
Abstract
Objective
Adults with craniofacial conditions experience more psychosocial problems than adults in the general population, but little is known about the factors that render a person more or less susceptible to these problems. Guided by research on adults with other conditions that affect appearance, this study examined predictors of psychosocial outcome in adults with craniofacial conditions.
Design
Single-sample cross-sectional design.
Setting
The Australian Craniofacial Unit, Women's and Children's Hospital, Adelaide, one of the main craniofacial treatment centers in Australia.
Participants
Adults (N = 93; 36.9% of the potential sample) with congenital craniofacial conditions (excluding cleft lip and/or cleft palate) who were treated in the Australian Craniofacial Unit.
Main Outcome Measures
All participants completed measures assessing anxiety, depression, and quality of life (Hospital Anxiety and Depression Scale, Short-Form Health Survey) and variables predicted to affect these outcomes (SF-36 Health Survey - Multidimensional Scale of Perceived Social Support, Rosenberg Self-Esteem Scale, Cleft Satisfaction Profile, Brief Fear of Negative Evaluation Scale, Derriford Appearance Scale).
Results
Multiple regression analyses revealed that anxiety was predicted by social support, self-esteem, and fear of negative evaluation, while depression was predicted by self-esteem and social support. Physical quality of life was not predicted by any of the measures. Satisfaction with appearance, gender, age, and education were not related to outcome.
Conclusions
Interventions designed to increase perceived social support and self-esteem and reduce fear of negative evaluation appear to be indicated and may assist in establishing a causal relationship between these variables.
Craniofacial conditions result from a wide range of congenital malformations that affect the head and facial bones, the most common of which are oral clefts. Even after protracted treatment, craniofacial conditions often result in permanent physical effects that may, directly or indirectly, cause long-term psychological problems. In addition, numerous medical and psychosocial stressors have the potential to adversely affect the health and well-being of adults with craniofacial conditions, including long-term treatment (Lansdown et al., 1997), continuing functional problems, persistent differences in appearance (Chuo et al., 2008), and social stigmatization (Roberts and Shute, 2011).
Possibly related to these stressors is the fact that adults with cleft lip and/or palate (CL/P) frequently report more psychological problems, including elevated levels of social anxiety, social avoidance (Berk et al., 2001), depression, and anxiety, with the latter being associated with appearance-related concerns (Ramstad et al., 1995). Similarly, some aspects of quality of life (e.g., perceived meaningfulness, satisfaction with family life) also appear to be worse in adults with cleft lip and palate (CLP) (Marcusson et al., 2001), with a recent study reporting poorer mental health in adults with CLP (Mani et al., 2010). In contrast, the psychosocial outcomes of adults with other congenital craniofacial conditions are poorly understood, with most studies focusing on CL/P. One of the few studies of adults with noncleft craniofacial conditions (hemifacial microsomia, orbital hypertelorism) reported lower self-esteem, satisfaction with facial appearance, and quality of life compared to adults with minor skin conditions (e.g., moles) (Sarwer et al., 1999). Another study of adults with a broad range of craniofacial conditions reported higher levels of self-esteem but more appearance-related concerns, lower quality of life, and less social support from friends compared to normative data (Roberts and Mathias, 2011). In combination, these findings suggest that adults born with craniofacial conditions are at increased risk for a range of poor psychosocial outcomes.
Despite an increased risk for poor outcomes, researchers have also identified a number of positive aspects of living with craniofacial conditions (Eiserman, 2001; Meyerson, 2001). For example, Eiserman (2001) noted positive outcomes in a number of areas, including a greater sensitivity toward others, ability to move on in the face of challenges, ability to help others, and acceptance of life's challenges; more gratitude for the small things in life; and greater self-determination and sense of purpose in life.
Predictors of Psychosocial Outcome
If adults with craniofacial conditions are more likely to experience psychosocial problems than the general population, the question arises as to whether specific individuals are at a greater risk of developing problems and whether interventions can be devised to improve their outcomes. At present, there is very limited research examining the factors that predict good outcomes in people with craniofacial conditions. Such research should be informed by both general models of adjustment to chronic conditions, which take into account issues relating to disabilities and impairments, as well as specific variables that are relevant to people with craniofacial conditions (e.g., treatment-related stressors, appearance-related concerns). One model of the determinants of health-related outcomes in people with chronic illness and disability is that of Moos and Holahan (2007), who proposed that personal resources (e.g., self-esteem, education), condition-related factors (e.g., severity), social and physical context (e.g., social support), a person's cognitive appraisal of his/her condition, adaptive responses (e.g., managing treatment), and coping skills collectively contribute to a person's health. Rumsey and Harcourt (2005), on the other hand, provided a framework that focuses on outcomes in people with disfigurement in which they identify some of the aforementioned variables (e.g., demographic, peer, and family influences) while also highlighting cognitive processes that may affect outcome (e.g., self perceptions, appearance-related beliefs). Limited aspects of both models have been examined in people with CL/P (e.g., Cochrane and Slade, 1999) but not in a broader group of adults with craniofacial conditions.
While the association between sociodemographic variables, such as education and socioeconomic status, and mental health is now well-established in the general population (Fryers et al., 2005; Akhtar-Danesh and Landeen, 2007; Dalgard et al., 2007), these variables have not been investigated in adults with craniofacial conditions. In contrast, age and gender differences in the psychosocial outcomes of adults with CLP, as well as patients undergoing reconstructive facial surgery, have been investigated (Marcusson et al., 2001; Carr et al., 2005; Moss and Rosser, 2008), with men and older persons having better outcomes. The relationship between the visibility or severity of a craniofacial condition and psychological adjustment has also been examined; however, severity does not appear to predict outcome (e.g., Sarwer et al., 2001).
In terms of the cognitive processes that Rumsey and Harcourt (2005) proposed may contribute to outcome, subjective self-assessments of appearance have been found to predict psychological well-being and social anxiety in adults with clefts (Cochrane and Slade, 1999). Similarly, fear of negative evaluation has been found to be related to quality of life in adults with a skin condition that affects appearance (psoriasis) (Kent and Keohane, 2001), suggesting that this factor may also be relevant to people with craniofacial conditions. There is also evidence for a relationship between self-esteem and depression among adults in the general population (e.g., Schroevers et al., 2003), although the direction of causality continues to be debated (Boden et al., 2008). Moreover, there is evidence to suggest that low levels of social support are related to social anxiety in adults with craniofacial conditions and that social support and self-esteem may protect people from psychological distress (Liossi, 2003). Finally, appearance-related concerns have been found to be related to anxiety and depression in patients with a range of problems affecting appearance (Carr et al., 2005) and are likely to be relevant to adults with craniofacial conditions.
Thus, the model of adjustment to chronic conditions postulated by Moos and Holahan (2007), and the framework provided by Rumsey and Harcourt (2005) for understanding the psychosocial outcomes of people with visible differences in appearance collectively provide guidance as to potential predictors when examining the psychosocial problems of adults with craniofacial conditions. However, existing research has not examined these predictors in people with craniofacial conditions other than CL/P.
Aims of the Study
The current study was designed to identify factors that predict physical quality of life and mental health status (anxiety, depression) of adults with a congenital craniofacial condition, excluding CL/P. More specifically, it was designed to investigate those predictors of psychosocial problems that are most likely to be amenable to intervention to aid in the eventual development of effective psychological interventions. Predictors of quality of life and mental health status were identified, based on existing research and theory, including self-esteem, appearance-related concerns, social support, fear of negative evaluation, satisfaction with facial appearance, and demographic variables. It was predicted that men would have better outcomes, as would participants of older age, higher socioeconomic status, and higher educational levels. In addition, it was predicted that outcome would be positively related to satisfaction with facial appearance, perceived social support, and self-esteem and negatively related to fear of negative evaluation and appearance-related concerns.
Methods
Participants
One hundred eleven adults who had been treated at the Australian Craniofacial Unit, Women's and Children's Hospital, Adelaide, for congenital craniofacial conditions (excluding CL/P) and for whom current addresses were available, were invited via mail to participate in the study. A total of 93 adults (39 men and 54 women) aged from 19 to 54 years (mean = 29.2 years, standard deviation [SD] = 11.4) responded. Participants had a wide range of diagnoses, including Crouzon syndrome (15), coronal synostosis (14), Binder syndrome (9), Treacher-Collins syndrome (6), Apert syndrome (5), metopic synostosis (4), Saethre-Chotzen syndrome (3), primary orthognatic growth disorder (3), Waardenberg syndrome (3), Goldenhar syndrome (3), and 21 other low-incidence craniofacial conditions for which there were a maximum of two cases. Participants were referred to the Unit at an average age of 8.1 years (SD = 9.9), had their first surgery at a mean age of 10.5 years (SD = 11.6), and had undergone up to nine surgical interventions (mean = 2.5, SD = 2.3). Final surgery for the craniofacial condition was completed at an average age of 23 years (SD = 8.2), with 21 patients still undergoing surgical treatment.
Measures
Seven questionnaires examining quality of life, anxiety and depression, self-esteem, appearance-related concerns, satisfaction with social support, social anxiety, and satisfaction with appearance were completed by participants. In addition, information was collected about education and residential area (via postal codes). The latter were used to calculate the Index of Relative Socio-Economic Advantage/Disadvantage (measure of socioeconomic status) (Australian Bureau of Statistics, 2006).
Predictor Measures
Rosenberg Self-Esteem Scale
The Rosenberg Self-Esteem Scale (RSE; Rosenberg, 1989) is a widely used 10-item scale in which participants rate their agreement on a 4-point scale, which ranged from “Strongly agree” to “Strongly disagree,” with items expressing positive and negative self-esteem (e.g., “I feel that I have a number of good qualities”). Low scores indicate high self-esteem (range: 10 to 40). This scale has been used with adults with disfigurement (e.g., Papadopoulos et al., 1999).
Derriford Appearance Scale
The Derriford Appearance Scale (DAS24; Carr et al., 2005) is a 24-item scale that measures body image disturbance (negative affects and impairments in functioning related to body image dissatisfaction) by assessing the frequency of avoidant behaviors and distress related to appearance concerns; it is designed to be used with people with visible differences in appearance. Participants respond to questions, e.g., “How distressed do you get when you see yourself in the mirror/window?” on a 4-point scale, e.g., “Not at all distressed,” “A little distressed,” “Moderately distressed,” or “Extremely distressed.” Higher scores indicate more appearance-related concerns (range: 11 to 96). This scale has high internal consistency, test-retest reliability, and validity in patients with appearance problems (Carr et al., 2000).
Multidimensional Scale of Perceived Social Support
The Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) is designed to evaluate the degree to which participants perceive their family, friends, and significant others to be socially supportive. Participants respond on a 7-point Likert scale that ranges from “Very strongly disagree” to “Very strongly agree” to 12 statements (e.g., “I can count on my friends when things go wrong”). The total score is then divided by 12, with higher scores indicating higher perceived social support (range: 1 to 7).
Brief Fear of Negative Evaluation Scale
The Brief Fear of Negative Evaluation Scale (Brief-FNE; Leary, 1983) is a self-report questionnaire that assesses the central cognitive aspects of social anxiety; namely, the degree to which respondents experience apprehension regarding the prospect of being evaluated negatively in social situations. Participants respond on a 5-point scale (e.g., “Not at all characteristic of me” to “Extremely characteristic of me”) to 12 statements (e.g., “I am afraid that others will find fault with me”). Higher scores indicate greater anxiety about being evaluated unfavorably (range: 12 to 60). This scale has established reliability and validity and has been used with adults with visible disfigurement (Kent and Keohane, 2001).
Cleft Satisfaction Profile
The Cleft Satisfaction Profile (CSP; Thomas et al., 1997) measures a person's cognitive appraisal of their appearance by asking participants to rate four features of their facial appearance (teeth, lip, nose, and profile) on a 7-point scale ranging from “very unsatisfactory” to “very satisfied” (score range: 4 to 28). While this instrument was originally designed for people with CL/P, it is also appropriate for use in persons with other craniofacial conditions.
Outcome Measures
Short-Form Health Survey
The Short-Form-36 Health Survey (SF-36; Ware and Sherbourne, 1992, adapted for Australian use by Sanson-Fisher and Perkins, 1998) is a 36-item measure of health-related quality of life that has well-established reliability and validity in adults with many different health conditions (Ware and Kosinski, 2001). Participants answer questions that assess eight scales: Physical Functioning, Role-Physical (i.e., limitations in usual role activities because of physical health problems), Bodily Pain, General Health, Vitality, Social Functioning, Role-Emotional (limitations in usual role activities because of emotional problems), and Mental Health. The Physical component summary score, which is derived from the Physical Functioning, Role-Physical, and Bodily Pain scales, was used to measure quality of life in this study (Ware and Kosinski, 2001). This summary score was converted to a T-score, which is standardized to have a mean of 50 and standard deviation of 10.
The Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS; Zigmond and Snaith, 1983) is a 14-item scale that measures participants' current levels of anxiety and depression. It was designed for use in populations with physical conditions, has established reliability and validity (Bjelland et al., 2002), and has been used in adults with visible disfigurements (e.g., Martin and Newell, 2004; Rumsey et al., 2004). Participants rated their responses to questions (e.g., “Worrying thoughts go through my head”) on a 4-point Likert scale (e.g., “A great deal of the time,” “A lot of the time,” “From time to time but not too often,” and “Not at all”). Scores on this measure range from 0 to 21 for the anxiety and the depression subscales. Scores of 11 to 21 on the HADS are thought to indicate probable clinically relevant levels of anxiety or depression, while scores of 8 to 10 represent possible clinically relevant levels of anxiety or depression and scores of 0 to 7 represent normal levels of symptoms for each subscale (Zigmond and Snaith, 1983).
Procedure
A total of 253 adults had been treated as children for a congenital craniofacial condition (excluding CL/P) by the Australian Craniofacial Unit, Adelaide, between 1977 and 2008. The Unit did not have a current mailing address for 141 of these adults, and an additional person had subsequently died, excluding them from the study. The Head of the Australian Craniofacial Unit sent the remaining 111 adults a letter introducing the study and seeking their involvement. A package containing a copy of the study questionnaires, an information sheet, and a consent form was posted to participants 2 weeks after the initial letter. Questionnaires and consent forms were returned to the researchers in postage-paid envelopes. Two reminder letters were sent during the next 3 months. The final sample of 93 adults represents a response rate of 83.8% of those for whom there was a current mailing address and 36.9% of all of the adults who were eligible to participate in the study. Six participants who had high levels of anxiety and depression (HADS) were contacted to discuss referrals for support. The craniofacial diagnosis was obtained for the 89 participants who gave written consent for the investigators to access this information from their medical files. All study procedures were approved by the Women's and Children's Hospital Ethics Committee.
Statistical Methods
Comparison with test norms for the SF-36 score was made using a single-sample t test. Preliminary analyses were performed to explore the relationships between the psychosocial predictors, age, and socioeconomic status and the outcome measures (HADS, SF-36) by computing bivariate correlations (Spearman's r). Gender and educational differences in psychosocial outcome were examined using independent-sample t tests and analysis of variance, respectively. A series of three multiple regression analyses were then conducted to establish which variables independently predicted quality of life (physical), anxiety, and depression. Only those variables that were significantly associated with the outcome measures in the preceding bivariate analyses were included as independent variables in the regression analyses. Any gender or age differences in predictor variables were controlled statistically by entering the variable as the first step into all of the regression analyses. No bivariate correlations between independent variables were above 0.66; therefore, the multicollinearity assumptions were met (Field, 2009). A power analysis for a regression analysis with five predictors indicated that for 80% power, an N of 91 and 43 would be required to detect a medium effect and a large effect, respectively, indicating that the current sample was adequate to detect medium or large effects.
Results
Missing Data
In a small number of cases, participants omitted a response to one or more items in a questionnaire. When only one response was missing for a measure, a mean response was substituted (one case for the MSPSS, three cases for the DAS); however, when more than one response was missing, the participant was removed from that particular analysis (see Table 2 for final Ns). Because eight participants had more than one missing item on the SF-36, participants who completed the SF-36 were compared with those who did not. Scores were not significantly different on any measure, except for the HADS Depression score, where participants who completed the SF-36 reported higher levels of depression (mean = 3.72, SD = 4.05) than those who did not complete the SF-36 (mean = 1.57, SD = 1.27) (t[19.23] = 3.30; p = .004). The study participants were compared with those who were eligible but unable to be recruited for this study because current addresses were not available to evaluate the representativeness of the study sample. The only information available for this purpose was gender, as consent was required to access all other records. This analysis revealed a significant difference in gender (chi-square [1, n = 234] = 4.04; p < .05), with a greater representation of women in the final sample.
Background Information
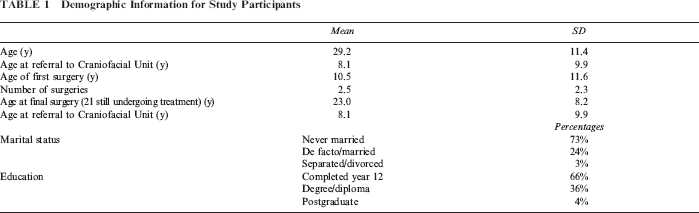
Demographic information is summarized in Table 1, where it can be seen that, on average, the participants were young adults, the majority of whom were unmarried and had finished high school. Most had completed surgical treatment for their craniofacial condition, with only 21 (29%) still undergoing treatment. The socioeconomic status (based on postal codes) of participants was in the middle range of the Australian population (Index of Relative Socio-Economic Advantage/Disadvantage: mean = 5.96, SD = 3.04).
Demographic Information for Study Participants
The age and psychosocial outcomes of the 72 participants who had completed treatment were initially compared with those of the 21 participants who were still undergoing treatment to determine whether there were any differences between these two subgroups. There was no significant difference in the age of participants (all values means ± SDs) (completed 28.2 ± 9.1; not completed 29.9 ± 7.4; t = 0.80, p = .43) or functioning on any of the three outcome measures (SF-36 Physical component: completed 52.4 ± 9.3; not completed 50.9 ± 9.6; t = −0.62, p = .54; HADS Depression: completed 3.8 ± 4.1; not completed 2.7 ± 3.2; t = −1.18, p = .24; HADS Anxiety: completed 6.8 ± 4.1; not completed 6.9 ± 4.9; t = 0.11, p = .91). In addition, with the exception of perceived social support (MSPSS: completed 5.4 ± 1.2; not completed 6.1 ± 0.68; t = 2.90, p < .01), there were also no significant differences between these subgroups on any of the predictor measures (RSE: completed 19.6 ± 6.1; not completed 20.6 ± 6.1; t = .68, p = .50; CSP: completed 20.3 ± 5.2; not completed 20.3 ± 5.9; t = .05, p = .96; Brief-FNE: completed 36.6 ± 10.9; not completed 33.9 ± 11.0; t = −0.97, p = .34; DAS24: completed 40.4 ± 15.3; not completed 35.7 ± 17.1; t = −1.19, p = .24). For social support, participants who had completed their treatments reported lower perceived levels of support than those who had not completed treatment. Thus, the two groups were comparable; the data were therefore combined in all subsequent analyses.
Descriptive Data
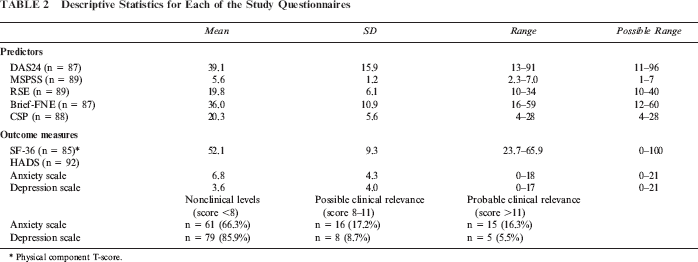
Summary data for the study measures are reported in Table 2. In terms of outcome, the average T-score for the Physical Component of the SF-36 was above the standardized mean of 50 (mean = 52.1, t(84) = 2.04, p = .05). However, nine people (11%) had scores that were 1 to 2 SDs below the standardized mean for a healthy sample, and an additional four people (5%) had scores that were more than 2 SDs below the standardized mean on the Physical score. In addition, 16 (17%) and 8 (9%) participants reported symptoms of anxiety and depression, respectively, which were of possible clinical relevance (i.e., score of 8 to 11). Fifteen (16%) and 5 (6%) participants met the criteria for probable clinical levels of anxiety and depression (score > 11). Previous work by the study authors comparing this sample with the general population showed no difference in the Physical score of the SF-36 and anxiety or depression levels (Roberts and Mathias, 2011; refer to for detailed demographic information).
Descriptive Statistics for Each of the Study Questionnaires
Physical component T-score.
Quality of Life, Anxiety, Depression, and Predictor Variables
A series of independent sample t tests revealed that there were no significant differences in the scores of men and women on the SF-36 (Physical T-scores), HADS, DAS-24, or Brief-FNE. However, women reported higher perceived social support (men: 5.2 ± 1.3; women: 5.8 ± 1.1; t = −2.39, p = .02, d = −0.51) and lower self-esteem (men: 21.3 ± 6.3; women: 18.7 ± 5.7; t = 2.02, p = .05, d = 0.43). One-way between-group analyses of variance, which compared the psychosocial outcomes of groups defined according to their highest level of education (high school year 10, 11, 12; diploma/trade qualification; bachelor degree; postgraduate degree), found no significant differences for any of the measures (SF-36 Physical component, HADS Anxiety and Depression scales).
The relationships between outcome and ratings of satisfaction with facial appearance, perceived social support, fear of negative evaluation, appearance-related concerns, self-esteem and outcomes (physical quality of life, anxiety, depression) were examined (Table 3). The correlations between the outcome measures are also reported, as are the correlations between age, socioeconomic status, and outcome measures. Spearman's rank order (rs) correlations were used because the scores on many of the measures were not normally distributed. Using Cohen's (1992) guidelines, rs = 0.1 equates to a small effect, rs = 0.3 equates to a medium effect, and rs = 0.5 indicates a large effect.
Spearman's Rank Order Correlations Among Study Measures

p < .05;
p < .01.
There were no significant correlations between age or socioeconomic status and any of the measures of psychological outcome (physical quality of life, anxiety, depression) or predictor variables (appearance concerns, self-esteem, social support, fear of negative evaluation, satisfaction with appearance) (Table 3). The physical aspects of quality of life (SF-36 Physical Component T-score) showed significant low-moderate correlations with the measures of appearance-related concerns (negative) and social support (positive). There were moderate to large and significant positive correlations between both the HADS Anxiety and Depression scale scores and measures of appearance-related concerns, self-esteem, and fear of negative evaluation; there were also moderate to large and significant negative correlations between these HADS scores and both perceived social support and satisfaction with facial appearance. Finally, correlations between the SF-36 Physical component and HADS scores generally showed moderate relationships between these measures.
Predictors of Physical Quality of Life, Anxiety, and Depression
Because there were gender differences in social support and self-esteem, gender effects were controlled statistically by entering gender as the first step in the regression analyses. Gender, social support, and appearance-related concerns together accounted for only 3% of the explained variance in physical quality of life (SF-36 Physical component scale T-score) (adjusted R2 = .03, F [3, 76] = 1.81, p = .15) (see Table 4 for results of all regression analyses). In contrast, 52% of the variance in anxiety (HADS) was explained by measures of social support, self-esteem, and fear of negative evaluation (adjusted R2 = .52, F [6, 76] = 15.71, p < .001), and 44% of the variance in depression (HADS) was explained by measures of social support and self-esteem (adjusted R2 = .44, F [6, 70] = 10.96, p < .001). However, for the latter regression, an inspection of the relationship between the residuals and predicted HADS Depression scores revealed a problem with heteroscedasticity; as a consequence, the variance estimates were modified using a generalized estimating equation with robust variance estimate (Table 4). This supported the original finding, also showing that the HADS Depression score was predicted by the measures of social support and self-esteem.
Summary of Regression Analysis for Variables Predicting the SF-36 Physical Component Scale T-Scores and the HADS Anxiety and Depression Scale Scores, Controlling for Gender
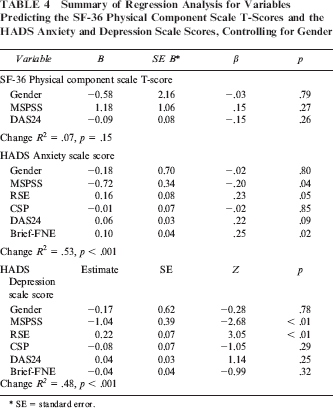
SE = standard error.
Discussion
This study was designed to identify factors that predict quality of life and mental health outcomes among adults with congenital craniofacial conditions by considering a broad range of potentially contributing variables. The findings suggest that the physical aspects of the quality of life (SF-36) were not compromised in this sample and were not predicted by any of the study measures. Of greater concern are the psychosocial problems that were experienced by the participants. More specifically, anxiety levels were lower in people who had higher levels of perceived social support, better self-esteem, and fewer fears of being evaluated negatively, while depression was lower in people who had more perceived social support and greater self-esteem. The fact that there is overlap in the predictors, with social support and self-esteem related to both psychosocial outcomes, supports the possibility that they play a more general role in reducing negative affect. Interestingly, satisfaction with facial appearance, age, gender, education, and socioeconomic status were not related to psychosocial outcomes. These findings provide partial support for two models that were originally developed to identify some of the variables that contribute to adjustment to chronic conditions (Moos and Holahan, 2007) and disfigurement (Rumsey and Harcourt, 2005). While both models suggest that demographic variables (e.g., education, gender) play a role in adjustment, this was not the case for adults with craniofacial conditions. However, a number of other variables that these models identify as important determinants of well-being were found to be significant predictors of mental health outcomes in the current study (social support, self-esteem, and fear of negative evaluation). Unfortunately, neither model makes specific predictions about different aspects of outcome, such as anxiety, depression, or quality of life. Thus, these models still require further refinement. Although a significant proportion of people reported psychosocial problems, it is equally important to draw attention to the resilient larger proportion who reported a good quality of life and good mental health. This is consistent with recent work focusing on the positive aspects of living with a craniofacial condition (e.g., Meyerson, 2001; Roberts and Shute, 2011).
The failure to find a relationship between either age or gender and our measures of psychosocial outcomes contrasts with previous research that has been undertaken in adults who were waiting for reconstructive plastic surgery for congenital or other conditions (e.g., scars from trauma and burns, obesity and weight loss, and facial aging) (Carr et al., 2005). The current findings suggest that, among adults with congenital craniofacial conditions, age and gender do not play a major role in predicting psychosocial outcome. Similarly, the lack of a relationship between educational level or socioeconomic status and psychosocial outcome suggests that there are other more important variables that need to be considered in addressing the psychosocial needs of this population.
The significant role of higher self-esteem and greater perceived social support in accounting for a large amount of the variance in both anxiety and depression is an important finding and is in agreement with previous research establishing a link between psychosocial outcomes and self-esteem and social support (Schroevers et al., 2003; Murphy and Murphy, 2006). The fact that fear of negative evaluation was additionally associated with anxiety is also consistent with research with adults who have other conditions affecting appearance (Kent and Keohane, 2001; Liossi, 2003; Carr et al., 2005).
Participants' satisfaction with their facial appearance was related to all of the psychosocial measures. Consistent with previous research (e.g., Cochrane and Slade, 1999), satisfaction with facial appearance was most strongly related to appearance-related concerns. However, when satisfaction with appearance was considered with other variables, it did not independently predict psychosocial outcomes.
This is one of the largest studies to date to examine predictors of psychosocial functioning in adults with congenital craniofacial conditions and the first study to consider such a range of psychosocial predictors. Despite its relatively large sample size, this study was slightly underpowered to detect a medium effect for the regression analyses using five predictors (N of 91 required for 80% power) but was sufficiently powered to detect large effects. Small sample sizes and low response rates are common problems in investigations of participants with craniofacial conditions. The relatively large number of participants examined here, in comparison to previous work, is therefore a strength of this study. However, the current research was limited by our inability to contact a significant number of eligible participants, with only 36.9% of the potential sample taking part in the study, and our inability to access information other than gender about nonparticipants. Ethical approval for this study did not allow the release of potential participants' names or other identifying information to the researchers until informed consent had been received. As such, no further efforts to contact participants were possible.
A further issue is that several participants did not complete all measures, with eight (8.6%) participants failing to complete the entire SF-36 (i.e., > 1 response missing). Noncompleters reported fewer symptoms of depression than those who completed the SF-36, although there were no significant differences in their scores on other predictor or outcome measures. In addition, this study was limited by its reliance on self-report measures and the use of a cross-sectional design. The latter prevents us from drawing conclusions about the direction of the relationship between predictors and outcome (physical quality of life, anxiety, and depression) variables. It is also important to note that there is a high likelihood of shared method variance in the outcome measures, given the high correlations between the anxiety and depression scales (r = .58). Additional research using a longitudinal design, in which children with congenital craniofacial conditions are regularly followed into adulthood, is needed to address this issue. The current study used a generic measure of quality of life to allow comparison with the only local quality-of-life norms available. Future work should consider using a quality-of-life measure that has specifically been developed for this population (Patrick et al., 2007) to ensure that condition-specific aspects of quality of life are captured. Moreover, future research should also include a measure of income, rather than social advantage/disadvantage, as previous research completed with other populations found that income is related to psychosocial outcome (Pinquart and Sorensen, 2000). Unfortunately, income data were not collected in the current study. Models of adjustment to chronic conditions (Moos and Holahan, 2007) and to appearance concerns (Moss and Carr, 2004; Rumsey and Harcourt, 2005) also suggest that other factors are more likely to predict positive outcomes, including coping strategies and self-concept. Future work should consider the relative importance of these factors in conjunction with fear of negative evaluation, self-esteem, and social support.
While awaiting further evidence, particularly from prospective studies, the current findings serve to identify some potential targets for future interventions that are designed to improve the psychosocial well-being of adults with craniofacial conditions, as well as for interventions that are targeted toward adolescents prior to their transition to adult services. Interventions designed to increase perceived social support and self-esteem and reduce fear of negative evaluation are all indicated on the basis of the current study and would enable an evaluation of the causal role of these variables. While social support is one possible area for intervention, Smith et al. (1994) previously suggested that a good understanding of an individual's needs is necessary prior to implementing an intervention, as some forms of social support can be viewed as negative (e.g., as an invasion of privacy or overdependence). Therefore, a focus on social skills training may be a more useful alternative, with promising results reported in interventions with adolescents (Kapp-Simon et al., 2005) and adults (Robinson et al., 1996) with craniofacial conditions. Moreover, recent research has shown that when youths with a craniofacial condition adopted a set of positive social skills, such as making good eye contact, initiating social interactions, and explaining their craniofacial condition to others, other people's perceptions of them were more positive (Edwards et al., 2011).
Cognitive-behavioral interventions have also been used with people with a range of other disfiguring conditions (Kish and Lansdown, 2000; Bessell and Moss, 2007). Indeed, a number of studies have reported positive mental health outcomes (e.g., improved self-esteem) in these groups when they used interventions that focused on some of the cognitive processes that were identified in the current study as being predictive of poorer mental health outcome (fear of negative evaluation) (Papadopoulos et al., 1999; Kleve et al., 2002). However, despite these promising interventions, a recent systematic review by Bessell and Moss (2007) of the effectiveness of psychosocial interventions for individuals with visible differences concluded that the evidence for these interventions is poor, with only small improvements shown. Interventions that draw on broader models of adjustment and incorporate a more comprehensive range of variables that contribute to psychosocial outcomes may be needed to achieve better treatment effects.
Finally, it is important to remember that the current study did not include persons with CL/P. However, the current findings are largely consistent with research examining factors related to psychosocial outcomes among persons with clefts and suggest that it may be appropriate to consider these groups together, both for research purposes and in the delivery of psychosocial services.
Conclusions
The present results suggest that both self-esteem and social support are significantly related to a range of psychosocial outcomes, with greater fears of negative evaluation additionally being associated with higher levels of anxiety, although whether this is a causal relationship has yet to be determined. This study highlights the importance of considering all of these factors, rather than simply focusing on satisfaction with appearance or sociodemographic variables, when clinicians are working with adults with craniofacial conditions.
Footnotes
Acknowledgments
This study was supported by a grant from the Faculty of Health Sciences, University of Adelaide.