
Abstract
Objective
To photogrammetrically objectify changes in nonsynostotic craniofacial deformity in orthotically treated versus untreated infants.
Design
A statistical retrospective pairwise comparison of two respective three-dimensional (3D) photo scans of 80 children performed in a 6-month time lag.
Patients
Two comparable samples of children (40 treated, 40 untreated) with nonsynostotic cranial deformity.
Interventions
Respective 3D photo scans were matched using Cranioform Analytics 4.0 software.
Main Outcome Measures
Median change of 30° Cranial Vault Asymmetry Index (CVAI), modified CVAI (CVAImod), Cranial Index (CI), and posterior symmetry ratio (PSR).
Results
We found an improvement in Δ30° CVAI by 3.3% (treated) and by 1.31% (untreated), respectively. CVAImod improved by 3.46% in the treated group and by 1.55% in the untreated group. CI improved by 4.41% in the treated group and by 3.68% in the untreated group, and PSR improved by 0.71 in the treated group and 0.49 in the untreated group. Although improvement of cranial asymmetry was higher in those children treated with an individual molding orthosis, we could not document a statistically significant difference between the two groups.
Conclusions
Helmet therapy may be less appropriate for the correction of brachycephaly than for cranial asymmetry. Nonsynostotic cranial deformity shows some spontaneous correction. Photogrammetry presents an accurate method to objectify craniofacial changes in early infancy.
A new problem arose after international pediatric societies advocated the bedding of infants in an exclusively supine position to prevent sudden infant death in the first year of life (American Academy of Pediatrics, 1992). Shortly thereafter, various centers observed a vast increase in positional cranial deformity (Argenta et al., 1996; Kane et al., 1996; Turk et al., 1996). Advances in the treatment of this new symptom have ranged from physiotherapeutic or osteopathic modalities (Moss, 1997; Pollack et al., 1997; Lessard et al., 2011) to the use of individual molding ortheses (Blecher et al., 1998; Littlefield et al., 1998). Some authors (Hutchison et al., 2004) described the spontaneous regredience of nonsynostotic cranial deformities in the first years of life, whereas others (Najarian, 1999; Teichgraeber et al., 2002; Biggs, 2003; Kluba et al., 2011) advocated early treatment to prevent sequelae in later life.
Most classifications and objectifications of cranial deformity are anthropometric (Wilbrand, Schmidtberg, et al., 2012), but radiographic (Bruner et al., 2004) and photographic (Loveday and de Chalain, 2001; Hutchison et al., 2005; van Vlimmeren et al., 2006) methods have also been used. These methods, however, provide only a two-dimensional representation of a three-dimensional cranial deformity. Nevertheless, based on these examination methods, different classification schemes for positional cranial deformities have been proposed (Argenta et al., 2004; Wilbrand et al.; 2008, Wilbrand, Schmidtberg, et al., 2012).
Currently, some health care professionals assume that nonsynostotic cranial deformities do not require helmet therapy because of the spontaneous disappearance of the condition during physiologic cranial growth, motor development, and increased verticalization.
A new instrument was developed to objectify cranial growth and shape and to provide a three-dimensional representation of cranial deformities in infants (Kau et al., 2007) in an easy, accurate, fast, and examiner-independent manner (Wong et al., 2008; Schaaf, Pons-Kühnemann, et al., 2010; Schaaf, Wilbrand, et al., 2010; Wilbrand, Szczukowski, et al., 2012). In this observational trial, we used this technique with specially developed software to evaluate a cohort of treated and untreated children with similar nonsynostotic cranial deformities. We sought to answer a recurrent question in the literature: To what degree does nonsynostotic cranial deformity in early life resolve properly without treatment using individual cranial orthoses?
Patients and Methods
In this retrospective observational study, a list of 40 treated and 40 untreated children (n = 80) was identified. Inclusion criteria were the availability of two photo scans taken at an approximate interval of 6 months and adequate age (approximately 6 months) at the initial assessment. For the untreated patients group, 40 children with the highest Cranial Vault Asymmetry Index (CVAI) values were selected from a sample of 120 untreated and photogrammetrically scanned children with nonsynostotic cranial deformities. To obtain comparability of cranial deformity between the groups, we selected 40 children with the lowest CVAI value from a group of 426 orthotically treated infants. All children had been seen at our center between January 2010 and January 2012. Clinical indication for helmet treatment had been established before, when a significant positional cranial deformation was found according to previously published articles (Wilbrand, Schmidtberg, et al., 2012). Most patients in the untreated group were not treated due to mild or moderate deformity, advanced age at first assessment, or absence of parental request for treatment. Physiotherapy and bedding maneuvers were recommended to this group. The local ethics committee approved the study in advance. Two three-dimensional photographic scans were obtained at an approximate interval of 6 months (pre- and posttreatment in the treated group) for each patient using a Vectra 360 four-pod imaging system (Canfield Scientific Inc., Fairfield, NJ). The two scans were matched and analyzed automatically using the Cranioform Analytics 4.0 software (Cranioform AG, Alpnach, Switzerland).
All children could be classified as plagiocephalic, brachycephalic, or both due to a definite aberrance in anthropometrically measured modified CVAI (CVAImod) or Cranial Index (CI).
Each pair of scans was matched using a triangle defined by the following landmarks: right tragus (Trr), left tragus (Trl), and subnasale (Sn). The midpoint (mp) was defined as the center of the Trr–Trl line, the x-axis was defined perpendicular to the Sn–mp line, and the z-axis was defined perpendicular to both axes through the vertex of the head. The software used in this study automatically calculated the following parameters: cranial circumference (in centimeters), defined as the course around the head at a preliminarily defined level; cranial length (in centimeters), measured through mp; cranial width (in centimeters), defined as the length of the x-axis through mp; diagonals A and B, measured from one frontotemporal side to the contralateral lambdoidal region, with diagonal A defined as the shorter measurement; CVAImod, which reflects the asymmetry between diagonals A and B independent of cranial size according to standardized anthropometric caliper measurements (Wilbrand et al., 2011) for all planes {CVAI = [(diagonal A – diagonal B)/diagonal A] × 100}; CVAI, which reflects the asymmetry between the 30° transcranial diagonals as described by Loveday and de Chalain (2001); CI, which reflects brachycephaly [CI = (cranial width/cranial length) × 100]; and posterior symmetry ratio (PSR), the ratio of the maximum posterior volume to the minimum posterior volume (PSR = Qmax/Qmin) independent of the affected side (perfect symmetry = 1).
Cranioform Analytics 4.0 divides the entire neurocranium into 11 levels of equal height. We preliminarily defined plane 5 as the relevant level for our evaluation and measured circumference, length, width, and diagonals A and B in this plane (Fig. 1).
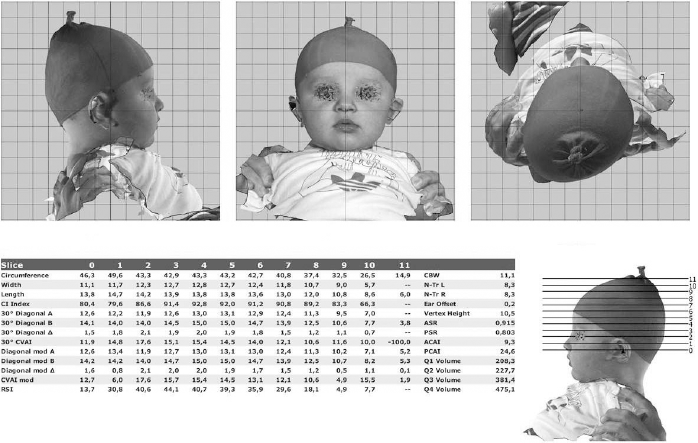
Automated analysis of positional head deformity by Cranioform Analytics 4.0 software.
All three-dimensional photogrammetric measurements were analyzed using a pairwise comparison statistical analysis.
Data analysis was performed by SPSS Version 20 (IBM SPSS Statistics 20, IBM GmbH, München, Germany). If data were asymmetrically distributed, normalization was performed by logarithmic transformation. A linear mixed model was used to analyze the repeated-measure design. Statistical significance was assumed if P < .05. Differences between groups were presented as mean ± SEM or mean ±SD.
Results
The mean age of untreated infants was 203.6 days (SD, 60.64) or 6.79 months at the first photo scan and 371.7 days (SD, 131.65) or 12.39 months at the end of our study interval. The mean age of treated infants was 195.9 days (SD, 34.91) or 6.5 months at the beginning of our study and 352.2 days (SD, 136.30) or 11.74 months at the end of the treatment interval. The groups were equalized regarding age distribution at the beginning of our trial, with a statistically insignificant difference between the groups (P = .49). Likewise, changes to the mean cranial circumference of our study cohort did not differ significantly between the groups (3.1 cm (untreated) versus 2.7 cm (treated), respectively (P = .181). Overall, 21 (26.3%) children were female and 59 (73.8%) were male.
Using the mixed-model analysis, we found significant interaction between the two groups (helmet treatment versus no treatment) regarding CVAImod (P < .001). Difference between the mean CVAImod of the two groups was different at the initial examination (CVAImod treated: 5.96%, SEM 0.352 versus untreated: 4.50, SEM 0.290, P = .001). This difference became insignificant at the final examination (CVAImod treated: 2.50% [ΔCVAImod 3.46%)] SEM 0.347 versus untreated: 2.95% [ΔCVAImod 1.55%], SEM 0.302, P = .294; Fig. 2).
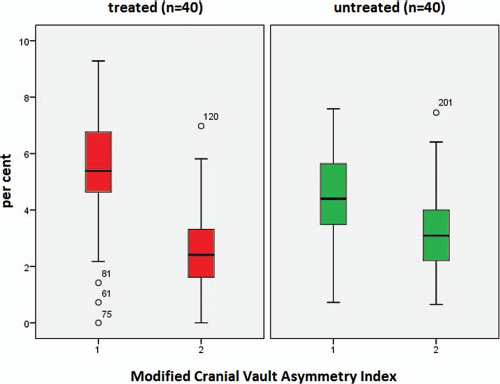
Median initial and final modified Cranial Vault Asymmetry Index (CVAImod) in treated (red) and untreated (green) infants.
For the 30° transcranial CVAI, we also found significant interaction between the groups (P < .001). The groups were significantly different at the origin (30° CVAI treated: 6.72%, SEM 0.388 versus untreated: 5.44%, SEM 0.317, P = .008). After the study interval, the difference between the groups was insignificant (30° CVAI treated: 3.42% [Δ30° CVAI 3.3%], SEM 0.384 versus untreated: 4.13% [Δ30° CVAI 1.31%] SEM 0.328, P = .141; Fig. 3).
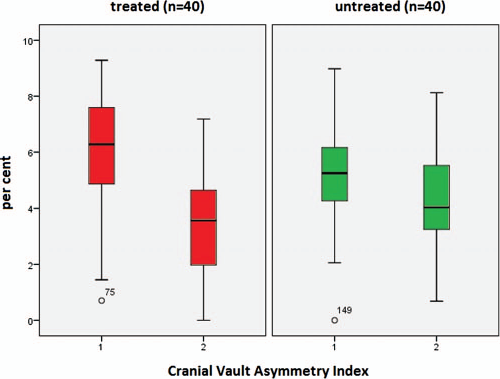
Median initial and final 308 transcranial Cranial Vault Asymmetry Index (CVAI) in treated (red) and untreated (green) infants.
Regarding the mean CI, we did not find a significant interaction (P = .172) between the two groups. A difference between helmet and nonhelmet treatment for the correction of brachycephal deformity therefore could not be observed in our trial. There was no significant difference in the initial values for CI (CI treated: 93.11%, SEM 1.113 versus untreated: 92.46%, SEM 0.892, P = .646) and no significant difference at the endpoint of our study (CI treated: 88.70% [ΔCI 4.41%], SEM 1.109 versus untreated: 88.78 [ΔCI 3.68], SEM 0.902, P = .958; Fig. 4).
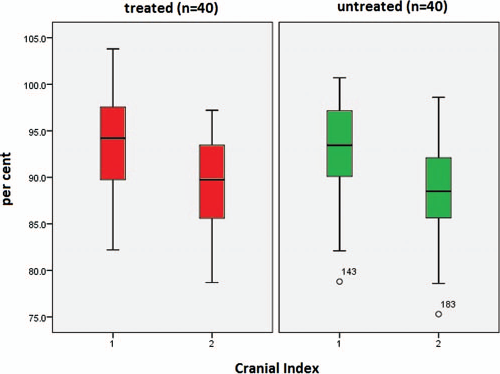
Median initial and final Cranial Index (CI) in treated (red) and untreated (green) infants.
For the volumetric PSR value, which includes the overall posterior cranial symmetry, we found no significant interaction between the two groups (P = .124). We found no significant difference between the groups at the origin of our study (PSR treated: 8.54, SEM 0.12 versus untreated: 8.78, SEM 0.1, P = .104) and no significant difference at the final point (PSR treated: 9.25% [ΔPSR 0.71], SEM 0.12 versus untreated: 9.27 [ΔPSR 0.49], SEM 0.11, P = .870; Fig. 5).
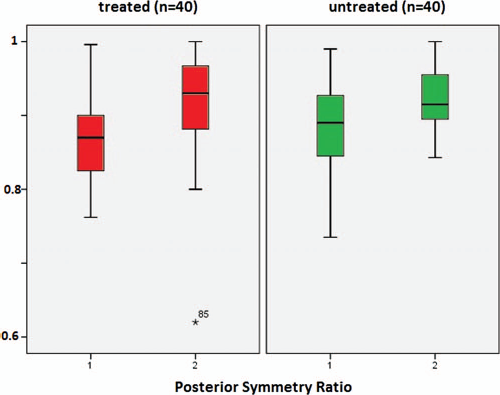
Median initial posterior symmetry ratio (PSR) in treated (red) and untreated (green) infants.
Discussion
Three-dimensional photogrammetry is a safe, fast, and easy-to-use method in pediatric craniofacial treatment and documentation (Wong et al., 2008; Schaaf, Wilbrand, et al., 2010). Positional cranial deformity in early childhood is a topic of lively discussion among practitioners worldwide. Current reviews of existing trials (Bialocerkowski et al., 2008; McGarry et al., 2008) have revealed that only fair-quality studies have been conducted to date. No observational study comparing spontaneous craniofacial changes with changes during helmet therapy has obtained highly significant statistical results. The present study was designed to conduct such an analysis and to assess medium-term cranial changes in an examiner-independent manner. The presented results, however, are still not suitable to certainly compare the course of cranial deformation with or without a helmet treatment. The absolute amount of positional cranial deformation shows statistically significant difference between the two groups. The overall clinical dimension (mild to moderate deformity), however, is equalized to some extent. The higher number of treated children (n = 426) versus the smaller number of untreated patients (n = 120) in our cohort is most likely due to a preselection process. Most children being presented to a specialized center have previously been examined by a family physician or pediatrician. Therefore, a much higher number of children with imposing cranial deformities are available for scientific assessment.
Hutchison et al. (2004) studied the natural history of nonsynostotic cranial deformity over a 2-year period and found significant spontaneous improvement in plagiocephaly, as demonstrated by oblique cranial length ratios. Vles et al. (2000) found significant differences in the correction of positional cranial deformity by orthotic helmet therapy compared with physiotherapeutic maneuvers alone. Our findings cannot confirm or confute these results, but they are based on objectified data, whereas Vles et al. classified plagiocephaly using a cosmetic outcome score with only fair reliability and Hutchison used a two-dimensional photogrammetric method.
Loveday and de Chalain (2001) found similar improvements in cranial shape by active counterpositioning and orthotic treatment (1.8% and 1.9% change in 30°CVAI, respectively). In our study, changes in 30°CVAI were greater in the group of orthotically treated children (3.3% improvement in the treated group versus 1.3% improvement in the untreated group). Loveday and de Chalain (2001) did not report changes in CI, CVAImod, or PSR.
The differences in improvement of CVAImod between the two groups show the most obvious divergency (ΔCVAImod treated: 3.46% versus untreated: 1.55%). CVAImod reflects the parameter obtained by direct anthropometric caliper measurements of the infant cranium as defined before (Wilbrand et al., 2011). Statistical significance regarding the improvement of asymmetric cranial deformity, however, could not be demonstrated. Nevertheless, we showed a difference in the individual impact on cranial asymmetry between the groups: significant interaction was shown for 30° CVAI and CVAImod.
The overall volumetric parameter PSR, however, was never analyzed in a study regarding nonsynostotic cranial deformation. Although we expected significant differences in improvement of this parameter, our results show that both groups improved to some extent (ΔPSR treated: 7.1% versus untreated 4.9%). Although improvement was clearly better in the treated group, the difference between treated and untreated infants was not significant after all.
Improvement of brachycephaly appears to be very similar in both of our study groups (ΔCI treated 4.41% versus untreated 3.68%). This finding might confirm the results obtained by Hutchison et al. (2004) and Teichgraeber et al. (2004), who found that orthotic helmet therapy was not so effective for the correction of positional brachycephaly. However, whether helmet treatment has a hard indication for the correction of positional brachycephaly must be subjected to more extensive studies.
Helmet treatment is aligned with significant cost to caregivers or insurance companies. To minimize the trend of cumulative financial strain, the indication for helmet treatment should be adjusted to some extent. Correction of mild to moderate nonsynostotic cranial deformities with alternative methods necessitates a prolonged period of time and is assumed to result in a less satisfying final outcome in most studies (Xia et al., 2008). It is not yet clear whether cranial shape improves in total without molding helmets. Nevertheless, cost-effectiveness in health systems might be one applicable argument against helmet treatment for children with mild to moderate cranial deformity.
Three-dimensional photogrammetry is playing an increasingly important role in craniofacial diagnostics (Wong et al., 2008; Schaaf, Pons-Kühnemann, et al., 2010; Schaaf, Wilbrand, et al., 2010) because it is easy to use, fast, examiner independent, reliable, and avoids exposure to radiation (Bruner et al., 2004). Computerized analysis of three-dimensional photography using special software avoids measurement mistakes and failure due to subjective appraisals of patients' clinical appearance (Wilbrand, Szczukowski, et al., 2012).
The results of this study indicate that asymmetric positional cranial deformity improves to some extent within a 6-month period if no orthotic treatment is initiated. Improvement is increased, however, with an orthotic therapy. In contrast to our expectations, however, we did not find statistical significance in our parameters.
Prospective randomized trials on treatment outcome versus nontreatment outcome would not be sufficient to obtain equality of the analyzed groups or flawed with ethical concerns. A retrospective matched-pair trial regarding age and to some extent severity of cranial deformation therefore was initiated to improve the statistical impact of the existing scientific base. Matching, however, could not be perfectly implemented, although we selected the mildest cases in the treated group against the most serious cases in the untreated group. Thus, as a limiting factor regarding the generalizability of our results, it must be considered that the analyzed children herein did not show severely deformed heads but mild to moderate cranial deformation. Further long-term studies of craniofacial changes in patients with positional deformities are currently implemented. In addition, a photogrammetric analysis regarding the individual groups of nonsynostotic cranial deformity and untreated patients with severe cranial deformation could improve the existing scientific data.
Conclusions
The present study reports on the first photogrammetrically based evaluation of craniofacial changes with and without orthotic therapy over a 6-month period. Three-dimensional photogrammetry is suitable and of high significance to monitor the course of different craniofacial deformities. The generalizability of our results is weakened, however, by the selection bias and lack of comparability between the groups at baseline.