
Abstract
Objective
Patients with cleft lip and palate (CLP) and maxillary retrognathia are usually treated with maxillary advancement (Le Fort I osteotomy). The aim of this study was to investigate the impact of maxillary advancement on the velopharyngeal function (VPF) and symptoms of velopharyngeal incompetence in patients with CLP.
Design
Retrospective group study before and after treatment.
Participants
All patients who had undergone Le Fort I osteotomy due to maxillary retrognathia from 2007 to 2010 at Karolinska University Hospital, Sweden (n = 13). Pre- and postoperatively standardized examinations were used. Blinded audio recordings were independently assessed by three experienced speech pathologists. Acoustical data (nasometry) and information on VPF (videoradiography and nasoendoscopy) were collected from the medical records. Two patients with additional malformations were considered outliers, and group data were based on a sample size of n = 11.
Main Outcome Measures
Perceptual and acoustic symptoms of velopharyngeal incompetence and overall assessment of VPF.
Results
No assessment method showed a significant deterioration of the VPF postoperatively. Individual data revealed that 6 of the 13 patients had no or only one symptom pre- and/or postoperatively. The two patients with additional malformations had most symptoms pre- and postoperatively and did not change. Three patients had an increased number of symptoms postoperatively by at least two symptoms. No associations between the outcome and possible prognostic factors were found.
Conclusions
Maxillary advancement did not have a significant impact on the VPF at the group level, but three individuals had a somewhat deteriorated VPF postoperatively.
Cleft lip and palate (CLP) is a common congenital anomaly, with a prevalence of 1 to 2:1000 (Hagberg et al., 1997). Primary palatal repair can be performed in different stages: in one stage, usually between 6 and 18 months of age; in two stages, with either early soft palate closure at around 6 months of age and hard palate repair later on, or with closure of the hard palate first and of the soft palate later (Peterson-Falzone et al., 2010). The anomaly of the palate combined with scarring after surgical procedures are probably the main causes for velopharyngeal incompetence (VPI) in CLP (Collins et al., 2012).
Velopharyngeal incompetence is defined as a dysfunction of the velum and/or the pharyngeal wall at the level of the nasopharynx resulting in inadequate velopharyngeal closure and hypernasality (Peterson-Falzone et al., 2010). An underdeveloped maxilla or fistula or discontinuity in the alveolar ridge will also contribute to impairment in speech production and articulation deviances (Schendel et al., 1979; Lewin et al., 1980). Also, the deterioration of velopharyngeal function (VPF) may lead to audible nasal air leakage and weakness on pressure consonants (Haapanen et al., 1997; Trindade et al., 2003). As a result, the speech intelligibility may be reduced. The most frequently used procedure for correction of VPI is a pharyngoplasty, (e.g., Cable et al., 2004; Yamashita et al., 2008).
Primary palate repair increases the risk of maxillary growth disturbance. The cause of maxillary retrognathia is debated, although a plausible theory is that primary palatal repair accentuates an intrinsic deficiency in midfacial skeletal growth (Ross, 1987; Good et al., 2007; Chua et al., 2010). Not only the chosen surgical method to repair the palate but also the experience of the surgeon is suggested to influence maxillary growth (Shaw et al., 1992; DeLuke et al., 1997).
Maxillary retrognathia affects both aesthetics and function (Chanchareonsook et al., 2006). The incidence of orthognatic surgery in CLP patients varies between 10% (Lilja et al., 2006), 27% (Ross, 1987), and 47% (Good et al., 2007). The standard procedure has been maxillary advancement with Le Fort I osteotomy for the past 60 years (Saltaji et al., 2012), but distraction osteogenesis is an alternative in severe maxillary retrognathia (Cohen, 1999; Figueroa and Polley, 2007).
When the maxilla is advanced surgically, the soft palate is also advanced to some extent, which leads to an increased space between the soft palate and the posterior pharyngeal wall. This would normally be compensated by the lateral pharyngeal and palatal musculature. However, some patients with CLP do not have the ability to compensate for this anatomical change, which may result in VPI (i.e., hypernasality, nasal air leakage, and weak pressure consonants; McComb et al., 2011).
As reported in Witzel and Munro (1977), several studies of the correlation between maxillary advancement and VPI, particularly in those with borderline function preoperatively, have been performed. Surprisingly, improved VPF was seen in 21% of the patients in one study, all with a pharyngeal flap in place at surgery (Watzke et al., 1990). No correlation between maxillary advancement and changes in VPI has been reported (Kummer et al., 1989).
Although there might be a risk for developing VPI after maxillary advancement, the surgery also has a potentially beneficial impact on articulation, since the reestablishment of a normal bite facilitates the positioning of the lips, tongue, and jaw (e.g., Chanchareonsook et al., 2006; Pereira et al., 2013).
Since it is of importance to detect patients with a risk of developing VPI after maxillary advancement, all patients are examined preoperatively. It is also important to assess speech and VPF after the operation to detect deterioration in speech and find a suitable treatment for side effects (Trindade et al., 2003; Janulewicz et al., 2004; Chanchareonsook et al., 2006). The velopharyngeal sphincter is a highly complicated mechanism, and it may sometimes be necessary to use different imaging modalities to obtain an adequate evaluation of the velopharynx (Skolnick et al., 1973).
Minimal standards have been proposed for reporting the results of surgery in patients with CLP with at least one instrumental assessment method in addition to perceptual evaluation of speech, to obtain an adequate assessment of speech (Dalston et al., 1988). For evaluation of VPF, videofluoroscopy (VF) and videonasoendoscopy (VNE) should be included (Golding-Kushner et al., 1990). Nevertheless, one review showed that 74% of the studies on maxillary advancement had applied perceptual speech assessment methods alone (Chanchareonsook et al., 2006). The relative value of an extensive examination has not been evaluated except in one study, which showed that 68% of the patients were recommended the same treatment regardless of the amount of examinations (Havstam et al., 2005). A recent critical review not only pointed out inconsistencies in the assessment methods but also concluded that the sample sizes often were insufficient (Pereira et al., 2013). The same conclusion could be drawn from another review, in which only 4 of 39 studies involved 40 to 60 patients, and the most common sample size was 2 to 10 patients (Chanchareonsook et al., 2006).
Thus, the knowledge base regarding the impact of surgical maxillary advancement on speech and VPF in individuals born with cleft palate is small with somewhat diverse findings. Our clinical experience does not consistently reflect the diversity. The primary aim of this project was therefore to add to the knowledge by investigating the impact of maxillary advancement, with Le Fort I osteotomy, on VPF and speech symptoms of VPI in patients born with CLP. A second aim was to investigate whether or not preoperative assessments of VPF, a pharyngeal flap, and the length of the advancement could be possible prognostic factors. In addition, we wanted to study the agreement between the auditory, acoustic, and visual assessments.
Methods
This retrospective comparative study was approved by the local ethical committee in Stockholm, Sweden (Dnr 2011/1278-31/1).
Subjects
The study was based on material from pre- and postoperative examinations on 13 consecutive young adults, eight males and five females, who were born with cleft lip and palate and had undergone maxillary advancement during 2007 to 2010 at Karolinska University Hospital, Stockholm, Sweden (Table 1). Eight patients had bilateral cleft lip and palate (BCLP), and five had unilateral cleft lip and palate (UCLP). One patient had the cleft palate as a part of a rare syndrome, and one had a dysmorphological configuration of the face and other additional symptoms but no syndrome diagnosis. All patients had undergone primary lip repair at the age of 5 to 7 months and primary palate repair at the age of 10 to 15 months, except for one patient who had primary palate repair at 7 months. The age of the patients at orthognatic surgery varied between 17 and 23 years (mean, 19.5 years). All patients were operated with conventional Le Fort I osteotomy by two experienced plastic and maxillofacial surgeons. The length of advancements ranged between 2 and 9 mm (mean, 6.2 mm). In two cases, there was also a minor rotation (1 to 2 mm), and in five cases, there was a vertical movement of 1 to 4 mm of the maxilla. Twelve patients did not have any relapse 1 year postoperatively, while one patient (No. 1) had a relapse of 1 to 2 mm, leading to an edge-to-edge occlusion. Four patients had a pharyngeal flap, and two of them had their flaps corrected. Eight patients had additional surgery, such as set back of the mandible. Four patients had palatal fistulas, pre- and/or postoperatively.
Demographics of the Included Patients *
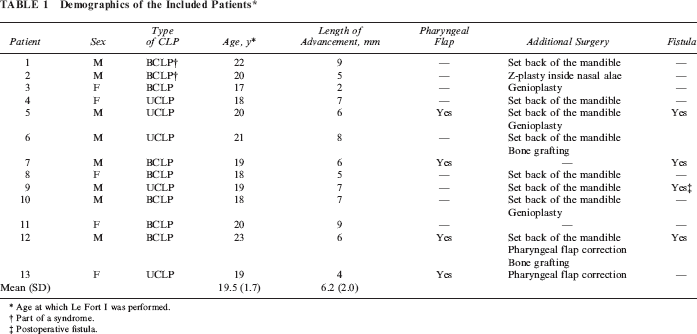
Age at which Le Fort I was performed.
Part of a syndrome.
Postoperative fistula.
The material was obtained as a part of the clinical routine, which had been standardized for this purpose. It contained audio recordings, acoustic measurements with the Nasometer, videonasoendoscopic and videofluoroscopic examinations, and the medical records. The examinations were performed 1 to 28 months preoperatively (mean, 11 months) and 8 to 22 months postoperatively (mean, 13 months). All postoperative examinations were performed at least 12 months after the operation, except one Nasometer examination 8 months postoperatively. Only one examination was performed after 16 months.
Audio Recordings
All speech examinations were performed using the speech material from the Swedish articulation and nasality test (Lohmander et al., 2005). The audio recordings were performed in a standardized manner with digital technique in a sound-treated room. Seventeen of the examinations were recorded on a digital audio tape recorder (Sony Walkman TCD-D8), and 19 examinations were recorded in Soundswell signal workstation (Ternström, 2000), with a microphone (AKG D190E). The recordings were edited in the computerized program Soundswell (sound file editor in Microsoft Windows System, version 4.; (Ternström, 2000) to create speech samples that were as homogenous as possible. Three representative speech samples were collected from every recorded examination: repetition of sentences, reading, and retelling of a standard text. The sentences consisted of 10 sentences with only oral consonants, one with only nasal consonants, and three sentences with mixed oral and nasal consonants. The latter included consonants varying in place of articulation, with emphasis on different plosives in combination with high and low vowels, whereas the oral sentences included either high- or low-pressure consonants (Lohmander et al., 2005). The text (Pojken och bonden, eng. “The boy and the farmer”) is routinely used for documentation of connected speech at our center. It contains 89 words and takes about 30 to 40 seconds to read. Each speech sample was approximately 20 to 60 seconds, and all samples (n = 144) were saved as separate .wav files.
Perceptual Speech Assessments
The edited speech samples were presented in random order for blinded perceptual analysis of speech and VPF. The variables and rating scales used are presented in Table 2. One third of the speech samples were randomly selected for repeated evaluation. Three qualified speech pathologists, who had not been involved in the patient care, made the analysis using ordinal rating scales. The assessments were performed individually with the use of headphones, and the listeners could relisten as many times as desired. The variables hyper- and hyponasality were used for evaluation of resonance and weak pressure consonants and audible nasal air leakage (which included nasal air emission and nasal turbulence) for evaluating other symptoms of VPI. An overall evaluation of general impression of speech and VPF was also performed. A nationally agreed five-point rating scale (from 0 to 4) was used for evaluation of hypernasality, hyponasality, weak pressure consonants, nasal air leakage, and overall impression of speech, and the VPF was assessed perceptually to be either competent, borderline, or incompetent (Lohmander et al., 2005). The median value of the ratings from the three observers was used as the result, and a scale value ≥2 and/or borderline VPF/incompetent VPF was considered as a symptom of VPI.
Variables and Rating Scales for the Perceptual Analysis of VPF and Other Symptoms of VPI

Nasometry
The Nasometer provides an indirect, quantitative measure of the VPF (Dalston et al., 1991). The measurements with the Nasometer (Kay Pentax Nasometer II, model 6400, Kay Elemetrics, 2001) had been performed on the same occasion as the audio recordings. The speech material contained the same oral sentences as those used in the perceptual analysis. The set of sentences was repeated twice in a sequence and then measured. Mean values and range for the stimuli were registered for each patient. The mean values were compared with normative nasalance values for adults, 17% (SD, 7) for oral sentences (Annelin et al., 2006). Values higher than the normative nasalance values (i.e., +2SD = 31%) were considered as a symptom of VPI. Changes in the nasalance scores between the pre- and postoperative examinations were calculated as percentages, and a change of more than five units was considered significant (Brunnegård and van Doom, 2009).
Videofluoroscopy and Videonasoendoscopy
The VF examinations had been recorded in frontal and lateral projections of velopharyngeal movements during connected speech. The speech material contained the same oral sentences, including high-pressure consonants, as those used in the perceptual analysis. In addition, syllable repetition was included containing bilabial, dental, and velar place of articulation for plosives and /s/ in combination with a high and a low vowel. The radiographic equipment that had been used at all examinations consisted of an x-ray tube (Bi 150/30/50/R), image intensifier (Siemens Sirecon II), Vidicon camera, Arriflex cine-camera running 35-mm film, and a TV monitor. A cephalostat was used for immobilization of the patient's head, and a microphone (Sony ECM-50PS electrets condenser) was attached at chest level for speech recording. A video camera simultaneously recorded facial movements. The synchronized recordings from the Vidicon camera, the TV camera, and the microphone were transferred to a mixing board and registered on a digital videotape. A barium sulphate contrast medium (EZ HD, E-Z-EM Company, Westbury, NY) was applied via the nasal cavity to improve the visualization of the soft tissues of the velum and nasopharynx (Henningsson and Isberg, 1986, 1991). The images were screened at the same magnification for each patient and each time point. The estimated total length of the radiation exposure including positioning and both projections was 1.5 minutes.
Videonasoendoscopy had been performed during the same examination as the VF. A flexible, fiber-optic, end-viewing nasopharyngoscope (Olympus ENF type P), with a diameter of 3.7 mm at the distal end, was inserted into the most patent nostril. The use of a high-intensity xenon cold light supply with automatic exposure (Olympus CLV) allowed video recording of the velopharyngeal movements during speech with simultaneous sound. The same speech material that was used during VF was used during VNE.
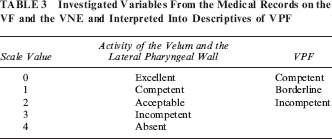
The activity in the pharyngeal walls and velum and the VPF had been assessed according to a standardized clinical routine with consensus by two examiners and documented in the medical records. The assessments were compiled from the VF and the VNE and were interpreted by the first author, who had not been involved in the examinations or original assessments into descriptive scale values of three variables (Table 3). The descriptions of the activity of the velum and the lateral pharyngeal walls were collected from the VF and the VPF from the VNE. A scale value ≥2 and/or borderline/incompetent VPF was considered as a symptom of VPI.
Investigated Variables From the Medical Records on the VF and the VNE and Interpreted Into Descriptives of VPF
Statistical Analyses
Collected data were processed with SPSS (Statistical Package for Social Sciences), version 20. Mean, standard deviation (SD), median, range scores, skewness, and kurtosis were investigated. The distribution of discrete data (nasalance scores) was tested with the Kolmogorov-Smirnov test and was not significant (i.e. the data were considered normally distributed). Two outliers were identified by quartile range analysis (patients 1 and 2) with values greater than the third quartile for nasalance and VPF and were not included in the statistical analyses. Differences pre- and postoperatively were tested with paired-sample t test or Wilcoxon signed ranks test. The correlations between assessments and between outcome results and possible prognostic factors were tested with the Spearman rank correlation test if ordinal data were included or with Kendal's tau_b for nominal data. Inter- and intrarater reliability were calculated by means of agreement point by point. P values less than .01 were considered to be statistically significant after Bonferroni correction.
Reliability
Reliability was measured as percentage agreement, point by point for the variables in the perceptual analysis. The intrarater agreement based on reassessment of 33% of the samples was 81%, 84%, and 76%, respectively, for the three listeners. If a difference of one scale value was accepted as agreement, the intrarater agreement was 100% for all three. The exact interrater agreement was poor between each pair of listeners (76%, 38%, 52%) but improved if a difference of one scale value was accepted as agreement for each pair of listeners to 94%, 85%, and 75%. Median values are presented as results in order to use the values from raters with the closest ratings (i.e., with the highest agreement).
The interpretations of the VF and nasoendoscopy examinations into the scale values of the four variables were discussed and verified by the experienced speech pathologist who originally performed all the examinations. No other control for reliability was performed.
Results
The results of the examinations for all 13 patients are summarized in Table 4. The table presents the number of symptoms of VPI from the auditory perceptual assessment, Nasometry, and visual perceptual assessment using VF and VNE. All results from statistical analyses are based on data from 11 patients (i.e., without the two outliers; Table 5). In summary, no assessment method showed a statistically significant deterioration of VPF postoperatively in the group.
Patients With Preoperative and Postoperative Symptoms of VPI *
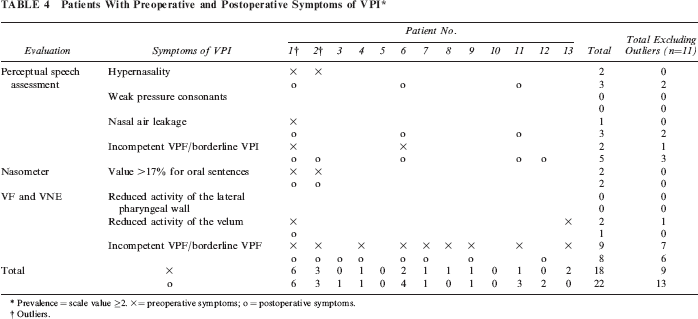
Prevalence = scale value ≥2. X = preoperative symptoms; o = postoperative symptoms.
Outliers.
Median Values, Ranges, Changes, and Significance for Perceptual Speech Assessments Preoperatively (Preop) and Postoperatively (Postop) of the Six Variables (n = 11) *
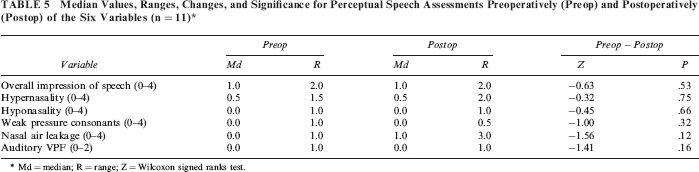
Md = median; R = range; Z = Wilcoxon signed ranks test.
Perceptual Speech Assessments
One of the 11 patients had preoperative perceptual symptoms of VPI, and three patients had symptoms postoperatively (Table 4). No patient had hyponasal speech or weak pressure consonants, neither pre- nor postoperatively, and no patient had severe hypernasality, constant occurrence of nasal air leakage, or severely reduced general impression of speech. One patient preoperatively and two patients postoperatively had a moderately reduced overall impression of speech. There were no statistically significant changes (Wilcoxon signed ranks test) from the preoperative to the postoperative assessment (Table 5).
Nasometer
The 11 patients had scores below the normative nasalance values both pre- and postoperatively, even though four of these patients had significantly increased scores postoperatively compared with preoperatively. No patient had decreased scores postoperatively. The Nasometer measurement showed significant changes (paired-sample t test) at a group level for oral sentences postoperatively (P < .01; Table 6).
Means, Standard Deviations, Median, Ranges, Changes, and Significance of the Results of the Examinations With the Nasometer Preoperatively (Preop) and Postoperatively (Postop) for Oral Sentences *

Bold figure shows statistically significance, n = 11. M = mean; SD = standard deviation; Md = median; R = range; t = paired-sample t test.
Videofluoroscopy and Videonasoendoscopy
All patients had excellent activity of the lateral pharyngeal walls, both pre- and postoperatively according to the clinical assessment. The VPF was, however, judged as borderline incompetent in seven patients preoperatively. Three of these had improved to competent VPF, and one had deteriorated to incompetent VPF postoperatively. Also, two patients with competent VPF preoperatively had borderline VPI postoperatively (Table 4). No changes were statistically significant (Wilcoxon signed ranks test: Z = 0.00, P = 1.00; Z = −0.71, P = .48).
Summary of Results
The assessments with the different methods showed that of the 11 patients, seven had one or more symptoms of VPI preoperatively. Two of these patients had more symptoms, three the same symptoms of VPI, and two fewer symptoms postoperatively. However, only one patient preoperatively and two patients postoperatively had symptoms of VPI at both the perceptual speech assessment and at the VF and VNE. Two patients with cleft palate as part of a syndrome/additional malformation had the highest number of VPI symptoms both pre-and postoperatively. Both were deemed to be outliers and not included in the statistical analyses.
Possible Prognostic Factors
The preoperative status of the VPF, the presence of a pharyngeal flap, a fistula, the length of advancement, and time after operation for postoperative assessment were compared with the postoperative result for each variable from the perceptual speech assessments, the measurements with the Nasometer, and the VF/VNE examinations. There were no significant associations (Kendall's tau_b) between any of the factors and the outcome. Three of the four patients with a pharyngeal flap had also a fistula preoperatively, and one of these was assessed to have a somewhat deteriorated VPF postoperatively. Another patient had a fistula postoperatively but no change of speech or VPI symptoms. The other patients with fistulas were not among those with assessed deviances in speech or VPF.
Correlations Between Methods for assessment
There were significant positive moderate correlations between the auditory perceptual ratings and the acoustic Nasometer measurements for the postoperative assessments of the 11 patients (rho = .75, P < .01; rho = .59, P < .01; Table 7). The determination coefficient (r2) revealed an explained variance of 56% and 35%, respectively.
Correlations Between the Auditory, Acoustic, and Visual Assessments (n = 11) *
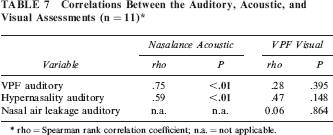
rho = Spearman rank correlation coefficient; n.a. = not applicable.
Discussion
No assessment method showed significant deterioration of VPF or aggravated symptoms of VPI at the group level around 12 months postoperatively after maxillary advancement with Le Fort I, even though four patients had a deterioration regarding one or two symptoms of VPI postoperatively. Two of these had a change from the auditory perceptual assessment, but no change was to a severe degree. The Nasometer showed a significant increase in nasalance values at the postoperative examination, but the values were still within the normative nasalance range (Annelin et al., 2006). There were no significant changes at the examinations with VF and VNE or in the compiled VPF score from the medical records. Hence, in the present study, there were no significant relationships between the postoperative changes in VPF and symptoms of VPI after Le Fort I osteotomy, and this finding is in agreement with previous observations (Kummer et al., 1989). Others have concluded that maxillary advancement can trigger or worsen VPI. Trindade et al. (2003) observed a significant increase in mean nasalance score, Janulewicz et al. (2004) observed significant deterioration in VPF and symptoms of VPI with perceptual speech assessments, and Watzke et al. (1990) found impaired VPF with aerodynamic assessment. In these reports, the study groups were larger than in the present study, which can be the reason for these differences. However, only one assessment method was used in these studies, and in one of them (Janulewicz et al., 2004), only clinical data were reported with no reliability, which weakens the implications of the results. Haapanen et al. (1997) reported a significant deterioration of VPF based on perceptual speech assessment in 27% of the 15 investigated patients but found no change in postoperative aerodynamic data or results from nasometry. Further, since the latter were interpreted in relation only to the preoperative scores and not to normative nasalance values, it is not clear whether these were deviant at the preoperative measurement. Reliability of the perceptual assessment was not reported, which potentially invalidates the perceptual speech findings.
Epker and Wolford (1976), Witzel and Munro (1977), Haapanen et al. (1997), and Trindade et al. (2003) all concluded that patients with borderline VPF preoperatively are more likely to get deteriorated VPF after maxillary advancement. No such association could be seen in the present study, in which only one patient had a symptom of VPI preoperatively. A higher number of subjects might have shown a different picture. Pereira (2012) included 20 patients with CLP in her study of the impact of maxillary advancement on speech and VPF. Several measures were used, and a multiple regression analysis revealed that the rating of hypernasality and nasal turbulence and measures from lateral VF, such as closure ratio, were predictive for the postoperative outcome. However, due to only moderately good agreement of the perceptual assessments, the results need to be interpreted with caution according to the author.
In the present study, there was no significant correlation between the length of advancement and the postoperative changes in hypernasality, which is in accordance with the findings by Watzke et al. (1990). In contrast, intelligibility was related to the length of maxillary advancement in the study by Maegawa et al. (1998) in patients with a maxillary advancement of more than 10 mm. However, large advancements such as in the latter study are most often not recommended, because the risk of speech deterioration is too large and the procedure is also technically very demanding (LaRossa, 2000). The results so far seem contradictory, which could be due both to methodological differences for outcome analysis and to differences in the variety of length of advancement in the studies.
Recent findings suggest that postoperative results are stable already after 3 months and that 3 months should be sufficient for a postoperative review (Pereira, 2012). This would mean that if pharyngeal flap surgery is needed, it could be performed within 6 months postoperatively and thereby reduce possible problems with speech. However, the possibility of relapse should also be taken into account (Cheung and Chua, 2006). Due to healing, adaption to the anatomical change, and surgical relapse, the postoperative result may not be stable until 12 months after the operation (Janulewicz et al., 2004; Cheung and Chua, 2006). Thus, the results might be dependent on the time of the follow-up assessment, which is therefore important to specify. Pereira et al. (2013) reported that only nine studies (22%) used a minimum of 12 months after surgery before follow-up. In the present study, only one of the postoperative examinations (with the Nasometer) was performed within a shorter time than 12 months postoperatively. All other examinations were performed between 12 and 22 months after surgery. Only one patient (patient 1) had a relapse in the present study and was already omitted from the statistical analysis because the patient had a syndrome.
Two patients in the present study displayed a higher number of symptoms both pre- and postoperatively than did the others. For these two patients, the cleft was a part of a more complex syndrome, presumably with a combined and negative effect on the speech function already preoperatively, and no change in number of symptoms of VPI postoperatively was seen.
Methodology
This study was small, with restricted possibilities to generalize, and the risk of drawing incorrect conclusions due to random variation is high. Heterogeneity was another problem since almost all patients had additional surgery: mandibular set back, pharyngeal flap correction, bone grafting, and genioplasty. Logically, the additional surgery should not have an impact on the outcome since it does not affect the VPF except for the pharyngeal flap correction, but statistical analyses on these variations cannot be performed in these small groups.
Few studies used concurrent different assessment methods, and the knowledge is poor about which examination enables an appropriate assessment of VPF and speech. The gold standard for evaluation of VPF includes auditory perceptual speech analyses, acoustic measurements with the Nasometer, and visual perceptual assessments with VF and VNE (Pereira et al., 2013). However, the compliance with these guidelines is questionable, given that Chanchareonsook et al. (2006) reported that 74% of studies in the maxillary advancement literature had applied perceptual speech assessment methods alone. In the present study, all patients were evaluated auditorily, acoustically, and visually, and the results could thus provide a multifaceted picture of the VPF with possibilities for conclusions. On the other hand, the agreement of the assessments was not excellent, which reduces the reliability of the results.
As important as reliable examinations for evaluation of VPF is the use of blinded and independent speech analyses by specialized speech pathologists. Such analyses require that the data have been recorded and archived and that the examinations were standardized. Pereira et al. (2013) found that only five studies (12.5%) explicitly commented on whether or not their analyses were blinded. The undertaking and reporting of inter- and intrarater reliability tests is also essential (Lohmander and Olsson, 2004; Sell, 2005). However, such tests had been implemented in only 13 studies (36%) in the review by Pereira et al. (2013). In the present study, two raters were consistent and had good inter- and intrarater reliability. That is, the two raters presented >80% exact agreement within each of them and >90% accepting one scale value difference between them (Zarcone et al., 1991; Lim et al., 2012). The values for the third rater were slightly lower. However, since the results were calculated on the median of the three assessments, differences for one rater's evaluation should not affect the results.
The efficiency of a comprehensive evaluation procedure using different visualization techniques of VPI was investigated experimentally by Havstam et al. (2005). The authors reported that 68% of the patients were recommended the same treatment regardless of the amount of examinations, including combinations of VNE and VF in the lateral and frontal view. Nevertheless, one third of the patients in that study were not recommended the same action, which might lead to incorrect recommendations for those patients. In the present study, no patient except for the two with syndrome/additional malformations were assessed with symptoms of VPI at the measurements with the Nasometer, while only one patient had one symptom of VPI at the perceptual speech assessment and seven patients with the VF or VNE. The latter might be due to the invalidity of the data captured from medical records. If this is the case, the results of the clinical examinations might point in the wrong direction and lead to poorly based decisions. A blinded assessment of the VF and VNE registrations might have strengthened the validity of the data. However, performing such assessments reliably has been proven to be difficult (Pereira, 2012), which questions the benefit of the procedure. Further, the VF and VNE assessments were not significantly related to the auditory or acoustical measurements. In contrast, there were significant correlations between the measurements with the Nasometer and the perceptual assessment of hypernasality and VPF for the postoperative assessments. However, when including the two patients with syndromes/additional malformation in the comparison, the visual assessments were also related to the other assessments. Pereira (2012) suggested a selected and combined evaluation approach in patients treated for maxillary retrognatia, including clinical perceptual analysis and the calculated closure ratio from videofluoroscopic pictures in the lateral view. A similar selected approach for evaluation of VPF in patients with VPI has been suggested previously (Havstam et al., 2005).
Conclusions
The results of this study suggest that maxillary advancement did not have a significant impact on the VPF around 12 months postoperatively at the group level, even though deteriorated VPF was found for a few individuals. Because of the small and heterogeneous sample, the results need to be interpreted with caution. Further studies with larger sample sizes are required for the understanding of the impact of maxillary advancement on VPF and speech in patients born with CLP. Also, a selected combined approach could be suggested, including a visualization technique for examination of the VPF in patients with syndromes/additional malformations, whereas perceptual speech assessment from standardized audio recordings and Nasometry might be sufficient for examination of the typical patient.
Footnotes
Acknowledgments
The authors thank speech pathologists Liisi Raud-Westberg and Maria Lundberg for their speech analysis, Jill Nyberg for performing data collection, and Gunilla Henningsson for sharing her knowledge and experience on videofluoroscopic and videonasoendoscopic examinations.