
Abstract
Objective
To assess the outcome of palate lengthening by myomucosal buccinator flaps for velopharyngeal insufficiency both in terms of speech and changes in palate length.
Design
Thirty-two consecutive patients who underwent the buccinator flap procedure were reviewed retrospectively. Palate length and the presence or absence of a velopharyngeal gap were assessed on pre- and postoperative videofluoroscopic recordings using a calibrated image analysis system. Hypernasality, nasal emission, nasal turbulence, and passive cleft type articulation errors were evaluated blindly by a speech-language pathologist external to the team using pre- and postoperative speech recordings.
Setting
Multidisciplinary cleft team based in a tertiary referral center.
Results
In 81% of patients, speech outcome was such that no further velopharyngeal surgery was considered necessary at the time of follow-up. The buccinator flap procedure resulted in a mean palate lengthening of 7.5 mm (±5.5 SD). After the operation, there was a complete elimination of the velopharyngeal gap on lateral videofluoroscopy in 77% of patients. There were significant decreases in hypernasality ratings and passive cleft type articulation errors postoperatively.
Conclusion
Palatal lengthening with myomucosal buccinator flaps in patients with velopharyngeal insufficiency is effective and safe. It has become one of our routinely practiced procedures for velopharyngeal insufficiency.
After primary palate repair, a small but significant percentage of patients present with velopharyngeal insufficiency (VPI) because of insufficient palate length and/or mobility (Grunwell et al., 2000; Sell et al., 2001). Treatment of patients with consistent hypernasality, nasal airflow errors, passive cleft speech characteristics, and/or nasal regurgitation is usually surgical (Harding and Grunwell, 1998). A large number of surgical techniques are described to address VPI. These can be grossly divided into two categories: palatoplasties (aimed at increasing the length and/or the mobility of the palate) and pharyngoplasties (aimed at decreasing the velopharyngeal space) (Rudnick and Sie, 2008). In the North Thames Cleft Service (NTCS), the decision to use a particular technique is tailored to the specific velopharyngeal structure and function of each patient and based on assessment of speech and lateral videofluoroscopic images of the soft palate kinematics. Nasendoscopy is performed if tolerated, usually above the age of 3 years. In cases of consistent VPI with anterior palatal insertion of the levator palati muscle (i.e., an anterior levator knee as imaged on videofluoroscopy), the levator muscle is retropositioned radically under microscopic vision (palate re-repair) as described by Sommerlad et al. (1994, 2002). The rationale for this approach is that levator retropositioning restores normal anatomy, carries very little morbidity such as upper airway obstruction, and is often sufficient to obtain normal speech. In the NTCS protocol, when the levator knee is posteriorly located and insufficient palate length is the primary factor contributing to VPI, then a modified Hynes pharyngoplasty (posterior pharyngeal wall augmentation by transposition of pharyngeal myomucosal flaps) has been the mainstay for surgical treatment (Hynes, 1950). The soft tissue bulge is positioned in line with the point of maximal lift of the soft palate as determined on lateral videofluoroscopy, after division of the soft palate in the midline for surgical access. However, a Hynes pharyngoplasty can be technically demanding if the level of attempted velopharyngeal closure is high in the nasopharynx because of difficult access. Secondly, because it is almost impossible to suture through lymphoid tissue, an adenoidectomy needs to be performed at least 3 months prior to the surgery in cases in which a significant adenoid pad is present at the proposed site of the soft tissue bulge. These considerations have led to a move toward the technique of palate lengthening by buccinator myomucosal flaps in the already described patient groups since 2000. The buccinator flap procedure was also preferred over a Hynes pharyngoplasty when palatal fistulas existed at the border between the hard and soft palate because these can be dealt with simultaneously. Finally, in the presence of excessive scarring in the soft palate, the decision-making was skewed towards the buccinator flap procedure on the hypothesis that breaking up the scar and introducing new tissue in the palate would increase its elasticity.
Though the use of myomucosal buccinator flaps in cleft surgery was first described in 1969 for the primary repair of a wide cleft palate (Mukherji, 1969; for historical overview see Hill et al., 2004), the first report on the use of myomucosal buccinator flaps to lengthen the palate in secondary VPI was published by Hill et al. (2004). The authors described the speech outcome of palate lengthening by bilateral buccinator flaps in 16 patients with VPI after cleft palate repair. Pre- and 6-month postoperative speech audio–video recordings were evaluated blindly by a speech–language pathologist and rated for hypernasality and audible nasal emission. Both parameters improved significantly after surgery, with 87% of patients presenting with normal resonance postoperatively. In 2008, Robertson et al. (2008) described their experience with the addition of a single myomucosal buccinator flap to a palate re-repair in secondary cleft palate surgery in 20 patients with VPI or palatal fistulas. They reported a significant improvement in nasal resonance, nasal emission, and intelligibility, based on a chart review. However, their results are difficult to interpret because of the small number of patients, the absence of a blind, independent speech analysis, and the mixed indication of VPI and fistulas. Most importantly, 50% of their patients underwent additional palatal or pharyngeal operations before the postoperative assessment used for the study, hampering any conclusion about the effectiveness of the buccinator flap. Recently, Mann et al. (2011) published their experience with using bilateral buccinator myomucosal flaps for VPI in a retrospective chart review of 27 patients, describing a postoperative improvement in both resonance and intelligibility. No blind independent speech analysis was performed, and they failed to report the nasal airflow errors of nasal air emission and nasal turbulence.
In this study, we aimed at enlarging the body of evidence for this particular procedure by assessing the outcome of the technique in 32 consecutive patients with cleft-related VPI. We studied speech outcome by independent, blind analysis of pre- and postoperative speech audio-video recordings, and we measured physical palate lengthening and assessed the presence or absence of a velopharyngeal gap on recorded pre- and postoperative lateral videofluoroscopies.
Methods
Patient Selection
The recorded lateral videofluoroscopies and the speech audio–video recordings of all patients who underwent palate lengthening by bilateral myomucosal buccinator flaps for cleft-related VPI between May 17, 2000, and February 7, 2010 were reviewed. The decision to proceed with surgery was based on a speech evaluation by a speech-language pathologist, nasometry, lateral videofluoroscopy, and when undertaken nasendoscopy. Palate lengthening by buccinator flaps was indicated when there was consistent VPI primarily caused by insufficient palate length, in the presence of an unfavorable anatomy for Hynes pharyngoplasty (such as large adenoid pad or sloping posterior pharyngeal wall), a fistula at the junction of the hard and soft palate or excessive soft palate scarring.
The study was conducted in accordance with the principles of the Declaration of Helsinki.
Operative Procedure
All operations were performed by the two senior cleft surgeons (LK and BCS) working in the NTCS between 2000 and 2010. Bilateral myomucosal buccinator flaps were raised on the inside of the cheek, inferior to the parotid papilla (Fig. 1a). The donor sites were closed directly. A transversal incision was then made through the soft palate, close to the junction with the hard palate, pushing the soft palate towards the posterior pharyngeal wall (Fig. 1b). The resulting palatal defect was reconstructed using the buccinator flaps. The first buccinator flap was sutured into the nasal layer of the defect with the mucosa facing the nasal lumen. The second buccinator flap was sutured in the oral layer, with the mucosa facing the oral lumen (Fig. 1c). If posterior molars were present, there was a risk of the patient chewing the pedicle and hampering the flap blood supply. To prevent this, the orthodontist constructed a bite block prior to surgery. The block, made of cold cure acrylic, was constructed on either the maxillary or mandibular dentition and separated the back teeth by at least 4 mm to provide sufficient space for the pedicle. Three weeks after surgery, the pedicles were divided during a short second anesthesia, and the bite block, if present, was removed.
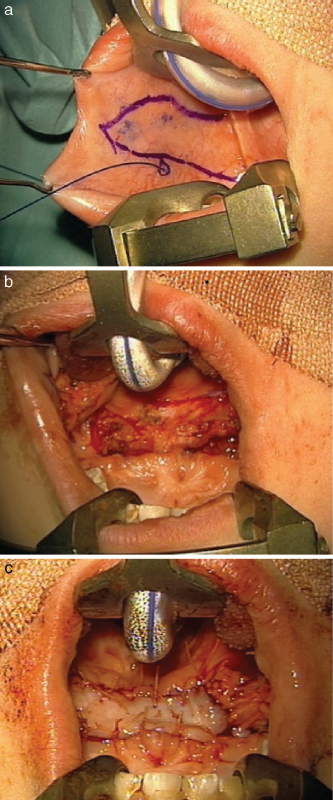
Surgical technique. a: Design of the left-sided buccinator flap with demonstration of the parotid papilla using a prolene suture. b: Transversal incision through the soft palate, close to the hard palate edge. c: View at the end of the procedure, showing the oral buccinator flap sutured in the palatal defect.
Chart Review
A systematic chart review was performed looking at age at surgery, date of surgery, sex, cleft type, diagnosis of a syndrome, previous VPI surgery, revision surgery, and surgical complications. The role of potential prognostic factors (male, age > 7 years, previous VPI surgery, syndromic diagnosis, operation before 2006 [i.e., early in the surgical learning curve], no simultaneous levator retropositioning) in predicting poor outcome (need for revision surgery) was tested.
Blind, External Speech Analysis
High-quality audio-video digital speech recordings were made preoperatively and at least 6 months postoperatively with a Panasonic digital video camera model NV-GS70 and a Rode NT-3 hypercardiod condenser microphone, held in place on a floor stand with the latter positioned approximately 10 to 20 cm away from the subject's mouth. The recordings were edited onto a master DVD in a randomized order (using the website www.random.org). The standardized speech sample consisted of a sample of spontaneous conversational speech when possible, followed by automatic speech and repetition of the UK 16 sentences, using a picture book with the younger patients (Sell et al., 1999; John et al., 2006). When children were unable to repeat sentences, the same picture material was used, but the therapist modeled short phrases and single words using the same target words. The recordings were analyzed blindly by a speech-language pathologist not associated with the NTCS, previously trained in the Cleft Audit Protocol for Speech-Augmented (CAPS-A) protocol (Sell et al., 2009).
The CAPS-A was used for speech evaluation (John et al., 2006). This included noting the presence and severity of hypernasality, hyponasality, audible nasal emission, nasal turbulence, and the frequency of passive cleft speech characteristics (weak and or nasalized consonants, nasal realization of plosives and/or suspected passive nasal fricative, gliding of fricatives/affricatives). The passive error category is usually directly related to the velopharyngeal structure and can thus be directly influenced by surgery (Harding and Grunwell, 1998). Hypernasality was scored on a 5-point scale, with 0 representing normal; 1, borderline; 2, mild; 3, moderate; and 4, severe. Each of these scalar points had a detailed operational definition. Audible nasal emission and nasal turbulence were each scored on a 3-point scale, with 0 representing absence of symptoms; 1, occasional symptoms; and 2, frequent symptoms. Hyponasality was scored on a 3-point scale, with 0 representing absence of hyponasality; 1, mild hyponasality; and 2, marked hyponasality. Passive cleft speech characteristics (CSCs) were scored on a 3-point scale (0 to 2), depending on the number of consonants affected (John et al., 2006). The traffic light color scheme was used to present the results as originally proposed by Harland (1996). John et al. (2006) expanded the definitions of each color category to include both outcomes and future treatment needs.
The red color coding indicates frequent and/or marked occurrence of features indicative of VPI, pointing to a need for investigations and probably surgery. The yellow color coding reflects occasional or mild occurrence of these parameters, requiring monitoring, although hypernasality may indicate the need for velopharyngeal investigations depending on the overall profile. The light and dark green color coding reflects an absence of these parameters, suggesting a satisfactory result.
Five random speech recordings (5 of 26, 19%) were repeated on the master DVD to calculate intrarater reliability. Five random speech recordings (5 of 26, 19%) were rated by a second speech-language pathologist to assess interrater reliability.
Measurement of Palate Length, Velopharyngeal Gap Size, and Palate Extensibility
The length of the palate at rest, velopharyngeal gap size in palatal elevation and palate extensibility were analyzed by the first author from videotapes of preoperative and (at least 6 months) postoperative lateral videofluoroscopies, using a computer-assisted method as described previously (Birch et al., 1994). Palatal length was measured at rest as the length of a straight line between the posterior edge of the hard palate and the uvular apex. The presence or absence of a velopharyngeal gap during maximal velar lift (on producing the sound /i/) was noted. Measurements were made using the software program ImagePro (Media Cybernetics version 6.2, Bethesda, MD).
Ten randomly selected videofluoroscopy recordings (10 of 60, 17%) were measured again by the first author following an interval of 7 months, to calculate intrarater reliability. To check interrater reliability, a second author (MB) also performed the measurements.
Statistics
Pre- and postoperative speech ratings (hypernasality, hyponasality, audible nasal emission, nasal turbulence, and passive CSCs) were analyzed using the Wilcoxon matched-pairs signed rank test. Using a Bonferroni adjustment, the level of significance was set at P < .01. Pre- and postoperative palate length was analyzed using the paired Student's t-test. Differences were considered significant at the P < .05 level. Data are reported as means ± standard deviation.
To assess inter- and intrarater reliability of the speech assessments and the assessment of the presence of a velopharyngeal gap, weighted kappa was calculated. To assess inter- and intrarater reliability of the palate length measurements, an intraclass correlation was used. To assess the value of potential prognostic factors for the need of revision surgery, the Fisher exact test was used.
Results
Patient Characteristics
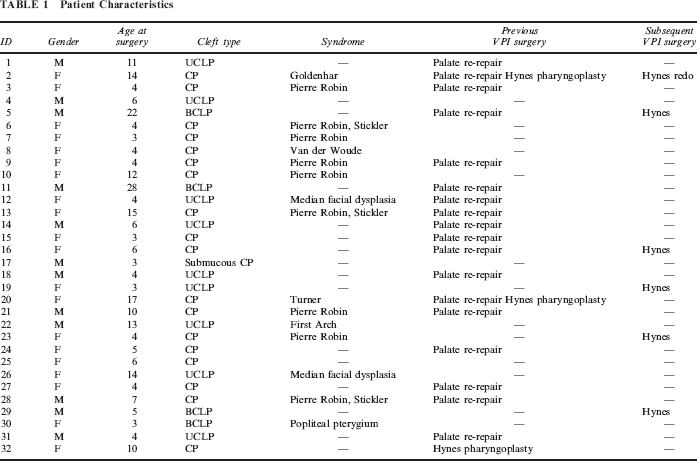
Between May 17, 2000, and February 7, 2010, 37 patients underwent palate lengthening by bilateral myomucosal buccinator flaps for VPI. Five patients were excluded because of incomplete records from missing the postoperative visit. Of the 32 buccinator flap patients included in this study, 12 were male and 20 were female. As shown in Table 1, nine patients were born with a unilateral cleft lip and palate, four with a bilateral cleft lip and palate, 18 with an isolated cleft palate, and one with a submucous cleft palate. Sixteen patients (50%) were diagnosed with a syndrome (including Pierre Robin sequence). All had undergone primary cleft palate repair or submucous cleft palate repair, and 19 (60%) had also undergone palate re-repair for VPI before the buccinator flap procedure. At the preoperative assessment all patients had clinical, videofluoroscopic, and in some cases nasendoscopic evidence of velopharyngeal insufficiency with short palate length identified as the major contributing factor to VPI. The mean age at the time of the buccinator procedure was 8 years, age range 3 to 28 years. Four patients who presented with a combination of short palate length and an anterior location of the levator muscles (patients 1, 13, 17, 23) underwent simultaneous levator muscle tightening and retropositioning during the buccinator flap procedure, and three patients underwent simultaneous fistula repair (patients 1, 12, 30). Postoperative assessments were made on average 9.2 months after surgery (ranging between 5.7 months and 17.2 months). The mean length of subsequent follow-up at the time of the data collection was 4.4 years (ranging between 13 months and 10.2 years).
Patient Characteristics
Palate Measurements
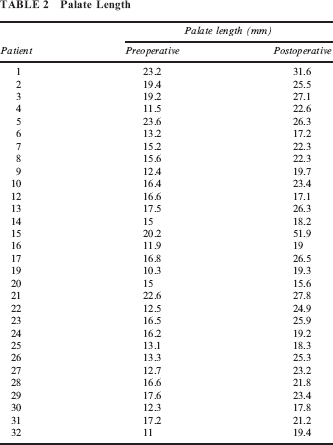
Thirty patients (94%) had sufficiently high quality pre- and postoperative recordings to allow computerized measurements. We measured a mean palate length of 15.8 ± 3.6 mm (range 10.3 to 23.6 mm) preoperatively and 23.3 ± 6.6 mm (range 15.6 to 51.9 mm) postoperatively (P < .0001), indicating that a lengthening of the palate of on average 7.5 ± 5.5 mm (range 0.5 to 31.7 mm) was achieved by insertion of the buccinator flaps (Table 2). Preoperatively, a velopharyngeal gap was visible on lateral videofluoroscopy in 27 of 30 patients (90%), postoperatively in 7 of 30 patients (23%). Intra- and interrater reliability for the measurement of palate length was very good, with an intraclass correlation coefficient of 0.98 and 0.86, respectively. Assessment of the presence or absence of a velopharyngeal gap also demonstrated a high intra- and interrater reliability, with a weighted kappa of 1 and 0.8, respectively.
Palate Length
Speech Results
In 26 patients, both pre- and postoperative speech audio-video recordings were available of sufficient quality for rating. Figure 2 shows the individual CAPS-A color codings for pre- and postoperative hypernasality, nasal emission, nasal turbulence, and passive cleft speech characteristics for all included patients (John et al., 2006). The hypernasality score decreased significantly from a mean value of 2.4 ±1.4 preoperatively to 0.3 ± 0.8 postoperatively (P < .0001). The mean score for audible nasal emission was 0.7 ± 0.8 preoperatively and 0.3 ± 0.6 postoperatively with no significant difference (P > .01). The mean nasal turbulence score was 0.4 ± 0.7 preoperatively and 0.8 ± 0.8 postoperatively (P > .01). The mean score for passive cleft type characteristics decreased from 1.0 ± 0.9 to 0.3 ± 0.6 (P < .01). Surgery had no effect on hyponasality: one patient was noted to have mild hyponasality preoperatively with no hyponasality noted postoperatively (patient 22) and one patient demonstrated mild hyponasality postoperatively where it was absent preoperatively (patient 14). Regarding the intrarater reliability for the speech parameters, a very good strength of agreement was found for parameters of resonance (weighted kappa of 1) and nasal airflow errors (weighted kappa of 0.8) and a good strength of agreement for passive cleft speech characteristics (weighted kappa of 0.69). Interrater reliability showed a good strength of agreement for resonance (weighted kappa of 0.63) and a moderate strength of agreement for nasal airflow errors and passive cleft speech characteristics (weighted kappa of 0.42 and 0.57).
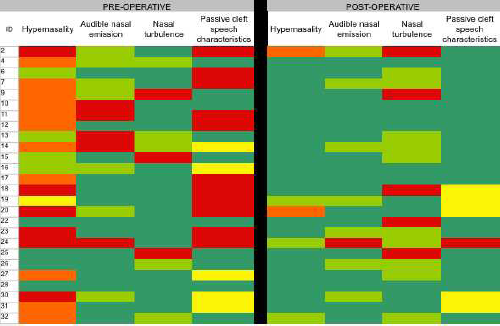
Pre- and postoperative CAPS-A ratings of hypernasality, nasal emission, nasal turbulence, and passive cleft speech characteristics. The “traffic light color scheme” is used (see Methods).
Further speech surgery (Hynes pharyngoplasty) was suggested or performed in 6 of 32 patients (19%) (patients 2, 5, 16, 19, 23, and 29). None of the tested potential prognostic factors (male, age > 7 years, previous VPI surgery, syndromic diagnosis, operation before 2006, absence of simultaneous levator retropositioning) were associated with a higher need for revision surgery (all P > .05). In the interval between surgery and postoperative review, 11 of 32 (59%) patients had significant speech therapy for CSCs, meaning regular therapy, 8 of 32 (25%) patients had minimal speech therapy for CSCs (meaning review only), 2 of 32 (6%) had speech therapy for language problems, and the remainder (10%) did not require speech therapy.
Burden of the Procedure and Surgical Complications
Patients were discharged when feeding was reestablished and when comfort allowed, which was on average 2.5 days after the buccinator flap surgery (minimum 1 day, maximum 5 days). Eighteen patients (56%) had bite blocks fitted. Twenty-eight patients had a second small procedure 3 weeks after the initial surgery to divide the pedicles, and if present, bite blocks were removed. In 73% of patients the pedicle division was performed as a day case, and the remaining 27% were discharged the day after the procedure.
One patient was admitted for a secondary hemorrhage 7 days after the pedicle division, which resolved without intervention. Two patients presented with a small fistula at the hard-soft palate border, which healed spontaneously. One patient needed further pedicle division at the start of orthodontic treatment. Another patient presented with a web to the left cheek, which may need further division in the future. There were no cases of identified flap loss, snoring, or sleep apnea.
Discussion
After the buccinator flap procedure, 26 of 32 (81%) patients required no further speech surgery. Comparing the 19% revision rate with outcomes of other commonly used VPI procedures reported in the literature, we found revision percentages of 13% to 16% for sphincter pharyngoplasties with high inset of the flaps at the level of attempted velopharyngeal closure (Riski et al., 1992; Witt et al., 1998; Losken et al., 2003; Pryor et al., 2006) and of 12% to 20% for superiorly based pharyngeal flaps (Witt et al., 1998; Keunig et al., 2009). However, making a valid comparison is hampered by the retrospective nature of the studies, differences in length of follow-up, differences in speech methodologies (in particular the use of live clinical data versus blind independent listening), differences in study population (with or without exclusion of patients diagnosed with a syndrome), and differences in the indication setting for revision surgery. As a consequence of the surgical decision-making process for VPI in the NTCS, 60% of the patients that were selected for a buccinator flap procedure had already undergone a palatal re-repair to retroposition anteriorly placed levator muscles without the desired success. Moreover, 50% of patients were diagnosed with a syndrome. The study population may therefore represent a subgroup of complex VPI patients that is more difficult to treat than the average patient. An advantage of the buccinator flap procedure in comparison with most types of pharyngoplasties, is that the procedure is technically relatively easy to learn and perform and to teach to trainees. Also, the buccinator flap procedure allows for a straightforward simultaneous repair of palatal fistulas at the border of the hard and soft palate. No major surgical complications were reported in our series, such as flap loss or airway obstruction. Further research comparing the buccinator flap technique with other procedures in a randomized and prospective way is warranted to make a final judgment on relative outcomes and complication rates.
Several potential prognostic factors that may influence the need for revision surgery were tested (male, age > 7 years, previous VPI surgery, syndromic diagnosis, operation before 2006 or surgical learning curve, simultaneous levator retropositioning). None of them were able to predict poor outcome (need for revision) after the buccinator flap procedure. Since the sample size is small (only six patients in the revision group), further research is needed in larger patient groups.
Independent, blind speech analysis showed a significant decrease in hypernasality with a normal postoperative resonance in 21 of 26 patients (81%) and a significant decrease in passive cleft speech characteristics. The mean score for nasal airflow errors (audible nasal emissions and nasal turbulence) did not change significantly after the operation. Strikingly, in 7 of 26 patients (27%), nasal turbulence worsened after the procedure. This is probably associated with a small residual velopharyngeal defect, whereas nasal turbulence was less pronounced or absent preoperatively due to the large size of the velopharyngeal gap (Kummer et al., 1992).
This study has demonstrated that the operation increased the soft palate length on average by 7.5 mm and reduced the velopharyngeal defect on palate elevation. The width of the buccinator flaps at the time of surgery was about 1.5 to 2 cm. At the time of the postoperative investigations (on average 9 months after surgery, with a minimum postoperative interval of 6 months), we measured a mean lengthening of 7.5 mm, demonstrating the occurrence of flap contraction during healing. The annual growth of the palate in patients with a previously operated cleft is reported to be on the order of magnitude of 1 mm per year (Coccaro et al., 1962) and is probably less pronounced in the year after palatal surgery, so the degree of lengthening we measured is indeed mainly caused by the insertion of the buccinator flaps.
This study has its limitations. Audio-video recordings of sufficient quality were not available for all of our patients, and blind speech analysis and palate measurements were therefore only possible in a subset of the study group (speech: 26 of 32 [81%], videofluoroscopy: 30 of 32 [94%]). The study population comprised a significant number of very young patients (14 of 31 were under 5 years old) with severely impaired speech, complicating the speech assessment and resulting in a moderate interrater reliability for part of the speech parameters. Due to the retrospective nature of the study, we had to rely on case note data to assess the complication rate. Though no snoring or sleep apnea was reported in our series, a prospective study including pre- and postoperative sleep studies is warranted. The presence of a velopharyngeal gap was assessed on lateral videofluoroscopy images only. Therefore, in cases in which velopharyngeal closure was observed, an asymmetrical velopharyngeal gap could in theory not be excluded. Another point of critique could be the heterogeneity of our study group, with a representation of all cleft types and a high percentage of syndromic cases. However, this reflects the reality in a velopharyngeal investigations clinic in a regional cleft team, particularly in a tertiary pediatric setting.
Conclusion
The buccinator flap procedure is a relatively safe and easy procedure. It is an appropriate surgical option in patients in which short palate length is the primary factor in VPI.
Footnotes
Acknowledgments
The authors would like to thank Johnny Volcano (medical photographer), David Searl (database manager), and Guy Thorburn (consultant plastic surgeon) for their help in editing the speech audio-video recordings and videofluoroscopies.