
Abstract
This article describes a new method that enables vector control during alveolar distraction osteogenesis in the treatment of a cleft palate patient. The patient presented with unilateral complete cleft lip and palate, and the alveolar part of the defect was covered by a mobile buccal flap. The distraction was performed by sliding the surgically released tooth segment with the help of an intraoral distractor over 1.5-mm stainless steel archwires held by metal crowns. This vector-controlled method enabled new bone and attached gingiva formation in harmony with the proper alveolar shape.
Large alveolar defects are a major problem for orthodontists in the treatment of cleft palate. Buccal and tongue flaps were used to cover such defects for many years. However, the results have been far from satisfactory in terms of clinical expectations. Clinicians have focused on distraction osteogenesis to overcome this problem. There are many successful case presentations and publications on this subject (Liou et al., 2000; Dolanmaz et al., 2003; Mitsugi et al., 2005). In all of these reports, distraction was carried out in a straight line. We herein introduce a new method that enables vector control during alveolar distraction osteogenesis.
Method
The method described herein comprises archwise distraction (AWDA) of the greater segment in a unilateral cleft patient. First, the transport and the anchor segments were determined, and cobalt-chromium (Co-Cr) crowns were fabricated accordingly without tooth preparation. The cast crowns consisted of two units: the transport segment and the anchoring segment, connected by a transpalatal bar. These cast metal crowns were tried in before cementation. Precise adaptation was required to ensure sufficient mechanical stability to withstand the forces resulting from the distraction process. The crowns were cemented with glass ionomer cement and the excess was removed. The metal crowns had double tubes on the molars and semicircular tubes on the other teeth to allow the surgeon to place the two 1.5-mm stainless steel archwires during the osteotomy. All the tubes were placed at the same horizontal level, enabling the segments to slide onto the archwires.
A custom-fabricated tooth-borne distractor is placed during surgery on either the gingival or the occlusal archwire, depending on the vestibular sulcus depth of the patient (Fig. 1). It is preferable to place the distractor on the gingival archwire to carry the point of force application close to the center of rotation of the transport segment to avoid an undesirable tipping effect. In the case described below, the distractor was placed on the occlusal archwire for patient comfort and ease of activation.
Stainless steel archwires (1.5 mm) and the intraoral distractor.
After the latency period (5 days), the distractor was activated one half-turn (0.5 mm) twice per day, and the device exerted a pushing force on the surgically released segment.
A significant advantage of this method is the infinite activation. The maximum opening capacity of the distractor itself is only 8 mm. After this is reached, the screw is completely closed. Semicircular activation tubes of variable width (C-rings) instead of one single straight C-ring are crimped onto the archwire and follow its curvilinear shape. This method allows infinite and vector-controlled activation of the distractor.
Case Report
A 16-year-old male patient presented with unilateral complete cleft lip and palate. The patient had already undergone an unsuccessful bone-grafting surgery, and only a thin bone bridge remained between the two segments facing the cleft space. The defect area was covered by mobile buccal flap that was not able to withstand normal oral functions (Fig. 2a). The treatment plan involved closure of the cleft gap using distraction osteogenesis. Treatment started with leveling and alignment of the dental arches by conventional orthodontics (Fig. 2b and 2c).
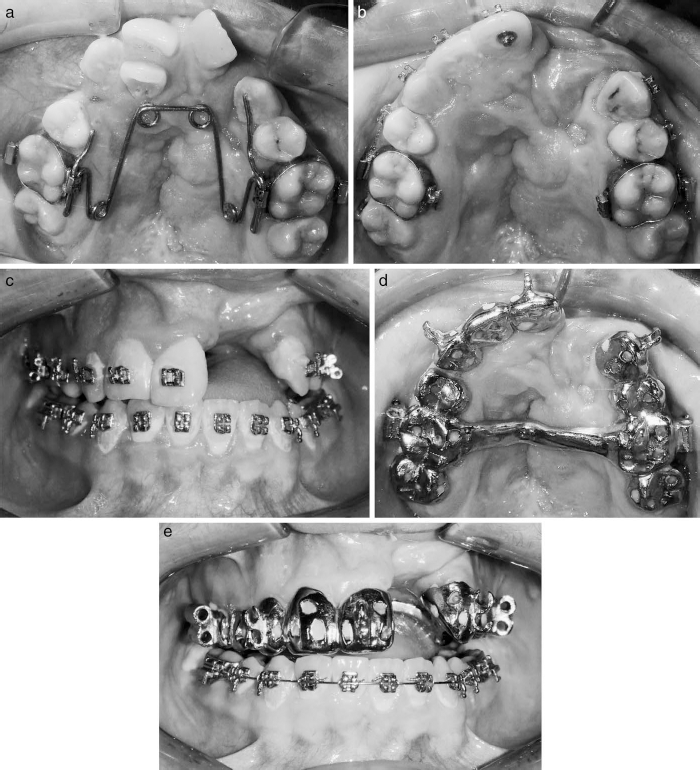
a: Pretreatment upper occlusal view, b, c: Intraoral pictures after leveling and alignment, d, e: Intraoral pictures with bonded cast metal crowns.
A precise two-phase silicone impression was taken after debonding braces. The Co-Cr metallic crowns were fabricated with no prior tooth preparation. Two stainless steel archwires (1.5-mm thickness) were bent according to the shape of the dental arch (Fig. 2d and 2e).
The cast metal appliance was cemented with hybrid glass ionomer cement before the surgery. The operation was performed under general anesthesia. The segment containing the upper right canine and central and upper left central teeth was mobilized by an osteotomy line passing under the anterior nasal spine and above the root apices. This approach maintained the nasal floor, and the distraction disc was able to pass through the midline. During this process, the palatal mucosa was left intact. The bone bridge remaining from the former unsuccessful bone grafting surgery was accessed by tunnel elevation and completely removed so that it would not hinder the distraction process. This area was dissected using the elasticity of the mobile mucosa graft. The arches and the distractor were inserted into the tubes and semitubes during surgery, and the archwires were cinched back. The distractor was activated with five full 5-mm turns to ensure that the segment was indeed liberated. The distractor was then closed, and the flaps were sutured.
After a 5-day latency period, activation was started at a rate of one half-turn (0.5 mm) twice per day (Fig. 3a and 3b). The patient was recalled weekly until the distraction segment contacted the left upper canine crown. The adjacent metal crown surfaces were completely ground to obtain closer bone contact (Fig. 3c through 3e).
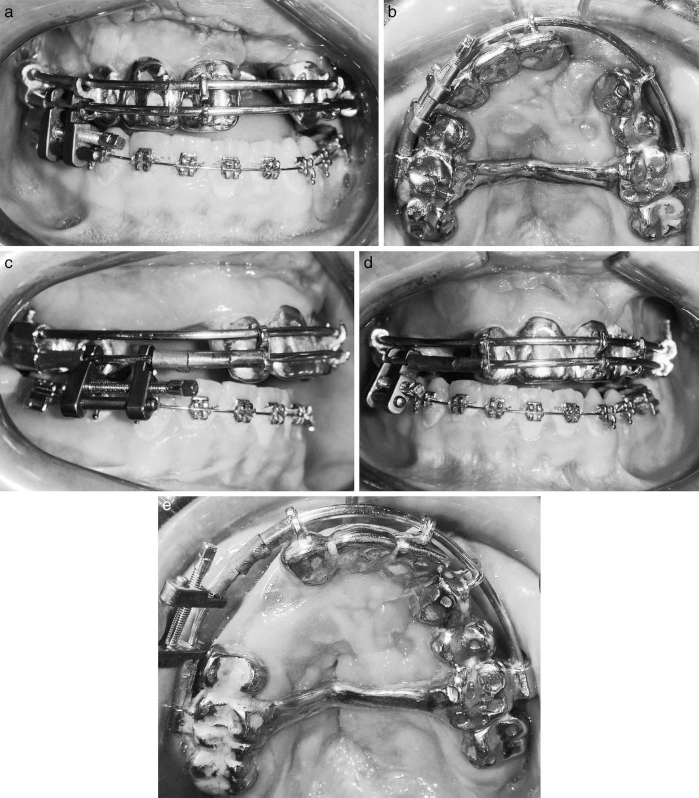
a, b: Intraoral pictures just after the surgery, c through e: Intraoral pictures after the completion of distraction.
After 2 months, the metal crowns were removed. The teeth were prepared. The maxillary right central incisor was converted into a lateral incisor, and the left central incisor substituted the right central incisor. The left upper canine was converted to the left central incisor, and a fixed prosthesis was cemented to maintain the treatment results and improve aesthetics (Fig. 4a through 4d; Fig. 5a through 5d).
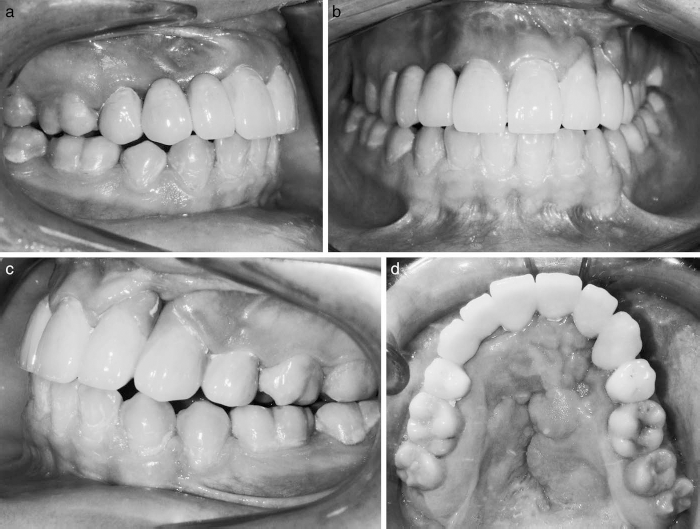
a through d: Posttreatment intraoral pictures.
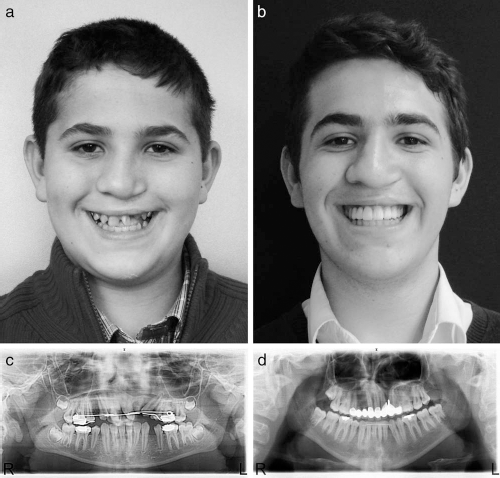
a: Pretreatment smiling picture, b: Posttreatment smiling picture, c: Pretreatment panoramic radiograph, d: Posttreatment panoramic radiograph.
Discussion
In the case presented herein, orthodontic treatment alone would not meet the patient's requirements. Out of many available treatment methods, we chose distraction osteogenesis.
The results of this case report are comparable with those of investigations focused mainly on maxillary segmental distraction (Liou et al., 2000; Guerrero, 2002; Erverdi et al., 2012a; Erverdi et al., 2012b). The method used a tooth-borne distractor and required an osteotomy surgery only, which is an advantage compared with distractions made with the Liou distractor. The Liou distractor is a bone-borne distractor that requires two surgeries: one for placement and a second for removal. On the other hand, this distractor orients the generated bone in a straight line, while the curvilinear distraction enables successful reconstruction of the alveolar ridge with its proper oval shape. Another advantage of our method is that the arch-shaped bone and attached gingiva closely resemble normal morphology. Additionally, the attached gingiva and the newly formed bone can withstand oral functions to a greater extent than can tongue or cheek flaps, which are prone to irritation. Finally, the amount of activation possible with the Liou distractor is limited; whereas, our distractor has infinite activation potential.
Two rigid, thick archwires were used to increase rigidity and were found to adequately prevent undesired tipping of the distraction segment. The outcome of this treatment method fully satisfied the patient's and our expectations because it resulted in successful alveolar ridge construction.
The new bone formed during distraction was more than sufficient for the successful placement of dental implants, however implants were not used in this patient for several reasons. First, the maxillary arch was expanded at the beginning of the treatment. Due to the lack of bone on the hard palate and the scar tissue remaining from the former surgeries on the palatal mucosa, the arch was prone to collapse and required maintenance during and after the treatment. Therefore, complete bridgework was preferred. The patient's smile was significantly improved and the fixed prosthesis completely satisfied his expectations.
When the patient applied for treatment, his first bicuspids were extracted and extraction of the upper right lateral incisor was discussed. Due to the lack of space, it was not possible to fit the lateral incisor into the arch. The root of the upper left central incisor was inclined mesially. Moreover, we were unable to push the tooth into the cleft area because there was insufficient bone distal to it. Leveling of the lateral tooth in the bone generated after distraction was also considered, but the osteotomy line planned by the plastic surgeon was supposed to pass through this area, which would have risked the blood supply of the transport segment. For that reason, the tooth was extracted at the beginning of the treatment.
After the distraction, we could eventually distract back to the midline and regraft the patient, but that would require an extra surgery and time. Furthermore, the results of an extra grafting surgery cannot be predicted. In this case, the midline shifting of the transport segment was uneventful.
The only disadvantage of this technique was the appearance of the appliance; the metal casts could be regarded as unaesthetic, although they are in place for no longer than 3 months. Suzuki et al. (2006) used a tooth-borne distraction device combined with an external distractor and concluded that additional surgeries may be avoided by the simultaneous closure of a wide cleft/fistula and advancement of a hypoplastic maxilla. In contrast, Wang et al. (2009) commented that the use of an external distractor can negatively affect the patient's social life because she or he must wear a bulky cranial frame. The intraoral method used in the present case is thought to be acceptable from a social point of view. However, a new appliance with aesthetic crowns can be fabricated instead of full metal crowns.