
Abstract
Background
Secondary deformities are common in people born with unilateral cleft lip and palate. In recent years, more and more attempts and efforts have been directed toward muscle reconstruction. The authors present a new method of orbicularis oris repair in correction of secondary cleft lip deformities.
Methods
From April 2009 to April 2013, a total of 28 patients underwent this procedure in the authors' department and had a follow-up with a minimum length of 1 year. Muscle reconstruction was divided into three units that deal with the nasal floor, white lip, and red lip. Common anatomical pathologies including a deviated columella, blunted alar-facial groove, lack of philtral column, “free border” deficiency, and unapparent vermilion tubercle can be corrected in a single operation.
Results
The average follow-up period was 14.6 months (range, 12 to 24 months). Contractubex gel (Merz Pharma, Frankfurt, Germany) was used to treat prominent or reddish scars in 16 patients. No major complications occurred. All the patients were satisfied with their nasolabial appearance.
Conclusions
“Three-unit” muscle repair was found to be effective and practical in secondary repair. Improved aesthetic and functional results can be achieved with this comprehensive procedure.
Secondary deformities are common in people born with unilateral cleft lip and palate. They vary in severity and form depending on the inherent tissue deficiency, operative methods, operator experience, and variable of growth (Stal and Hollier, 2002; Ferrario et al., 2003). Thus, secondary procedures are frequently more complex than initial surgeries. More and more attempts have been directed toward musculature repair in recent years (Suzuki et al., 2000). This article describes the corresponding author's method of muscle reconstruction in secondary cleft lip repair, which has been more or less routine in our department.
In this approach, muscle reconstruction is divided into three units that deal with the nasal floor, the white lip, and the red lip (Fig. 1). Under normal conditions, the nasal floor unit includes the nasal bundle and some fibers from the levator labii superioris and levator labii superioris alaeque nasi; the white lip unit mainly consists of the nasolabial bundle; the red lip unit corresponds to the deep orbicularis oris muscle. However, in the secondary cases of cleft lip, the nasal floor unit is the muscle located at the nasal floor; the red lip unit is defined to be the muscle in the vermilion region; the white lip unit is the muscle part between them.
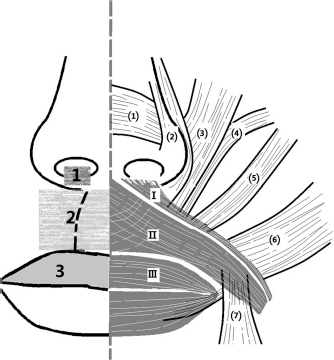
Three units in muscle reconstruction. 1: nasal floor unit; 2: white lip unit; 3: red lip unit. (1): nasalis; (2): levator labii superiors alaeque nasi; (3): levator labii superioris; (4): zyomaticus minor; (5): zyomaticus major; (6): buccinator; (7): depressor anguli oris. I: nasal bundle; II: nasolabial bundle; III: deep part of the orbicularis oris muscle.
The main purpose of this method is to correct the displacement of the upper lip. Common anatomical pathologies including (1) deviated columella, blunted alar-facial groove, (2) lack of philtral column, and (3) “free border” deficiency (Chen et al., 1995) and unapparent vermilion tubercle can be corrected in a single operation. The free border of the lip represents the red border of the lip. A persistent lateral muscle bulge and depressed nasal floor can be improved, but it is difficult to achieve symmetry by this method alone.
Method
Design
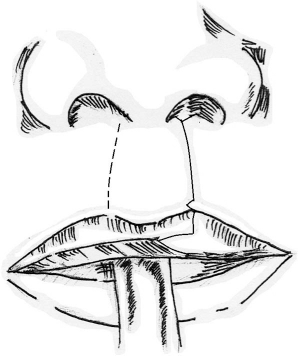
The design of the incision basically depends on the shape of the original scar and width of nasal floor (Fig. 2). A small triangular white roll-cutaneous tenon was designed at the vermilion border laterally. A vertical triangular vermilion flap was drawn along the border of the vermilion defect, with its tip pointing toward the peak of the Cupid's bow. The length and width of the flap varied in accordance with the amount of the tissue needed to create the vermilion tubercle.
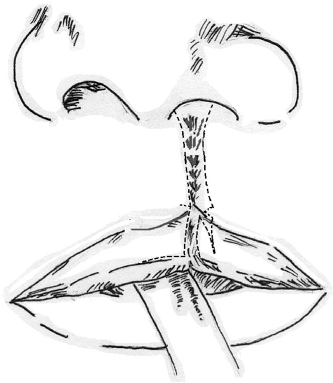
Design for “three-unit” repair (frontal view).
Dissection
Skin was dissected from the nasal floor unit and white lip unit muscle on both the medial and lateral sides of the cleft (Fig. 3). Medially, the dissection of the white lip unit should not cross the midline. Laterally, the dissection of the nasal floor unit stopped just short of the alar groove; for the white unit, dissection was carried over for 8 to approximately 10 mm. The two units were separated from the underlying submucosa and mucosa and also from the maxilla. The subcutaneous tissue below the columella was dissected to expose the anterior nasal spine. The red lip unit was separated from the glandular tissue of the adjacent mucosa. The triangular tenon at the vermilion border was created with muscle 1 mm thick. Correspondingly, a mortise was made at the medial vermilion-cutaneous junction. The laterally based triangular vermilion flap was constructed on the lateral side. A split extended medially along the red line (Noordhoff, 1984).
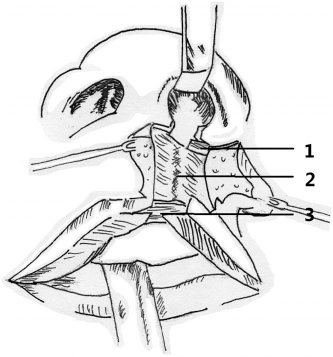
Dissection of nasal floor unit, white lip unit, and red lip unit (basal view). ②: anterior nasal spine; 1: nasal floor unit; 2: white lip unit; 3: red lip unit.
Reconstruction
The nasal floor unit was brought toward the midline and sutured to the base of the columella. Following this, the white lip unit was reconstructed in two stages. The first stage was adequate rerotation and advancement of the lateral flap. The cephalic portion of the lateral flap was anchored to the periosteum of the anterior nasal spine. Clear nylon or other permanent suture was used (Fig. 4). The second stage is the functional reconstruction of the philtral column. A lateral muscle flap was partially split into two leaves along the coronal plane. The lower leaf was sutured to the corresponding portion on the medial side end to end. The upper leaf and the medial flap were sutured together with a horizontal mattress suture to create a vertical interdigitation. These mattress sutures were placed so that the first pass started through the upper leaf and the entire muscular layer of the medial flap; the second pass went through the dermis at the intended location of the philtral dimple, then through the upper leaf. Usually, two sutures were needed at the midpoint and the cutaneous-vermillion junction (Fig. 5). Then the red lip unit was reconstructed by end-to-end anastomosis. The triangular white roll-cutaneous tenon in the lateral lip element filled the mortise on the medial side; whereas, the laterally based vermilion flap was inset into the notch along the red line (Fig. 6). Finally, when muscle suturing was finished, excessive skin was discarded and skin was closed.
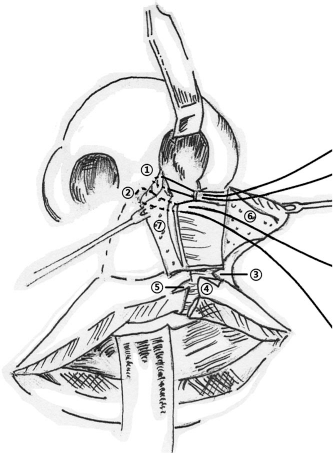
Reconstruction of nasal floor unit and location of the lateral flap (basal view). ①: the base of the columella; ②: anterior nasal spine; ③: the triangular tenon at the vermilion border; ④: vertical triangular vermilion flap; ⑤: the notch along the red line; ⑥: skin on the lateral side; ⑦: skin on the medial side.
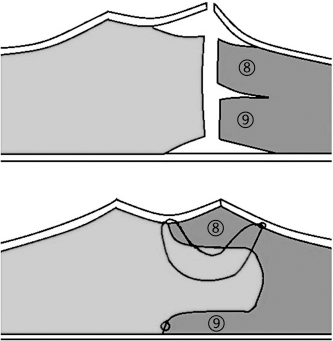
Formation of philtral column (horizontal section of the upper lip). ⑧: upper leaf; ⑨: lower leaf.
Skin closure (frontal view).
Results
The study protocol was approved by the Independent Ethics Committee of Shanghai Ninth People's Hospital affiliated with the Shanghai Jiaotong University School of Medicine. Informed consent was obtained from all patients or their parents. From April 2009 to April 2013, there were 28 consecutive patients who received reconstruction using the aforementioned method and were reviewed at a minimum of 1 year (11 men and 17 women; mean age of 21 years, range, 18 to 28 years). They received primary cleft lip repairs and palate repairs at other institutions. No patient received orthognathic surgery. A combination of secondary deformities was present in the study population, including unapparent alar-facial groove, a deviated columella, unapparent or grooved philtrum, central vermilion insufficiency, and poor lip scars.
The corresponding author did all the surgeries. There were no surgical complications such as infection, bleeding, or flap necrosis. Contractubex gel (Merz Pharma, Frankfurt, Germany) was used to treat prominent or reddish scars in 16 patients. It was used in accordance with patients' requirements and economic conditions. For most patients, a minimum of 4 months was required for the scars to become inconspicuous, and Contractubex gel (Merz Pharma) appeared to hasten the resolution. After an average follow-up of 14.6 months (range, 12 to 24 months), all the patients were satisfied with their nasolabial appearance and found the scars to be acceptable.
Discussion
Secondary deformities of the cleft lip are the rule rather than the exception. They are varied in both appearance and etiology. Comprehensive muscle reconstruction must be based on a thorough knowledge of normal anatomy and a proper understanding of such displacements as may occur (Nicolau, 1983).
The normal orbicularis oris muscle is well described. It is divided into superficial and deep components, corresponding to the double function of the muscle. The superficial part is subdivided into upper and lower bundles. The upper or nasal bundle derives its fibers from the zygomaticus major and minor, the levator labii superioris, and the levator labii superioris alaeque nasi. They insert into the anterior nasal spine, the septo-premaxillary ligament (Latham, 1970), and the nostril sill, passing deep to the alar base. The lower or nasolabial bundle derives its fibers from the depressor anguli oris muscle on each side. Its fibers insert in the skin, forming the philtral ridges. Short fibers end in the ipsilateral ridge; whereas, long fibers decussate in the midline to insert into the contralateral ridge. The deep part runs under the vermilion from one modiolus to the other. Its lower border curls upon itself, forming the vermilion by everting the mucous membrane (Nicolau, 1983). Eversion of the deep part forms the tubercle of the lip (Latham and Deaton, 1976).
When the mouth is pursed, contraction of the deep part thickens the vermilion and lengthens the upper lip height. Simultaneous relaxation of the superficial part produces numerous perioral fine wrinkles, accentuates the philtral columns, and flattens the nasolabial folds. When the mouth is open, the contraction of the superficial part flattens the perioral fine wrinkles and philtral columns, accentuates the nasolabial folds, and shortens the upper lip height. Simultaneous relaxation of the deep part decreases the thickness of the vermilion (Park and Ha, 1995).
The nasal bundle on the cleft side is attached to the lateral aspect of the nasal ala. The muscle on the noncleft bundle appears to be unaffected. Muscle imbalance might lead to a less obvious alar groove, depressed and wide alar base, and deviation of the columella. Nasal bundle reconstruction provides support for nasal tip projection and symmetry. Nicolau (1983), Seagle and Furlow (1993), and Suzuki et al. (2000) gave priority to the restoration of the depressed nasal floor and displaced alar base. The nasal bundle was freed and sutured either to the nasal spine or to the periosteum just below the spine, bringing the alar base forward. Delaire's anatomical theory (Delaire, 1978; Markus and Delaire, 1993) led to wide subperiosteal undermining to achieve complete freeing of the muscle. Differently from our procedure, the “paranasal muscle” was anchored to the base of the nasal septum, behind the anterior nasal spine.
Nasolabial bundle distortion by the cleft has been described in electrical stimulation and histologic studies (Nicolau, 1983; De Mey et al., 1989). On the cleft side, the lateral part seems totally normal. However, the muscle changes in direction below the displaced alar base to run almost vertically. It is abnormally attached to the nostril and the periosteum of the pyriform aperture. During contraction, a lateral bulge presents with a contour deficiency between the bulge and alar base. On the noncleft side, the nasolabial bundle appears to be unaffected. Nevertheless, the normal bilateral insertion of the muscle fibers is disrupted. Displaced muscle, lateral bulge, and unobvious philtral ridge are common secondary deformities. Various techniques have been described to create a better orbicularis junction. Anchoring the cephalic portion of the orbicularis to the periosteum of the anterior nasal spine helps to centralize the lip. Though this step recreates the clefted or scarred pathology, it has been shown to be stable and has been used by many surgeons (Nicolau, 1983; Markus and Delaire, 1993; Suzuki et al., 2000; Seagle and Furlow, 2004; Matic and Power, 2011). The lateral bulging prominence have been shown to be associated with greater orbicularis oris thickness and levator width on the cleft side (Power et al., 2010). It can be eliminated by a complete orbicularis oris takedown and new muscle insertions (Seagle and Furlow, 2004; Matic and Power, 2011). The philtrum can be created by increasing muscle thickness and creating laxity on the skin. “Basket-weave” muscle repair grossly mimics the microscopic interlacing of the superficial orbicularis fibers (Seagle and Furlow, 2004). Cho and Baik (2000) introduced the vertical interdigitation of orbicularis oris muscle flaps. Kim et al. (2007) and Cakir (2009) partially split the muscle flap along the coronal plane and increased the muscle height by eversion of the muscle fibers. Soft tissue augmentation or cartilage graft in some cases can elevate the philtral column (Schmid, 1964; Lim et al., 2012); yet, extra scars, unnatural contour, and lack of dynamic properties limit their use.
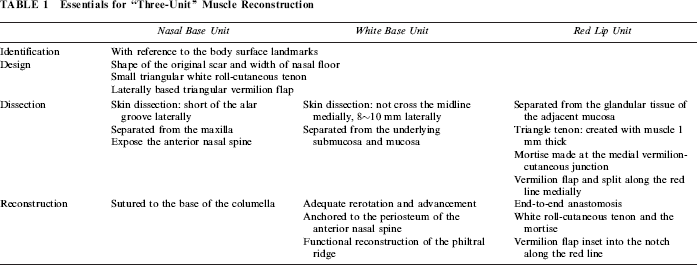
In clefts, the deep part of the orbicularis oris muscle does not reach the extremity of the interrupted vermilion. Muscle fibers are not distorted but simply interrupted (Nicolau, 1983; De Mey et al., 1989). The free border of the lip consists of the deep part of the orbicularis oris muscle and its overlying subcutaneous tissue, vermilion, and mucosa. The deformity in this area may involve any or all of these components. The tubercle of the lip is not apparent. Reapproximation of the deep part must be done especially carefully to avoid secondary contraction. Accurate reconstruction of the deep part is beneficial for vermilion repair. First, orbicularis oris continuity is a prerequisite for a better vermilion contour (Rodgers and Mulliken, 1989; Stal and Hollier, 2002). Second, a more natural tubercle and central lip element can be created only by accurate muscle diastasis in some cases (Assunção et al., 2006; Grewal et al., 2009). The triangular tenon at the vermilion-cutaneous junction is created to achieve elongation of the medial element and carry the white roll to the medial side of a unilateral cleft lip. However, there are different opinions about its design, location of the mortise, and even the necessity to apply this procedure (Onizuka, 1980; Mulliken and Martínez-Pérez, 1999; Suzuki et al., 2000; Guyuron et al., 2009). The nasal bundle, nasolabial bundle, and deep part of the orbicularis oris muscle should be repaired independently to fulfill their separate function (Nicolau, 1983). We have presented in Table 1 the essentials for this surgical approach.
Essentials for “Three-Unit” Muscle Reconstruction
Identifying and separating the three parts of the orbicularis oris muscle is basic and critical for the best functional and aesthetic result. Because all the patients received their preliminary procedures using different methods in different hospitals, the relationship of the muscle subunits are likely to be altered, adding to the trouble of discrimination. In our 3 years' experience, it has been practical to subdivide the muscle units with reference to the body surface landmarks. Electrical stimulation at the time of operation can be very helpful in complicated cases.
In nasal floor unit repair, skin dissection should not exceed the alar groove; otherwise, the pull tension to the inferolaterally displaced alar base will be decreased, contributing to a poorer alar-facial groove. The nasal floor unit is elevated and sutured to the base of the columella instead of the anterior nasal spine. Because deviation of the columella is partly caused by muscle balance, this step helps to correct the deviated columella to some extent (Fig. 7). Furthermore, it can not be fully corrected because deviated columella are likely tied to underlying septal deviation and a displaced anterior footplate. Nasal bundle reconstruction alone may not be enough to restore the nasal sill symmetry. There are at least two primary reasons for the outcome. First, there was not sufficient or available muscle in nasal floor unit from primary surgery. Second, the nasal floor was not raised overcorrectively. Postoperative scarring and retrogression may play roles in the recurrence of nasal sill depression. Third, this problem almost always relates to deficiency of the bony base and an inherent tissue deficiency, which can be improved by alveolar cleft repair and then a graft of autogenous tissue such as cartilage, fat tissue, or dermis or by the placement of artificial material such as silicone or hydroxyapatite.
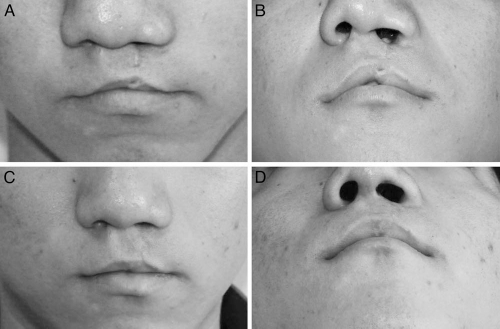
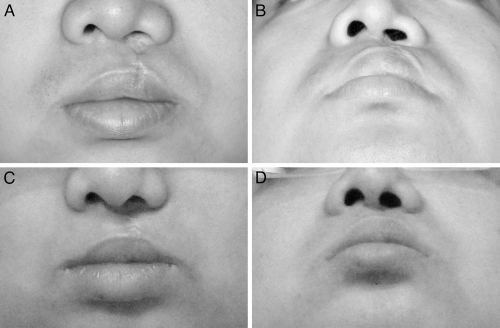
Patient 1: 21-year-old man. Left complete cleft lip and palate. A, B: Preoperative view. C, D: 12 months after secondary repair.
As to the white lip unit, the skin dissection in the medial flap should be restricted to within 5 mm and avoid crossing the midline to preclude effacing the natural philtral pit. Complete freeing of the nasolabial bundle is very important in that it allows adequate rerotation and advancement to the correct position. According to a literature survey (Nicolau, 1983), the nasolabial bundle can be reattached to the inferior part of anterior border of the nasal septum, the anterior nasal spine, and to the muscles of the opposite side. Although reattachment to the muscle on the medial side is more coincident with the normal anatomy, only the insertion into a bony projection-the anterior nasal spine will reach strong stability and establish the muscle balance needed for proper height of the skin (Fig. 4). We perform a two-layer approximation to accomplish precise muscle alignment, create a prominent philtral column and normalize orbicularis anatomy postoperatively at the repair site (Fig. 5). This procedure minimizes wound tension and provides excess skin through the vertical interdigitation. It is necessary for both creating a dominant philtral column and improving the cosmetic outcome of scar. The new philtral column should be created overcorrectively because it will decrease due to the lip movement. The philtral dimple is accentuated by grabbing the dermis at the midline, making the column more apparent (Fig. 8). The lateral bulging prominence is proved to be associated with greater orbicularis oris thickness and levator width on the cleft side (Power et al., 2010). Its correction remains a difficult problem. The lateral bulge did not seem to be significantly improved, perhaps because the skin dissection on the lateral side is not adequate and not all muscle was adequately freed from abnormal attachment to the lateral nasal base. In the future we will try wide dissection over the entire muscle bunching area.
Patient 2: 23-year-old man. Left complete cleft lip and palate. A, B: Preoperative view. C, D: 13 months after secondary repair.
In red lip repair, muscle in the vermilion is reconstructed by careful end-to-end anastomosis. We lay special stress on the two external triangles. Both the flaps must be created with muscle. In this way the flap circulation can be improved, thus minimizing scarring. A small triangular tenon is designed 1 mm above the vermilion border, making the vermilion everted and improving the groove line (Fig. 9). The triangular vermilion flap rotates almost 90° to enlarge the median tubercle and obliterate the vermilion defect.
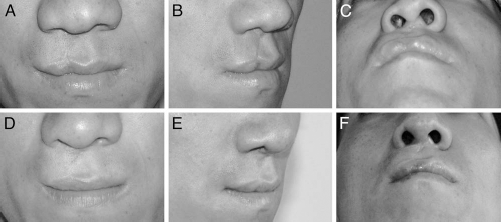
Patient 3: 27-year-old man. Right complete cleft lip and palate. A–C, Preoperative view. D, E: 19 months after secondary repair.
Conclusion
Our proposed procedure is standard and easy to learn. It is based on a proper anatomical assessment and efficiently improves the secondary lip deformities outlined here. Improved aesthetic and functional results have been achieved with this comprehensive procedure.
Footnotes
Acknowledgments
Thanks are due to Wei Zhang for assistance with the figures and for valuable discussion.