
Abstract
Velopharyngeal dysfunction (VPD) can be secondary to anatomic, neurologic, or functional maldevelopment in the pediatric population. We present a case of transient VPD after the removal of a voluminous oropharyngeal hairy polyp in a newborn with an intact palate. This report sensitizes physicians, speech-language pathologists, and occupational therapists not only to the repercussions of oropharyngeal congenital masses, such as hairy polyps, on the feeding mechanisms of a newborn but also to the possibility of conservative management.
Keywords
Introduction
The pharynx is an important region when discussing otolaryngology in pediatrics. It is the most common area for surgery in this population, as well as a key player in resonance and valve functions in speech (Milczuk, 2012) and deglutition. Lesions in this region can lead to velopharyngeal dysfunction (VPD), and thus, physicians need to be aware of the components of the velopharynx, namely, the five paired muscles of the soft palate, the superior constrictor, and the adenoid pad (Milczuk, 2012), when performing procedures in this area. Velopharyngeal dysfunction after adenoidectomy is a well-known complication (Milczuk, 2012), with reports of cases posttonsillectomy (Wachtel et al., 2000).
We report a case of transient postoperative VPD occurring after the excision of a voluminous hairy polyp originating from the tonsillar fossa. Pharyngeal hairy polyps are rare benign congenital masses that can be asymptomatic or may cause intermittent to acute airway obstruction. Possible sites of origin include the nasopharynx, oropharynx, tongue, external auditory canal, and middle ear (Budenz et al., 2005; Cone et al., 2012; Yilmaz et al., 2012). In the oropharynx, hairy polyps originating from the tonsillar fossa, namely, the palatopharyngeus, have been reported (Christianson et al., 2013). The main purpose of this article is not to describe the hairy polyp but rather to report the rare diagnosis of VPD after excision of an oropharyngeal mass in a neonate and its conservative management.
Case Report
A term female neonate, with normal prenatal ultrasounds, was found to be in respiratory distress with cyanotic features at delivery. While performing oral suction, a large red mass was found in the patient's oral cavity. With persistent desaturations, an oral intubation was attempted without success secondary to the large obstructing mass. Manipulation of the lesion caused moderate bleeding and significant enlargement of the mass. Because of failure of direct laryngoscopy and intubation, the otolaryngology team was called emergently. On examination, a large hemorrhagic obstructing mass was filling the oral cavity, preventing visualization of the oropharynx on direct laryngoscopy. Through nasal flexible endoscopy, the patient was intubated. Magnetic resonance imaging (MRI) demonstrated an exophytic heterogeneous well-circumscribed tubular structure involving the oral cavity and oropharynx, without infiltration of the tongue but causing elevation of the soft palate (Fig. 1).
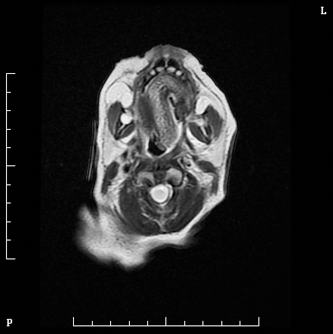
Magnetic resonance T1-weighted axial image demonstrating a circumscribed tubular structure involving the oral cavity. The mass has increased signal intensity peripherally and hypointense signal intensity in the center.
The patient was brought to the operating room for a thorough examination. Intraoperatively, a soft cylindrical 5.1 × 1.5 × 1.5-cm mass, pedicled in the left mid-tonsillar fossa, was found and removed in one piece (Figs. 2 and 3). Examination of the hard and soft palate demonstrated an intact palate with an asymmetrical left posterior tonsillar pillar compared with the contralateral side. Histopathological examination revealed a firm, dark, congested, and elongated ovoid mass partially covered by membranous and mucosal tissue. On sectioning, the mass appeared to be a blood-filled vascular structure. The final diagnosis was of a hairy polyp with ischemic changes.

Hemorrhagic pedunculated hairy polyp protruding from the oral cavity.

Postexcision view of the left tonsillar fossa. The location of the attachment of the mass can be seen.
Postoperatively, the patient presented with feeding issues with nasal regurgitation and difficulty obtaining a good seal while breastfeeding. The endoscopic evaluation of the velopharyngeal mechanism by the treating otolaryngologist revealed poor sucking and asymmetry of the velar length and ovements, which was thought to be the etiology of the VPD. The patient was referred to the occupational therapist (OT), who suggested a temporary nasogastric tube to help manage the patient's poor feeding. A videofluoroscopy revealed evident nasal regurgitation during feeds due to incomplete closure of the velopharynx, which proved our initial theory (Fig. 4).
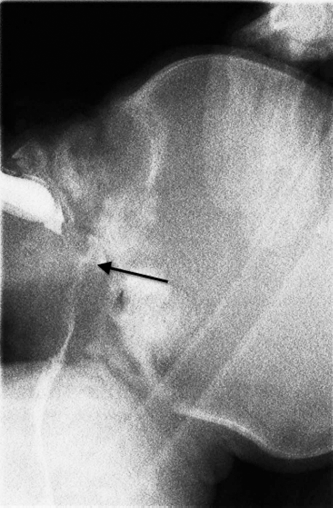
Video fluoroscopy demonstrates nasopharyngeal reflux (arrow) secondary to incomplete velopharyngeal closure.
Finally, we elected to manage the patient conservatively with a compressible bottle, similar to the ones used for patients with a cleft palate, despite the fact that the patient's palate was intact. At 1 month postoperatively, there was already improvement in the VPD. At 3 months, the symptoms had improved tremendously with rare regurgitation. At 6 months, the symptoms had completely resolved.
Discussion
Hairy polyps are uncommon masses with an incidence of 1 in 40,000 live births and a female-to-male ratio of 6:1 (Budenz et al., 2005; Cone et al., 2012; Yilmaz et al., 2012). Most cases originate from the lateral nasopharyngeal wall or superior surface of the soft palate (Budenz et al., 2005; Cone et al., 2012) and therefore are at risk of causing VPD. Cases of neonatal hairy polyp originating from the oropharynx have been described, including cases originating from the palatopharyngeus (Kelly et al., 1996; Karagama et al., 2003; Shvidler et al., 2007; Christianson et al., 2013). The presenting symptoms depend on the polyp's size and location and most commonly include feeding difficulties and respiratory distress; however, other symptoms such as stridor, cyanosis, hemoptysis, unilateral Eustachian tube dysfunction, and unilateral rhinorrhea may also occur (Shvidler et al., 2007; Yilmaz et al., 2012). Associated anomalies have been described and include congenital atresia of the left carotid artery, ankyloglossia, clefts of the soft and hard palate, and absence of the uvula and auricles (McShane et al., 1989).
Hairy polyp most likely falls into the category of a choriostoma, a benign mass consisting of normal tissue in an abnormal anatomical position (Budenz et al., 2005). Hairy polyps are usually described as gray to white or pink fleshy pedunculated masses. Interestingly, our case was found to be a blood-filled vascular structure histologically, and the final diagnosis was a hemorrhagic hairy polyp. In newborns and young children, other lesions must be considered such as meningocele, encephalocele, glioma, craniopharyngioma, and Rathke's cyst (McShane et al., 1989). Imaging modalities of choice for hairy polyps are computed tomography and magnetic resonance imaging. Both can demonstrate the fat containing polyp and distinguish it from a cyst or lesion of vascular or neurogenic origin as well as rule out intracranial or intraspinal connection (Kochanski et al., 1990; Budenz et al., 2005). The treatment of choice is surgical excision at the base of the stalk with histopathologic evaluation of the specimen (Cone et al., 2012).
There are many etiologies of VPD after procedures of the oropharynx. Some have suggested that VPD posttonsillectomy can occur secondary to injury to the motor nerves in the region, namely, the glossopharyngeal nerve (Garnett and Ramadan, 1996; Wachtel et al., 2000) that innervates the oropharyngeal and hypopharyngeal musculature. In fact, it is known that the velar muscles, apart from the tensor muscle, are innervated by the glossopharyngeal nerve and the pharyngeal plexus of the vagus nerve (Haapanen et al., 1994). Authors have reported glossopharyngeal nerve praxia following injury to the peritonsillar musculature or electrocoagulation of bleeding vessels in the tonsillar fossae (Haapanen et al., 1994). The incidence of paresis of the glossopharyngeal nerve has been reported to occur in 0.1% of tonsillectomies (Haapanen et al., 1994).
Furthermore, some have suggested that tethering of the soft palate from tonsillar pillars can lead to VPD (Shprintzen et al., 1987; Wachtel et al., 2000), possibly from retracted pillars secondary to large tonsils or posttonsillectomy due to scarred pillars pulling the velum down (Abdel-Aziz, 2012). However, as the VPD was transient in our case and the pillars did not appear to be scarred on examination, this etiology is unlikely.
There are reports of an association between oropharyngeal lesions and cleft palates due to the inability of midline fusion of the palate secondary to the bulk of the mass (Olivares-Pakzad et al., 1995). This could lead to VPD from a submucosal cleft palate or an occult submucosal cleft palate. However, our patient had an intact palate, which misled our OT to suggest a nasogastric tube to feed the patient. The latter highlights an important aspect of this report, in which physicians, OTs, and speech-language pathologists (SLPs) should be suspicious of VPD in patients who have an oropharyngeal mass resected despite a normal-appearing palate, in order to recognize and manage this entity early. In our case, the VPD was most likely secondary to the large empty volume of the nasopharynx left behind after excision of the polyp. On MRI, one can see that the space-occupying lesion caused the velopharyngeal musculature to be inhibited in its development, which created a large anteroposterior velopharyngeal distance (Fig. 5). After the mass was removed, the child's musculature gained space to develop and velar function was improved, thus allowing compensation to occur. This explains why, after a few months, our patient had adequate velopharyngeal closure. The authors have previously reported that VPD can occur after transoral procedures secondary to rostral pharyngeal disruption from injuries to the palate, modifications to the posterior pharyngeal wall, and creation of a large dead space in the posterior pharynx (Tuite et al., 1996; Koo et al., 2010), the latter being the cause of VPD in our patient. Similar to our case, Koo et al. (2010) reported transient VPD after a retropharyngeal lymphangioma was excised transorally, improving with conservative management.
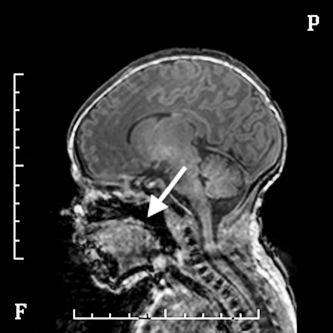
Magnetic resonance T1-weighted sagittal image demonstrating the large volume of the nasopharynx after excision of the polyp (arrow).
This case report has three main purposes. First, we demonstrated that VPD can occur secondary to an oropharyngeal mass without a concomitant cleft palate, and thus, physicians, SLPs, and OTs should be able to recognize the presence of VPD early in cases of postoperative feeding issues after excision of a neonatal oropharyngeal mass. The latter will avoid repetitive struggling of inadequate breastfeeding, early use of supplementary tools such as a compressible bottle, and more invasive feeding devices such as nasogastric tubes. Second, this report advocates for a conservative approach as an adequate first step in the management of this type of complication, as VPD can be transient and resolve spontaneously. Third, this report sensitizes physicians to the rare diagnosis of hairy polyp in the differential diagnosis of a neonatal oropharyngeal mass.
Conclusion
We present a unique case of a hemorrhagic polyp of the oropharynx in a neonate with transient VPD postexcision. This report sensitizes physicians, SLPs, and OTs to the potential of transient VPD postexcision of an oropharyngeal lesion in a neonate with an intact palate. It would be interesting to assess the feeding status of the previously reported cases of oropharyngeal hairy polyps, particularly of those originating from the tonsillar pillars, such as our case. This rare finding of VPD after oropharyngeal mass excision has led to us consider an interesting future project to examine the possible association between weak neonatal sucking mechanism and potentially unrecognized VPD.