioned, no study was excluded for its study period, and our analysis incorporates studies conducted across a 60-year time frame, 1943 to 2005. No appreciable variation in relative IMR of OC cases was observed across this time. Furthermore, odds ratio (OR) statistical analysis has been used in this review to also reflect the significantly decreasing IMRs of the background population during the period of concern. Also to note, although the eligibility criteria did not limit the location of the studies, the localities of those available on the topic are all high-income countries with superior health indicators (the United States, Denmark, and the United Kingdom) (World Bank, 2010). These results, therefore, only reflect the relationship of IMRs and OCs in developed, advanced economic settings comparable to the included study countries.
List of Included Articles and Study Characteristics *
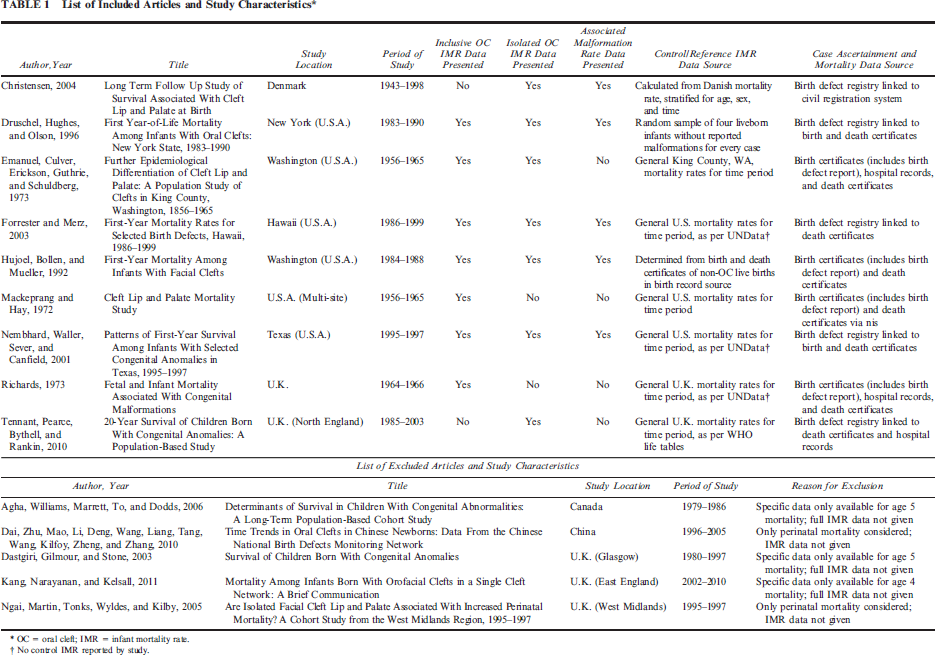
OC = oral cleft; IMR = infant mortality rate.
No control IMR reported by study.
Throughout the included studies, several data collection methods and sources were used to identify study participants, and often multiple sources were used within the same study to corroborate findings, diagnoses, birth and death dates, and related details. The data collection sources are listed in Table 1. Comparison of birth and death certificates alone is traditionally viewed to be the least reliable (Druschel et al., 1996a), but in favor of comprehensiveness, no study has been excluded on the basis of method of information ascertainment.
The data from the nine selected studies, extracted from the tables and text of the publications, were then divided up by OC case type. Seven studies on the infant mortality of inclusive OC cases were included. Five of these included separate data for the etiologically distinct subtypes cleft palate (CP) and cleft lip with or without cleft palate (CL±P) (Mossey et al., 2009), and only one further broke down CL±P data into the subtypes cleft lip (CL) and cleft lip and palate (CLP).
Increased IMRs have been observed in OC infants affected with additional major birth defects, including malformations, syndromes, and sequences. As defined by the CDC, a major birth defect is any structural anomaly that adversely affects health, development, or functional ability. For example, clubfoot would be considered a major malformation, where as a single transverse palmar crease would not (CDC, 2011). For this reason, isolated OC cases, which are those infants without additional major birth defects, have been considered separately. Seven studies were found to include specific data on the IMR of isolated OC cases, five of which also contained inclusive OC data, which has been used in the inclusive IMR analysis. Of these seven, five presented select data for the isolated subtypes CL±P and CP and two provided specific IMR data for CL and CLP cases. Separate analyses of the IMRs associated with classifications OC, CP, and CL±P have been conducted for both inclusive OC cases and isolated OC cases.
Method of Statistical Analysis
After consolidating the data, the collected results were tabulated and aggregated according to OC type and study, with inclusive OC data presented in Table 2 and isolated OC data in Table 3. These tables include all available breakdowns of the data by OC type (i.e., CL/P, CP, CL±P, CLP, and CL). Reported case IMRs were then compared with reference population IMRs. When explicitly stated, the reference population IMR printed in the study was used. Otherwise, the average reference population IMR was calculated according to United Nations (UN) data for the study country during the study time period in consideration (UNData–UN Statistics Division, 2010). Table 1 lists the reference population IMR source used for each study.
Study Results: Infant Mortality Associated With Inclusive Oral Cleft Cases *
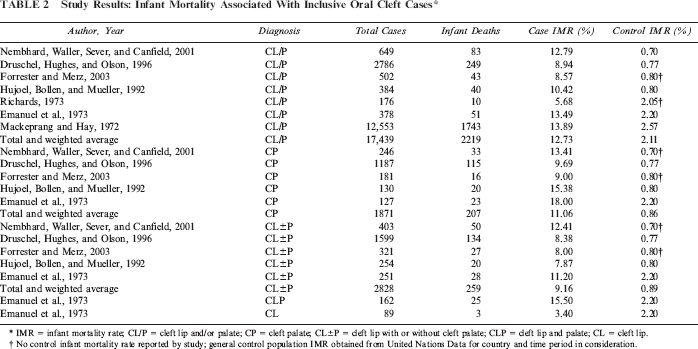
IMR = infant mortality rate; CL/P = cleft lip and/or palate; CP = cleft palate; CL±P = cleft lip with or without cleft palate; CLP = cleft lip and palate; CL = cleft lip.
No control infant mortality rate reported by study; general control population IMR obtained from United Nations Data for country and time period in consideration.
Study Results: Infant Mortality Associated With Isolated Oral Cleft Cases *
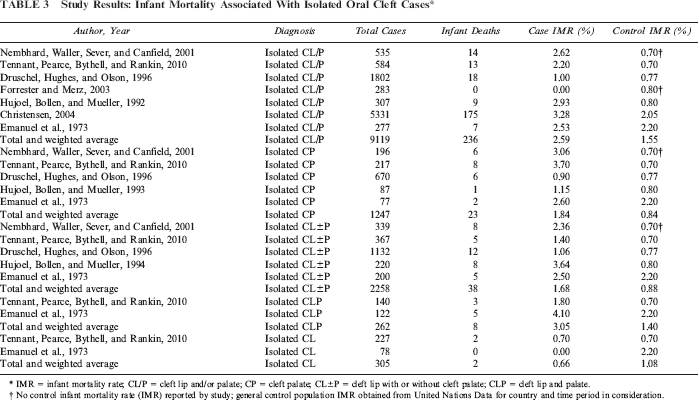
IMR = infant mortality rate; CL/P = cleft lip and/or palate; CP = cleft palate; CL±P = cleft lip with or without cleft palate; CLP = cleft lip and palate.
No control infant mortality rate (IMR) reported by study; general control population IMR obtained from United Nations Data for country and time period in consideration.
The individual sets of collected IMR data for each OC type were then meta-analyzed, comparing observed mortalities in OC case populations to the calculated mortality figure of a reference population of 1,000,000, based on the respective standard population IMR. The standardized, large reference population ensures reported effects are due to the cleft case group findings. Although it is also possible that potential bias may exist if characteristics such as socioeconomic status, gender, or education level vary between the cleft population and the reference population used, the most precise reference data available has been used to limit this potential biasing factor. Additionally, only two of the studies reported data from actual control group cohorts. This reference population standardization also helps prevent possible biasing against these studies. Due to the differing base IMRs, total ORs are more reliable figures for analysis than the aggregated case IMRs. Random effects ORs with 95% confidence intervals (CIs) were calculated according to the method described by DerSimonian and Laird (1986). Given the heterogeneity of the listed studies and the varied study settings, the random effects total OR has been selected as the most suitable and complete statistical analysis for this review. Furthermore, a formal I2 test for heterogeneity among the meta-analyzed studies also demonstrated a high level of heterogeneity among both the isolated OC and inclusive OC analyses, further supporting the use of random effects total OR (Higgins, 2003). Sensitivity analyses investigating the effects of excluding the highest OR, lowest OR, or both showed unremarkable variance in each case. Internal sensitivity analysis was also performed, examining the effect of excluding studies with specific characteristics (i.e., case ascertainment technique, country of study, study time period, different relative mortality rates). This also revealed no notable variances.
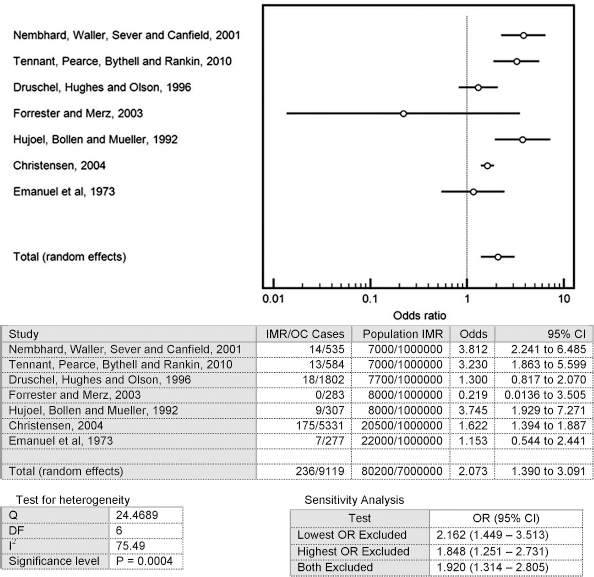
The meta-analyses for inclusive CL/P and isolated CL/P have also been visually represented in forest plots (see Fig. 1). The results of the meta-analyses performed for each subcategory of oral cleft type are listed in Table 4. Studies of IMRs associated with CL and CLP have not been meta-analyzed due to the limited data, but this IMR data is included in Tables 2 and 3.
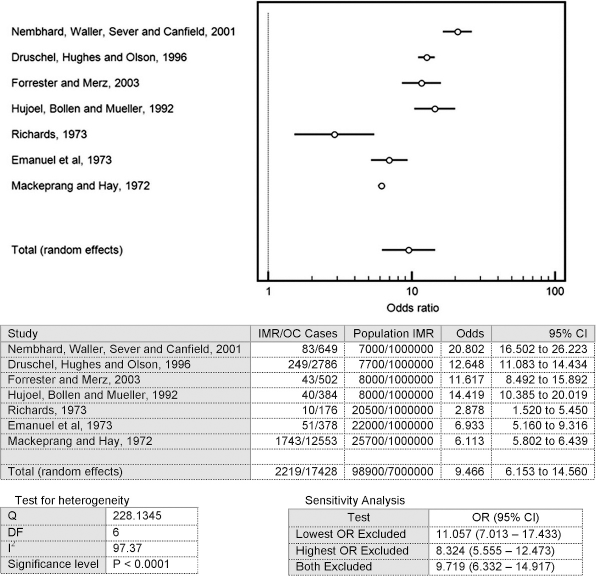
Meta-analysis: IMR of inclusive oral cleft cases.
Total Infant Mortality Odds Ratios for Oral Cleft Cases *
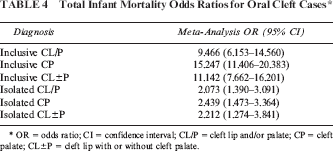
OR = odds ratio; CI = confidence interval; CL/P = cleft lip and/or palate; CP = cleft palate; CL±P = cleft lip with or without cleft palate.
Additionally, due to the significance of associated malformations in the IMRs of oral cleft cases, data on the prevalence of additional malformations in OC cases in the reviewed publications has also been consolidated in Table 5 in order to provide a multifaceted, though incomplete, assessment of this relationship. Statistical analyses were aided by MedCalc for Windows, version 11.3.4 (MedCalc Software, Mariakerke, Belgium).
Study Results: Additional Malformations Associated With Oral Cleft Cases *
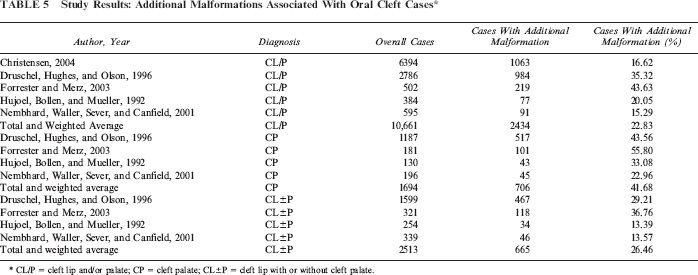
CL/P = cleft lip and/or palate; CP = cleft palate; CL±P = cleft lip with or without cleft palate.
Analysis of Results
Inclusive OC-IMR Studies
According to the published studies considered in this review, the reported IMRs of inclusive OC cases range from 56 to 139 infant deaths per 1000 live births. The weighted average of these IMRs is 12.72%, compared with a weighted average standard population IMR of 2.11% (see Table 2). The meta-analysis yielded a total OR of 9.466 (95% CI, 6.153–14.560; see Table 4). Given the rare outcome in consideration, infant mortality, the OR approaches the relative risk (McNutt, 2003). Therefore, it indicates that infants with OCs in these developed study settings have approximately nine times the risk of dying before the age of 1, compared with the overall populations. These figures have been largely influenced by the Mackeprang and Hay study (1972), which found a relatively high mortality rate but also reported a relatively higher standard population IMR. Among these studies, there was one substantial outlier in the lower end (Richards, 1973). This study by Richards reported an infant mortality relative risk for OC cases compared with the overall population nearly one half the next lowest finding. As previously mentioned, though, the sensitivity analysis showed little effect from excluding the outlying studies.
The studies that included breakdowns of IMRs by OC subtypes consistently showed a higher IMR in CP cases compared with CL±P cases. This was substantiated by the meta-analyses of the subtypes, which generated total ORs of 15.247 (95% CI, 11.406 to 20.382) and 11.142 (95% CI, 7.662 to 16.201) for CP and CL±P, respectively (see Table 4). Similarly, the studies that included data on the percentages of CP cases and CL±P cases with additional malformations consistently presented considerably higher incidence of additional malformations in CP cases (see Table 5). The overall averages from the studies showed that additional malformations were found in 41.68% of CP cases compared with 26.47% of CL±P cases. Neither Mackeprang and Hay (1972) nor Richards (1973) were included in the CP or CL±P analyses, which explains the raised ORs for both CP and CL±P in these analyses.
Only the Emanuel et al. study (1973) presented data divided further into CL and CLP subtypes. Although the case populations considered were small, this showed a much lower IMR in CL cases (3.40%) when compared with CLP cases (15.5%). Additionally, a higher percentage of CLP cases are affected with an additional malformation than CL cases are (Milerad et al., 1997; Harville et al, 2005).
Isolated OC-IMR Studies
Excluding OC cases with associated syndromes and additional major birth defects or malformations, the IMR of isolated OC cases is significantly lower (26 infant deaths per 1000 live births) averaged across the studies. The studies found relatively similar mortality rates in the case populations, although Forrester and Merz (2003) found no mortalities among isolated OC cases. As noted in Table 4, the calculated total OR of infant mortality in isolated OC cases is 2.073 (95% CI, 1.390 to 3.092; see Fig. 2). This shows a significant relationship between isolated OCs and raised IMRs. According to Cohen's rule-of-thumb, this would be classified as a medium-small effect (Chen et al., 2010). Again, given the relatively small probability of the outcome being considered (i.e., infant mortality), the total OR, 2.073, approximates the relative risk of infant mortality for infants with oral clefts. This means that in the developed-world setting of these studies, infants with OCs but no other malformations are approximately twice as likely to die before 1 year of age compared with the overall population.
Meta-analysis: IMR of isolated oral cleft cases.
The studies varied in their findings for IMRs of CP versus CL±P. Overall, the meta-analysis showed a total OR of 2.439 (95% CI, 1.473 to 3.364) for CP cases, which was slightly higher than the total OR for CL±P cases, 2.212 (95% CI, 1.274 to 3.841). Similar to the studies for inclusive OC cases, few data were divided into CLP and CL. Only the Emanuel et al. (1973) and the Tennant et al. (2010) studies broke the data down into these subtypes. They did, however, both show a much higher occurrence of infant mortality in CLP cases (3.05% on average) than in CL cases (0.66% on average).
Discussion
In regard to the inclusive OC cases, this review's results have provided a more complete epidemiological understanding of the IMRs associated with cleft lip and/or cleft palate. Bringing together the available publications on the topic, this review shows a significant odds ratio for infant mortality in OC cases compared with the general population, 9.393 (95% CI, 6.1 to 14.464). As Druschel et al. (1996b) noted, as have other included studies, cleft lip and/or palate is a marker of an at-risk group for infant mortality, usually related to additional congenital malformations and syndromes. The findings here support this claim.
This review also found the IMR associated with CP to be considerably higher than the IMR associated with CL±P. It is likely that this is closely related to the finding that there is a higher chance of infants with CP having additional malformations than those with CL±P.
Cleft lip and/or cleft palate alone is not traditionally viewed as a source of infant mortality (Druschel et al., 1996a). Whether OC cases without associated malformations exhibit an increased IMR has been debated, but this review indicates that these cases likewise exhibit a significantly raised infant mortality rate, with a calculated total OR compared with the overall population of 2.073 (95% CI, 1.390 to 3.092).
It is interesting that the OR for infant mortality associated with isolated CP was slightly higher than that for isolated CL±P as well. Furthermore, in the limited available data, CL cases, both isolated and inclusive, demonstrated exceedingly lower mortality rates than CLP cases. The premise that CL cases do not exhibit increased mortality rates might explain the higher IMR associated with isolated CP compared with isolated CL±P, because CL±P IMRs would be notably lowered by the inclusion of CL. This could also partially account for why inclusive CP cases exhibit higher IMRs than inclusive CL±P, in addition to the theory that this is due to increased probability of CP cases having additional malformations. From these points, it could be inferred that possessing a CL±P is associated with a raised IMR. More extensive research would need to be performed on the IMRs associated with isolated CLP cases versus isolated CL cases to substantiate this theory.
This leads to the next essential question: Why do infants with cleft lip and/or palate, even without additional malformations, face an increased infant mortality risk? What are the underlying causes of mortality in infants with OCs? In regard to OC cases with associated malformations, Christensen and colleagues’ (2004) study of the long-term survival of OC cases investigated the underlying causes of mortality. They found that OC cases had an increased risk associated with all major causes of death, which therefore would suggest that the reasoning for this amplified mortality risk is multifactorial. The highest reported cause of infant death in OC cases was “cleft lip and palate,” which was a somewhat ambiguous category. Upon following up on these cases, 28% of the mortalities were due to pneumonia and bronchopneumonia. Christensen et al. (2004) asserted that one possible cause of increased mortality in OC cases without associated malformations were undiagnosed structural brain anomalies, which would predispose infants with OCs to seizures, another elevated cause of mortality. Certain studies also found excess risk in OC cases for certain cancers, although mostly adult cancers (Zhu, 2002; Bille, 2004), but Christensen and colleagues’ (2004) study did not support this finding. With the increased risk of infant mortality among OC cases, with and without additional malformations, it will be important to accumulate more information on the underlying causes so they can be anticipated and prevented. Several factors need additional research in order to understand not only how often they are associated with OCs but also what role they might play in increased mortality risk. Understanding the specific causes of mortality in infants with OCs will enable health care professionals and organizations to develop enhanced, guided interventions to prevent mortality and lower the IMR overall.
Confounding Factors and Bias
It is important to recognize that several confounding factors and biases, both within the literature review and within the original studies, might have affected this analysis. Methodology and eligibility criteria designed in line with the PRISMA guidelines were formed to control possible systematic biases of the literature review and meta-analysis processes. Issues common to meta-analyses were observed, though. Because the topic is rather narrow with small case populations, only nine usable studies were available and some of these had relatively small data sets, as few as 78 cases when analyzing CL cases alone (Emanuel et al, 1973). This review found these data sets to effectively correspond with one another, though. For example, CP case IMRs were greater than CL±P case IMRs, and raised rates of infant mortality were found in isolated OC cases in all but one small study. By combining the data sets, we were able to generate stronger, more robust statistics on the subject as well as to determine significance that was not necessarily clear previously.
Another issue in this meta-analysis was that these studies were performed on separate populations, although entirely in developed country settings. Random effects ORs were used to balance this concern. Also, the agreement among these data sets illustrates the congruence and comparability among the developed settings of these studies.
One major advantage of this review is that it easily circumvents publication bias (i.e., the “file drawer problem”), a common bias affecting meta-analyses where insignificant findings remain unpublished and therefore overlooked in the review. Unlike other meta-analyses, many of the studies included in this review originally did deem their findings regarding isolated OC cases as insignificant (e.g., Emanuel et al., 1973, and Druschel et al, 1996a), and the significance has only been recognizable by the compilation of these small data sets. Also, several of the articles were not focused mainly on OC case mortality rates but rather on other specific findings (e.g., Richards, 1973, and Tennant et al., 2010). As a result, the effect of publication bias in this review would be minimal.
Various factors might also have confounded the individual studies reviewed here. One point to take into consideration in respect to the reported IMRs, specifically those inclusive of OC cases with additional malformations, is that these rates have likely been artificially lowered by elective pregnancy terminations. Due to the growing capacity of health care professionals to prediagnose congenital anomalies in utero, the practice of elective pregnancy termination for fetuses with major malformations has expanded in recent years and, therefore, has artificially lowered IMRs among populations with congenital anomalies (Bourke, 2005), including nonisolated OC cases. Estimates of the accuracy of the detection rate of CL±P vary widely, from 18% to 75%, although the accuracy of the detection of CL increases when associated anomalies are present (Demircioglu et al., 2008). Because this analysis looks at studies across several decades, it is important to note that there has been a marked increase in the accuracy of detection since the early 1980s. For example, one study found the detection rate of CL±P to be only 5.3% between 1979 and 1988 compared with 26.5% between 1989 and 1998 (Stoll, 2003). It is also important to note that this analysis is inclusive of several studies that were conducted before or concurrently with the point in time when laws legalizing abortion were implemented, specifically 1973 for Denmark, 1967 for the U.K., and 1973 for the United States. This fact combined with the increasing rate of detection by ultrasound may have had some effect on our study. The rate at which mothers choose to terminate a pregnancy after the detection of a cleft varies widely from study to study. Several studies show that without an associated malformation, mothers do not choose to terminate their pregnancies. One review of termination after an isolated cleft diagnosis showed nine studies with rates varying from 0% to 92%, the latter being a clear outlier with the next closest rate of termination being 27% (Johnson and Sandy, 2003). Decisions to terminate a pregnancy after a cleft diagnosis also vary by culture (Johnson and Sandy, 2003). Given the variety of factors that go into making a decision to terminate a pregnancy, such as the existence of laws legalizing abortion, the sensitivity of ultrasound detection, the presence of additional malformations, and cultural values, this inextricably remains a possible confounding factor in this review. Conversely though, an appreciable variation in OC case IMRs was not noted across the wide time period under review, and therefore the effect of this in these studies was most likely minor.
One other possible confounding factor is low birth weight. Several studies have shown an association between OCs and low birth weight, but the correlation between low birth weight and increased risk of mortality specifically among infants with OCs is presently unclear (Lilius and Nordstrom, 1992; Becker et al, 1998; Wyszynski et al., 2003). More targeted research would be necessary to discern any effect of this factor.
In Wyszynski's review of the issues affecting OC studies, he cited the underreporting of associated anomalies in OC cases as another possible confounding factor in OC research (Wyszynski, 2006). It is possible that certain defects have been overlooked in the examinations of OC mortalities—for example, the structural brain anomalies that Christensen et al. (2004) cited as possible factors in mortalities of isolated OC cases. On the other hand, if underreporting of associated malformations were significant, we would expect the IMR related to isolated OC cases to drop substantially across the 60-year time period in consideration, as malformation diagnostic tools progressed. These tools allow health care professionals to better assess whether there was an associated malformation, decreasing the percentage of overlooked additional malformations. Therefore, fewer cases would be misidentified as “isolated OC cases” in later studies, which had hypothetically raised IMR rates in earlier isolated OC research. One would then expect the observed IMRs in isolated OC cases to fall as the time period of the study advanced. This again, however, has not been observed in this review.
As in most retrospective studies, the methods of case and outcome ascertainment in the individual studies allow possible biasing. As listed in Table 1, the studies used different techniques to establish OC case populations and to determine the number of deaths in each population. As previously mentioned, birth certificate reporting is usually the least reliable source for birth defect statistics, as used in the Hujoel et al. study. As this misreporting is assumedly random, though, it is unlikely that this would bias these results. On the other hand, many of the studies (Emanuel et al., 1973; Richards, 1973; Tennant et al., 2010) used hospital records as a data source for OC cases, which might bias studies by omitting infants born outside of hospitals. The actual effect of this, although very small, cannot be determined. Last, unlike following patients across their lifetime, retrospective follow-up techniques, such as exploring a state's death certificates, are susceptible to losing cases over the study period. Because survival is the assumed outcome, this would result in underreporting infant death outcomes. Only Christensen et al. (2004) followed patients across their lifetimes. This, therefore, would likely bias our results, but toward the null hypothesis that IMRs and OCs are not associated.
One shortcoming of this review to note is that the included studies have been performed in similarly developed, high-income settings only. This is because the available published research relating OCs and IMR has been carried out only in high-income countries. Whereas, it made the data from the selected publications more comparable and therefore better suited for meta-analysis, it also considerably limits the generalizability of the results. Some authors have claimed a clear relationship between OCs, regardless of additional malformations, and IMR in the developing world due to feeding difficulties and a higher susceptibility to infection among infants with cleft lip and/or palate (Hodges et al., 2009). With infection and malnutrition being two of the leading causes of infant mortality around the world (Rosano et al., 2000), this seems obvious. Furthermore, risks associated with congenital malformations are amplified in developing-world settings (Rosano et al., 2000).
One large study on this subject has recently been conducted in China (Dai et al., 2010). This study reported that 6.46% of liveborn infants with OCs without additional malformations die within the first 7 days of life (401 early neonatal mortalities of 6206 liveborn infants with OCs). Additionally, 32.15% of liveborn infants with OCs who have additional malformations die within the first 7 days of life (235 early neonatal mortalities of 731 liveborn infants with OCs). This can be compared with a reported 0.37% standard neonatal mortality rate among the total sample population (17,990 mortalities out of 4,843,080 live births). According to this study's findings, cases with isolated CL and CP, compared with the overall population, have a 17.46 relative risk of early neonatal mortality in China.
There is an outstanding need for further research regarding mortality associated with oral clefts in developing countries. More information on raised IMRs in infants with cleft lip and/or cleft palate, as well an understanding of the causes associated with the amplified risk of these conditions, would enable governments and aid organizations to better develop and implement intervention strategies to diminish this risk and in turn lower IMRs throughout the developing world.
Conclusion
Overall, it is clear from our review that persons with cleft lip and/or palate are an infant mortality at-risk group, largely due to the presence of additional malformations, having nine times the risk of mortality in the first year of life than the overall population. Additionally, although their rate is lower than the inclusive OC infant mortality relative risk, infants with isolated OCs also exhibit a significantly increased risk of infant mortality and are approximately twice as likely to die during the first year of life than the overall population. Currently, the causes of this raised mortality rate in isolated OC cases are not fully understood.
Current thought and Dai's study in China point to an even more highly increased IMR among OC cases in the developing world. Conducting additional research in developing countries is critical to provide a more complete picture of the relationship between infant mortality and OCs throughout the world.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Bill Magee, Dr. Randy Sherman, and Dr. Luis Bermudez for their input and advice throughout this review, as well as Ellen Agler, Allison Bradshaw, and Shannon Mintz for their overall guidance and assistance. The authors would also like to offer special thanks to Operation Smile, Inc., for the organization's support during this project.