
Abstract
Objective
To compare the maxillofacial morphology in the early mixed dentition phase between two patient groups with unilateral cleft lip, alveolus, and palate who underwent different types of palatoplasty.
Design
Cross-sectional study.
Setting
An institutional study.
Patients and Interventions
Seventy-one patients with unilateral cleft lip and palate (UCLP) treated at Osaka University Dental Hospital, Japan, were divided into two groups: 33 patients were treated by early two-stage palatoplasty by the modified Furlow Technique (ETS), and 38 patients were treated by one-stage Wardill-Kilner push-back palatoplasty (PB). Intergroup comparisons were performed.
Main Outcome Measures
The dental, skeletal, and soft-tissue features were evaluated. For intergroup comparisons, Mann-Whitney U test was used for the statistical analyses.
Result
No significant differences existed between the ETS and PB groups regarding the skeletal features except for the mandibular ridge height. Meanwhile, the upper central incisor and upper lip of the ETS group showed a more anterior position than those in the PB group.
Conclusions
Early two-stage Furlow palatoplasty leads to more protruded upper lip, providing more anteriorly positioned upper incisors compared with PB, at least at the early mixed dentition stage.
Keywords
There have been conflicting results of comparisons between dentofacial growth after one-stage and two-stage palatal repairs for patients with complete unilateral cleft lip and palate (UCLP) (Molsted et al., 1992; Friede et al., 1999; Corbo et al., 2005; Stein et al., 2007). These controversial findings likely derive from the differences in surgical protocols among institutions (e.g., the timing of and techniques used for soft/hard palate closures) and methodology (e.g., the validities of sampling, measurement and, analyses) (Yang and Liao, 2010).
At our institution, the early two-stage Furlow method (ETS; Nishio et al., 2001) was adopted in 1998. During ETS, the soft palate was closed by a Furlow double-opposing Z-plasty (Furlow, 1986) at 12 months of age, and the hard palate was closed by a Veau method at 18 months of age. Compared with the previous two-stage methods, it is considered that the earlier hard palate closure may reduce the impairment of the maxillary growth and allow earlier skill acquisition in terms of the speech articulation. In fact, a significantly longer anteroposterior palatal length and a better crossbite score were observed in 4-year-old patients treated by ETS than those who were treated by push-back palatoplasty (PB) performed at 12 months (Kitagawa et al., 2004; Nishio et al., 2010; Yamanishi et al., 2009, 2011). However, there have been no comparisons between the dentofacial morphology after the beginning of upper permanent incisor eruptions for groups of patients who underwent ETS and PB.
Previous reports demonstrated that PB methods lead to large denuded bone regions on the hard palate (Ross, 1987; Friede et al., 1993; Semb and Shaw, 1998); ignorance of the possible effects of inherent growth patterns prompted us to ask whether the ETS and PB approaches lead to different postoperative outcomes in terms of the convexity or concavity of the midface.
To orthodontically correct a maxillary deformity, the potential for maxillary growth must be considered. There are various views about growth modification of the maxilla during the primary and early mixed dentition period (Takada et al., 1993; Deguchi et al., 1999). It has been reported that the skeletal and dentoalveolar changes due to a maxillary protractor in subjects with deciduous dentition were significantly greater than those in subjects with mixed dentition (Kajiyama et al., 2004). Currently, no data are available to clarify the necessity for orthodontic growth modification to the patient with UCLP who underwent different types of palatoplasty in the early mixed dentition stage. Moreover, it remains unknown how orthodontic and orthopedic intervention should be optimized, and whether the dentofacial morphology of children who developed after the ETS and PB differs.
Accordingly, the purpose of this study was to evaluate the skeletal, dental, and soft tissue features of the patients with complete UCLP treated by ETS/PB and to compare them at the early mixed dentition stage. The findings of this study will contribute to decision-making regarding the orthodontic intervention during this period for the patients with complete UCLP.
Patients and Methods
Patients
The test group consisted of 71 patients with complete UCLP who had been consecutively referred from the Department of Oral and Maxillofacial Surgery to the Department of Orthodontics and Dentofacial Orthopedics, Osaka University Dental Hospital. They were divided into two groups: a PB group (27 male and 11 female patients; mean age, 7 years 2 months; treated by one-stage Wardill-Kilner push-back palatoplasty (Wardill, 1937) between 12 and 18 months of age) and an ETS group (21 male and 12 female patients; mean age, 7 years 4 months; treated by early two-stage Furlow palatoplasty, which consists of soft palate closure at 12 months of age, with modified Furlow's palatoplasty and hard palate closure at 18 months of age) (Nishio et al., 2001). To eliminate a technical bias, all palatoplasties were performed by the same senior surgeon at Osaka University Dental Hospital First Department of Oral and Maxillofacial Surgery, Osaka, Japan. All patients had no medical history and no previous history of orthodontic treatment. The study was approved by an ethics committee.
Measurements
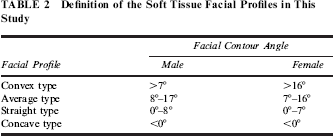
The lateral cephalometric radiographs were taken 1 month before the orthodontic treatment started. All cephalometric radiographs were traced and measured by one examiner. Each cephalometric radiograph was measured twice, and the mean value was used for the analyses. To assess intraexaminer errors, 20 randomly selected cephalometric radiographs were measured twice at an interval of 2 weeks. Intraexaminer errors were assessed using a paired t test. The cephalometric landmarks and angular and linear measurement parameters are shown in Table 1 and Figure 1. In addition, we measured the facial contour angle (Burstone, 1958), which was contained between lines drawn from the glabella (G) to subnasale (Sn) and a line connecting the soft pogonion (Pogs) and Sn, to classify the types of facial profile and calculate the proportion of each type (Table 2).
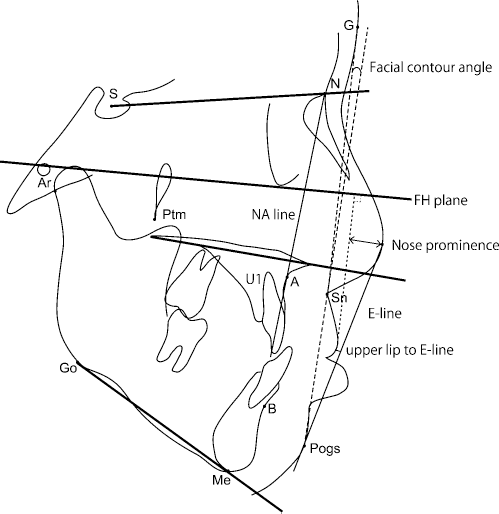
Reference points on the cephalometric radiographs.
Definitions of the Variables Used in This Study

Definition of the Soft Tissue Facial Profiles in This Study
Data Analysis
Initially, a null hypothesis that each variable had a normal distribution was tested by a chi-square test, whereas the homogeneity of variance for each variable was examined by a Levene test. Consequently, the characteristics of the dental, skeletal, and facial profiles at the initial stage of orthodontic treatment were statistically compared between the ETS group and the PB group by Mann-Whitney U test. In addition, we compared the proportion of each type of anterior occlusion and facial profile between the ETS and PB groups. The statistical analysis was performed using a statistical analysis software program (SPSS v17.0, SPSS Inc., Chicago, IL). The significance of mean differences was set at the .05 level. Additionally, the relative risk (95%CI) was calculated.
Results
To evaluate the reproducibility, the intraexaminer error was calculated. There was no significant intraexaminer error (P > .05). The results of intergroup comparisons of the skeletal and dental characteristics and soft tissue facial profiles at the initial visit to the orthodontics department are shown in Table 3. There were no significant differences in the angular or linear measurements of the skeletal features between the ETS group and the PB group, except for the Ar-Go linear distance. The ETS group showed a significantly greater Ar-Go distance than the PB group (P = .035; 95% CI, -3.87, -0.10). The distance of the upper incisors to the NA line was significantly smaller in the ETS group than in the PB group (P = .041; 95% CI, -3.48, -0.22). A significant difference (P = .006; 95% CI, -2.56, –0.43) in the distance of the upper lip to the E-line between the ETS group and PB group was observed. Except for overjet, measurement values of the two patient groups were within normative values (Wada, 1977).
Results of Comparisons Between the Early Two-Stage Furlow Method (ETS) Group and the Push-Back Palatoplasty (PB) Group at the Initial Visit to the Orthodontics Clinic
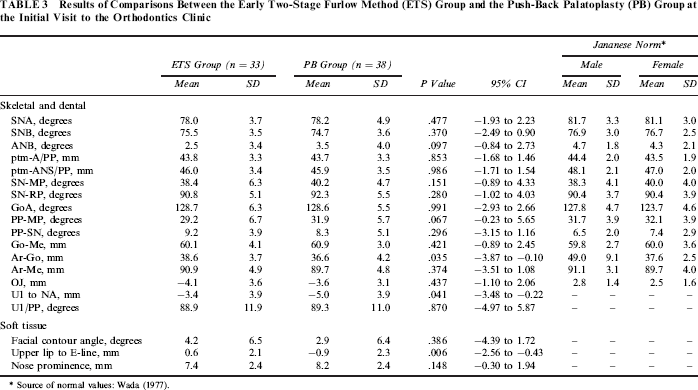
Source of normal values: Wada (1977).
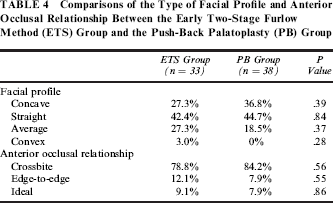
There were no significant differences in the proportions of each type of facial profile and anterior occlusal relationship between the ETS and PB groups (Table 4). Figure 2 shows a schematic diagram of the facial and dental features of patients in each subject group.

A schematic diagram of the facial and dental features of each patient group.
Comparisons of the Type of Facial Profile and Anterior Occlusal Relationship Between the Early Two-Stage Furlow Method (ETS) Group and the Push-Back Palatoplasty (PB) Group
Discussion
Previous comparisons between 4-year-old children who underwent the ETS and PB (Yamanishi et al., 2009, 2011; Nishio et al., 2010) reported that ETS provided a longer anteroposterior length of the maxilla and a better anterior occlusal relationship compared with those in patients treated by PB. With regard to the maxillary growth in the anteroposterior dimension, the present finding that there were no significant differences between the ETS and the PB groups suggests that efficient maxillary catch-up growth occurs in the PB group from 4 to 7 years of age, which is independent of gender. In addition, based on the findings of a similar distribution of the pattern of anterior occlusal relationship and facial profile for the two patient groups (Table 4) and no significant differences in the SNB angle and length of the Go-Me between the ETS and the PB groups, it can be concluded that the growth potential of the craniofacial skeleton for the ETS and PB groups was equally normal during the period of eruption of the upper central incisors.
The result of present analyses of the facial profiles of the soft tissue revealed a more posterior position of the upper lip in the PB group compared with the ETS group. These findings are associated with the significantly more anterior position of the erupted tooth crown of the upper central incisor with reference to the anterior border of the maxilla (U1 to NA) for the ETS group compared with the PB group (Table 3; Fig. 2).
Based on these findings, in addition to the lack of a significant difference in the nasal prominence between the ETS and PB groups, the facial profiles were closely related to their upper and lower dentoalveolar relationship in the incisor region.
Accordingly, the current results suggest that early two-stage Furlow palatoplasty provides a more protruded upper lip by leading to more anteriorly positioned upper incisors than does push-back palatoplasty at the early mixed dentition stage.
From 12 months to 4 years of age, it has been demonstrated that the increase in the upper arch length after palatoplasty for the ETS group is greater than that for the PB group (Yamanishi et al., 2009). Moreover, the increase was more than that for healthy controls (Yamanishi et al., 2009). Considering the remarkable decline of the anterior growth rate of the maxilla after 4 years of age in subjects with/without CLP (Mapes et al., 1974; Chen et al., 2010), the current findings suggest that the PB group had excellent maxillary growth potential that allowed the patients to catch up to the normative value during the period from 4 to 7 years of age. Accordingly, the finding of a posterior position of the upper incisors (U1 to NA) for the PB group might have resulted from impaired anterior development of the alveolar region before/during the eruption of permanent upper central incisors.
There is a thin gingival fibromucosa covering the alveolar process and surrounding the necks of the teeth (Markus et al., 1993). The presence of scar tissue in this part of the palate appears to be detrimental to the growth of the dental arch, in contrast to scars closer to the midline (Friede, 2007). Thus, different involvement of maxillary structures during surgery might account for variations in the growth outcome in cleft cases. Based on this information, it seems likely that the timing of the cleft palate repair is not the major cause of facial growth interference; instead, the push-back method itself may cause the deformity (Palmer et al., 1969; Rohrich et al., 2000). While PB is technically easier and gives good immediate results, there may be considerable scarring (Markus et al., 1993), which may be detrimental to the normal development of the maxillary dental arch in the incisor region.
Finally, the limitations of this study were the relatively small size of participants sampled from a local population by a single institution. Additional studies by an interinstitutional corporation are crucial to address those issues.
Conclusions
This study compared the dentoskeletal and soft tissue morphology of patients with complete UCLP treated by early two-stage palatoplasty and patients treated by push-back palatoplasty. The results indicated that the early two-stage Furlow palatoplasty allowed patients to obtain a more protruded upper lip with a more forward anterior position of the upper central incisors than the push-back palatoplasty did at the early mixed dentition stage. In addition, there were no significant differences in the maxillary growth between the ETS and PB groups, and their mean values were within normal range. Future studies will be directed toward investigating the outcome of orthodontic treatment after the early mixed dentition stage in patients with complete UCLP after different types of palatoplasty.