
Abstract
Objective
To establish for the first time the prevalence of fistula symptoms and the effectiveness of secondary alveolar bone grafting to treat these symptoms in a single surgeon cohort in Bristol, United Kingdom.
Design
Direct questioning of 233 consecutive patients with cleft before and after secondary alveolar bone grafting as to the presence of fistula symptoms.
Setting
Southwest and South Wales Cleft Centre, Frenchay Hospital, Bristol, United Kingdom.
Participants
Consecutive patients with cleft who were being treated for secondary alveolar bone grafting.
Outcome Measure
Patients reporting presence of fistula symptoms. Data collection on cleft type (unilateral, bilateral), date of birth, and age at secondary alveolar bone grafting.
Results
Of the 167 unilateral patients with cleft lip and palate and 66 patients with bilateral cleft lip and palate, 45% had symptoms of a fistula before alveolar bone grafting and 10% had symptoms of a fistula after surgery. There were no statistically significant differences between the presence of symptoms before or after secondary alveolar bone grafting between cleft types or by age at secondary alveolar bone grafting.
Conclusion
This is the first study examining the rates of fistula symptoms before and after secondary alveolar bone grafting in the United Kingdom. This study used the patient-centered outcome of the presence of symptoms as a way of measuring the presence of fistulas in this group. Secondary alveolar bone grafting reduces the incidence of symptomatic fistula in this setting.
Secondary alveolar bone grafting is an integral stage in the surgical management of children with cleft palates. This procedure aims to restore bone volumes in the tooth-bearing portion of the maxilla when a cleft defect has disrupted the development of bone in the area. Secondary alveolar bone grafting is recommended to be carried out when the patient is 9 to 11 years old, as this has been shown to result in the most favorable outcomes for facial growth and orthodontic treatment. One of the many roles of secondary alveolar bone grafting is to close oronasal fistulas, which are a recognized complication for children who have had primary cleft palate surgery (Fig. 1). Oronasal fistulas result in embarrassing symptoms of food and/or fluid regurgitation into the nose on eating or drinking, speech problems of hypernasality, audible nasal escape, and weakness of pressure consonants (Bureau et al., 2001).
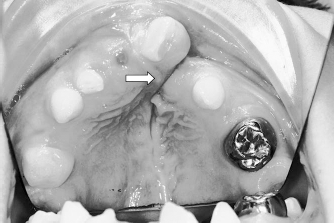
Cleft palate before secondary alveolar bone grafting showing fistula.
The existing literature reveals fistula rates of 1% to 57% (Cohen et al., 1991; Emory et al., 1997; Bearn et al., 2001; Muzaffar et al., 2001; Williams et al., 2001; Andersson et al., 2008; Lu et al., 2010; Maine et al., 2012). Previous studies have often excluded anterior, small, or alveolar fistulas in their data sets (Cohen et al., 1991; Emory et al., 1997; Muzaffar et al., 2001; Lu et al., 2010; Maine et al., 2012), however, which may, in part, explain this wide range of fistula rates. The risks associated with developing fistula has been a subject of controversy; studies have implicated cleft type, cleft severity, operator experience in primary repair of the palate, age at palatal closure, and other factors. However, there is no clear evidence demonstrating a definite association with any of these (Cohen et al., 1991; Kalaaji et al., 1996; Parwaz et al., 2009; Losken et al., 2011).
A 2006 study carried out in the southwest of England (Felstead et al., 2010) showed radiographically a high success rate (94%) using the Kindelan Index to assess bone height after secondary alveolar bone grafting compared with the national radiographic success rate (85%) (Revington et al., 2010). The 2006 study did not report on patient symptoms. It became apparent from clinical assessment of our patients that oronasal fistulas were causing symptoms, and this study aimed to quantify the rates before and after secondary alveolar bone grafting. This is the first time the effectiveness of surgery to eliminate these embarrassing symptoms has been quantified.
Methods
All patients being assessed for a secondary alveolar bone graft procedure were directly questioned before and 6 months after the procedure as to the presence of symptoms of an oronasal fistula, namely, food and/or fluid regurgitation on eating or drinking. For the purpose of this study, neither preoperative nor postoperative examinations were carried out to determine the location or presence of a fistula. The information was collected prospectively by the same individual (P.J.R.) at multidisciplinary cleft outpatient clinics throughout the southwest of England between October 2004 and May 2011. Data were collected on cleft type (bilateral or unilateral) and age at the time of the alveolar bone grafting procedure.
All secondary alveolar bone grafting procedures were carried out by the same surgeon (P.J.R.) using the tibia (n = 231) or iliac crest (n = 2) as a donor site.
Results
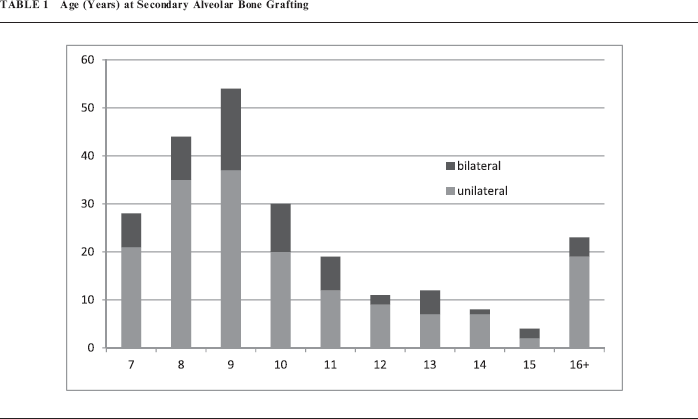
A total of 210 consecutive patients with cleft palate were included (representing 233 clefts: 167 unilateral and 66 bilateral) who required secondary alveolar bone grafting. The patients' age at secondary alveolar bone grafting ranged from 7 years 2 months to 52 years 2 months, though in most the procedure was done at 7 to 11 years old (n = 174). The median age of secondary alveolar bone grafting was 9 years, and the mean age was 11.4 years (Table 1).
Age (Years) at Secondary Alveolar Bone Grafting
The fistula symptom rate before alveolar bone grafting was 45% (105/233) (Table 2). The fistula symptom rate after surgery was 10% (24/233), with an odds ratio of 0.1 (95% confidence interval of 0.1–0.2). This demonstrates a 90% reduction in risk of fistula symptoms after secondary alveolar bone grafting.
Risk of Fistula Symptoms After Secondary Alveolar Bone Grafting

There was no statistically significant difference in risk of fistula symptoms between unilateral and bilateral types of cleft after secondary alveolar bone grafting (P = .424) (Table 2).
There was no statistically significant difference in risk of fistula symptoms between those patients that had secondary alveolar bone grafting at the recommended chronologic age of 9–11 years and those who had the procedure at a younger or older age for unilateral (P = .61) or bilateral (P =.194) clefts (Table 3).
Risk of Fistula Symptoms After Secondary Alveolar Bone Grafting, Comparing Age at Surgery and Cleft Type

Discussion
This study demonstrates a fistula symptom rate of 45% in a cohort of people with clefts in the southwest of England. After secondary alveolar bone grafting there was a 90% reduction in risk of fistula symptoms. This reduction in risk was not affected by the type of the cleft or the age at which the secondary alveolar bone graft was carried out.
Data were collected prospectively over a period of 6 years and 7 months (2004–2011). The results demonstrate a narrow confidence interval with an upper limit of 73% reduction in risk of fistula symptoms. The reduction in risk of fistula symptoms are representative of the current clinical situation as all secondary alveolar bone grafts were carried out by the same surgeon within the existing centralized cleft service.
This study used a patient-centered outcome measure to investigate the success of secondary alveolar bone grafting. We documented the patient's experience of fistula symptoms as these cause embarrassment for patients, and clinical examination may not always detect small fistulas. We were satisfied that direct questioning with a simple “yes or no” approach as to the presence or absence of symptoms was a quick, noninvasive, and cost-effective method to measure the effectiveness of this type of surgical repair.
Using a patient-centered measure may have resulted in overreporting of fistula rates, however, because of misclassification. Similar symptoms may occur with velopharyngeal incompetence and midpalatal fistulas, neither of which would be repaired by this procedure. Such misclassification could lead to an underestimate of effect size.
The fistula symptom rate before secondary alveolar bone grafting may not be representative of the current clinical situation, as this sample included persons who had had their primary palatal surgery before centralization.
This is the first United Kingdom series detailing the risk reduction of oronasal fistula symptoms in patients after secondary alveolar bone grafting. Previous studies of secondary alveolar bone grafting have focused on alveolar bone height as a measure of success but did not address the issue of patient symptom resolution (Revington et al., 2010).
The regionalization of cleft centers in the United Kingdom means there is now an opportunity to audit large case series. Future studies are needed to examine the fistula rates nationally and investigate the high rates of fistula in this population. Currently, the Cleft Care UK study is collecting data regarding the fistula symptom rate and anatomic location in the national United Kingdom population, and these data will be available in the near future.
Conclusion
This is the first report of fistula symptom rates in the United Kingdom and demonstrates the effectiveness of secondary alveolar bone grafting to reduce the risk of fistula symptoms. Fistula symptoms are a useful patient-centered outcome measure of the success of secondary alveolar bone grafting.