
Abstract
Objectives
Can a synthetic bone substitute be used to repair the alveolar cleft to bypass donor site morbidity as well as to shorten the operating time? In earlier experimental studies, micro-structured beta-tricalcium phosphate (β-TCP) provided similar bone healing when compared with grafting with iliac crest bone. This justifies the clinical evaluation of this bone substitute in the human alveolar cleft situation.
Design
Prospective clinical study.
Setting
University clinic.
Participants
Seven patients, all with unilateral alveolar cleft, were randomly included for alveolar cleft repair with β-TCP in 2010 and 2011.
Main Outcome Measures
In all patients, the alveolar cleft was repaired by micro-structured β-TCP grafting. Our assessments were distilled from cone beam computed tomography scans taken preoperatively, 1 week postoperatively, and 6 months postoperatively. A volumetric outcome could be realized.
Results
Six months after the operative grafting of micro-structured β-TCP into the alveolar cleft, the bone volume thus acquired was satisfactory. We found an average bone volume percentage of 73% ± 6% compared with the original cleft volume.
Conclusions
Previous experimental and clinical studies and the initial findings of this pilot study now elucidate a path toward the clinical use of micro-structured β-TCP bone substitute for repair of the alveolar cleft.
The incidence of congenital facial clefts varies throughout the world and between ethnic groups (Gundlach and Maus, 2006). In Europe, the occurrence of clefts of lip, alveolus, and palate among Caucasians has been reported to be between 0.69 and 2.35 per 1000 births (Andra et al., 1988). Repair of the alveolar cleft by creating continuity of the alveolar process comprises more than the treatment of a local bony defect only (Bajaj et al., 2003). It helps restore dental arch continuity, stabilizes the maxilla complex, and provides support to soft and cartilaginous tissue structures such as the alar base and upper lip (Schnitt et al., 2004; Van Aalst et al., 2005). The current gold standard for repair of the alveolar cleft is autologous bone graft harvested either from the iliac crest or from the mandibular symphysis (Koole et al., 1989; Koole, 1994; Enemark et al., 2001; Mikoya et al., 2010). Both grafting procedures carry potential risks for donor site morbidity, such as postoperative pain, hypersensitivity, pelvic instability, meralgia paresthetica, lateral femoral cutaneous nerve injury, infection, paraesthesia, apical root damage, and visible cutaneous scarring (Damien and Parsons, 1991; Hoppenreijs et al., 1992; Canady et al., 1993; Beirne et al., 1996; Booij et al., 2005; Swan and Goodacre, 2006; Weibull et al., 2009; Myeroff and Archdeacon, 2011). To prevent donor site morbidity, as well as to shorten surgery time, a synthetic bone substitute could be used to close the alveolar cleft. An in vivo study in a goat model has shown that grafting created alveolar clefts with pure-phase beta-tricalcium phosphate (β-TCP) provides similar bone healing to grafting with iliac crest bone (De Ruiter et al., 2010). In addition, when β-TCP was used in this model, orthodontic tooth movement proved to be similar. Although the exact mechanism of osteogenesis stimulated by β-TCP is still not completely understood, the aforementioned study justifies clinical evaluation in the human alveolar cleft situation. The aim of this pilot study (n = 7) was to generally evaluate the repair of the alveolar cleft after grafting with microstructured β-TCP.
Materials and Methods
Patients
Permission to carry out this study was granted by the Medical Ethics Committee, University Medical Centre, Utrecht, the Netherlands, protocol No. 09-129.
Seven patients, all with unilateral alveolar cleft were randomly included for alveolar cleft repair with β-TCP in 2010 and 2011. The male-female ratio was 5:2, and the mean age of the patients was 11.16 years (SD, ±1.83 years). The timing of the surgical procedure was on orthodontic indication (i.e., the point at which formation of two-thirds of the root of the tooth [canine or lateral incisor] bound to erupt into the repaired graft was visible on radiograph). In all patients, the alveolar cleft was repaired with micro-structured β-TCP grafting.
Surgical Procedure
Alveolar cleft repair was performed under general anesthesia with nasoendotracheal intubation. Antibiotic prophylaxis was given intravenously for 3 days (clindamycin, Hameln Pharmaceuticals, Hameln, Germany; 10 mg/kg per 24 hours). The surgical technique as described by Koole in 1994 and used until now was carried out. All patients had oronasal communication. The alveolar cleft region was exposed by means of a marginal incision and a releasing incision in the buccal sulcus. After the nasal lining was prepared and closed, the alveolar cleft was filled with β-TCP mixed with autologous blood (Figs. 1 and 2). No membranes were used.
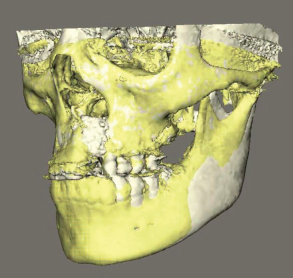
Micro-structured β-TCP granules inserted for repair of the alveolar cleft (CBCT scan).
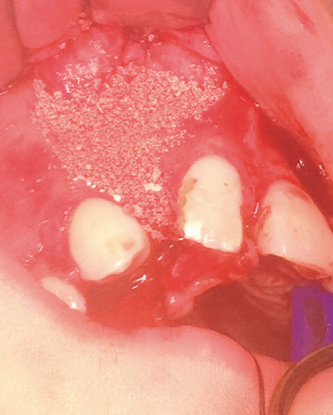
Micro-structured β-TCP granules inserted preoperatively for repair of the alveolar cleft.
The palatal mucosa was then sutured, and a vestibular mucoperiosteal layer was constructed with transpositional mucoperiosteal flaps. All sutures used were resorbable (Vicryl 4.0, Ethicon, Brussels, Belgium).
Orthodontic Procedure
Three months postoperatively, orthodontic therapy was started without actively engaging erupting teeth adjacent to the cleft. No orthodontic opening of the cleft gap was carried out.
Bone Substitute
The micro-structured β-TCP used in this study is a 65% ± 15% porous and >90% pure phase β-TCP graft material (X-Pand Biotechnology BV, Bilthoven, the Netherlands). It is synthetic, osteoconductive, osteoinductive, and resorbable (Yuan et al., 2010).
Radiographic Assessment
In the study group, a cone beam computed tomography (CBCT) scan was carried out directly preoperatively, 1 week postoperatively, and after 6 months. Radiation hazards restrained us from using conventional CT scanning. Parallel to this new radiographic protocol, conventional postoperative radiology by means of orthopantomography, occlusal radiography, and lateral cephalometry was also carried out. The CBCT scan analysis was performed by two independent investigators using an Osirix Dicom Viewer (Apple Inc.; Kim et al., 2012). Each investigator performed the analysis three times. Axial images were processed by demarcating the alveolar cleft using a free-form tool. The measured cleft region was assessed in the coronal plane from the lowest part of the nonaffected piriform aperture to the most caudal interdental alveolar bone level of the two proximal teeth in the large cleft segment. Thereafter, a three-dimensional model was calculated. The volume of the preexisting bone defect was compared in percentages with the total graft volume and with the residual bone volume 6 months postoperatively. We also looked at the vertical eruption of adjacent teeth into the bone substitute graft from the transversal images of the scans.
Statistical Analysis
Repeated-measures analysis of variance (SPSS 15.0, SPSS, Chicago, IL) was used to determine the influence of the within-subject factors moment of measurement, examiner, and repetition. Subsequently, contrasts were determined to study the levels of the within-subject factors. P < .05 was considered significant.
Results
Bone Volume
The 6-month postoperative examinations showed progressive alveolar bone union in all but one patient, in whom there was total graft loss. We excluded this case from further analysis, as shown in Tables 1 and 2. Eruption of the adjacent canine or lateral incisor into the repaired cleft occurred spontaneously in all patients.
Cleft Volumes Preoperatively, Postoperatively, and 6 Months After Operation*
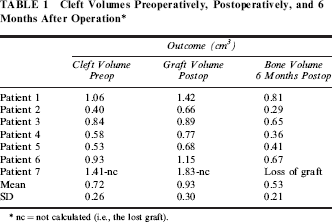
nc = not calculated (i.e., the lost graft).
Percentages of Cleft Volumes Preoperatively, Postoperatively, and 6 Months After Operation*
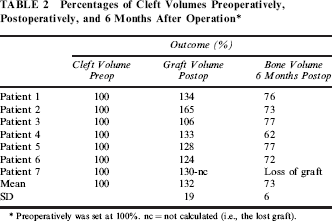
Preoperatively was set at 100%. nc = not calculated (i.e., the lost graft).
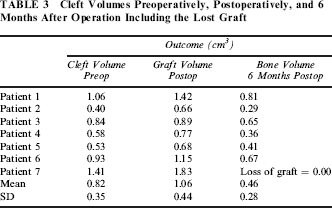
The outcome of the volume of the original clefts prior to surgery including the case with total graft loss is depicted in Tables 3 and 4.
Cleft Volumes Preoperatively, Postoperatively, and 6 Months After Operation Including the Lost Graft
Percentages of Cleft Volumes Preoperatively, Postoperatively, and 6 Months After Operation Including the Lost Graft*
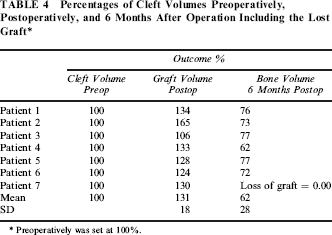
Preoperatively was set at 100%.
Statistical Analysis
Examiners did not have a significant influence on the determination of the bone volume (P = .58). Also, repetition of the determination did not significantly influence the outcomes (P = .21). The moment of the measurement, however, significantly influenced the bone volume outcomes (P < .001).
In Tables 1 and 2, a significant increase in bone volume was observed directly after operation (P < .005). The volume increased from on average 0.72 cm3 to 0.93 cm3, an increase of 32%. A significant decrease in volume occurred in the following 6-month period, from 0.93 cm3 to 0.53 cm3 (P < .001). The bone volume after 6 months was significantly lower than the initial value, 73% (P < .001). The results are depicted in Tables 3 and 4 with the data including the lost graft case.
Discussion
Six months after the operative grafting of microstructured β-TCP into the alveolar cleft, the bone volume thus acquired was satisfactory.
This leads to the assumption that the bone formation in the alveolar cleft after grafting it with micro-structured β-TCP was successful. We pixel-counted and compared the outcome as volumetric percentages, bearing in mind that the number of patients (n = 7) characterizes this study as a pilot study.
“As low as reasonably achievable” (ALARA) is an accepted principle in medicine and dentistry that dictates that health care professionals should use the smallest amount of radiation required to produce the information needed to diagnose and treat the patient (Reiner, 2009). Conventional medical CT scanning of a maxilla subjects the patient to 200 to 300 times the amount of radiation required for a panoramic radiography. Cone beam scanners use a narrow, collimated cone beam of radiation that can scan the maxilla only. This requires only 2 to 8 times the amount of radiation used in a panoramic radiograph. Compared with the two-dimensional data delivered by panoramic radiographs, the three-dimensional data generated by a CBCT provide outstanding information about alveolar cleft repair, thereby justifying its higher radiation load.
Overfill repair of the alveolar cleft with micro-structured β-TCP showed a mean fill percentage of 131.5% with regard to the original cleft. The percentages of acquired new bone volume with regard to the original cleft showed a mean percentage of 73%. This means a considerable resorption has occurred as also occurs when grafting the cleft with autologous bone. In general, these findings are corroborated in the literature (Rosenstein et al., 1997; Van der Meij et al., 2001; Schultze-Mosgau et al., 2003; Dickinson et al., 2008; Forte et al., 2012; Nagashima et al., 2013).
Repairing an alveolar cleft does obviously not mean that the alveolar process needs to be completely restored. Restoration of only 73% of the original cleft size bone volume apparently satisfies the functional load-bearing requirements of the roots of the teeth in terms of width and height of the alveolar process.
On the issue of filling the alveolar cleft defect, it is paramount to first assess which part of the defect needs to be filled with bone to obtain a successful result. The cranial part of the cleft site, which does not contribute to the facilitation of tooth eruption, is in most cases a bony site that is not subject to functional loading. The primary reason for this is the lack of paranasal musculature due to the cleft deformity. Resorption rates will therefore presumably be higher in the cranial part of the graft.
Overfilling the alveolar cleft defect is a method that most surgeons, whether using autologous or synthetic grafts, are inclined to. In an overfilled defect, there is a great deal of graft material that is not functionally loaded. When calculating the resorption rates of overfilled defects with regard to the original cleft volume, higher resorption rates will be found than when calculating resorption rates in nonoverfilled defects.
In one patient in this pilot study, there was total loss of the graft. The reason for this was surgery related and could not be attributed to the β-TCP scaffold. In this patient, a lateral incisor had erupted through the palatal side of the alveolar cleft defect, which made water-tight closure of the mucosa of the defect virtually impossible and may have caused salivary contamination of the granules. We therefore excluded this case from further analysis in Tables 1 and 2. These tables depict the more realistic outcome of the actual effect of grafting with β-TCP.
The authors heavily stress the importance of water-tight closure of the mucoperiosteal flaps when using β-TCP granules. It is even more important than when using bone blocks or spongious bone, since granules may leak from the restored cleft site, as was the case in this patient. Currently, the application of a putty-like micro-structured β-TCP is investigated in order to get around the problem of leaking graft material.
The spontaneous eruption that was scored for all six patients was considered as proof of the presence of bone. Histological data could not be provided since in the Netherlands, taking biopsies in humans for research purposes is strictly forbidden. But in a previous study, we were able to take a biopsy from the area of the chin from which bone had been harvested and then filled with the micro-structured calcium phosphate more than 18 months previously (De Ruiter et al., 2013). The biopsy was taken during a necessary reentry and with strict permission from patient and parents. This mandibular symphysis bone biopsy material was then prepared for histology, and the presence of almost complete bone formation is indisputably shown (Fig. 3).
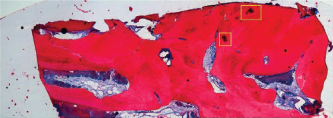
An overview of the entire biopsy at 40× magnification. The yellow squares indicate remnants of the implanted micro-structured calcium phosphate material. The open structure in between the bone is filled with bone marrow.
Conclusions
Worldwide, congenital facial clefts are considered to be a burden (Gundlach and Maus, 2006). To date, repair of the alveolar process in patients with cleft of lip, alveolus, and palate means the harvesting of autologous bone with its associated donor site morbidity. Previous experimental and clinical studies and the initial findings of this pilot study now elucidate a path toward the clinical use of microstructured β-TCP bone substitute for repair of the alveolar cleft.
Because of the considerable amount of bone resorption after overfilling the alveolar cleft, only recontouring the alveolar process with graft material will be sufficient for the bone volume needed for the functional loading of the bone by the teeth present.