
Abstract
Objective
This study uses the American College of Surgeons Pediatric National Surgical Quality Improvement Program (ACS NSQIP Pediatric), a multicenter database, to identify risk factors for complications after cleft palate repair.
Design
Patients undergoing Current Procedural Terminology (CPT) codes 42200 and 42205 were extracted from the 2012 ACS NSQIP Pediatric. Patients older than 36 months or those who had undergone an additional surgery that altered the risk were excluded. Outcome variables were combined to create a complication variable. Fisher's exact, Pearson chi-square, and Wilcoxon rank-sum tests were used for analysis.
Results
Eligibility criteria were met by 751 patients. Of these, 192 (25.6%) had unilateral clefts, 146 (19.4%) bilateral, and 413 (55.0%) were unspecified. The average age at time of surgery for those without and with complications was 421.1 ± 184.8 and 433.6 ± 168.0 days, respectively (P = .76). Of the 21 (2.8%) patients with complications, respiratory complications were the most common. Risk factors associated with complications included American Society of Anesthesiologists classification of 3 (P = .003), nutritional support (P = .013), esophageal/gastric/intestinal disease (P = .016), oxygen support (P = .003), structural pulmonary/airway abnormality (P = .011), and impaired cognitive status (P = .009). Patients undergoing concurrent laryngoscopy (P = .048) or other surgeries (P = .047) were also found to be associated with increased complications. The 30-day fistula rate was 0.5%, and the readmission rate was 1.9%.
Conclusion
Perioperative complications for primary palatoplasty were 2.8% according to the ACS NSQIP Pediatric. Preoperative patient-related factors as well as concurrent surgeries may affect 30-day complication rates. These results help target those at greater risk for complications and allow for appropriate interventions to mitigate risks.
The goal of cleft palate (CP) repair is to aid normal feeding and speech development by repairing the muscular and palatal defect, while minimizing any potential impact on facial growth from disruption of the surrounding structures. Mortality rates with CP repair are very low, 0.01%, and complication rates range from 3% to 38% (Fillies et al., 2007; Desalu et al., 2010; Nguyen et al., 2014). Perioperative complications include dehiscence, bleeding, failed or difficult intubation, hypoxia, laryngospasm, bronchospasm, and reintubation (Lees and Pigott, 1992; Eaton et al., 1994; Desalu et al., 2010; Jackson et al., 2013). Respiratory complications are among the most common perioperative events, with published rates between 5.7% and 38% (Antony and Sloan, 2002; Desalu et al., 2010; Jackson et al., 2013; Kulkami et al., 2013), compared with the 7.4% to 15% associated with other pediatric operations (Bordet et al., 2002; von Ungem-Sternberg et al., 2010).
Although current studies based at single institutions offer insights into potential risk factors for complications, no study has made use of a national cohort to describe these complications. In addition, there is little agreement on what items are collected or what constitutes major or minor complications. The American College of Surgeons Pediatric National Surgical Quality Improvement Project (ACS NSQIP Pediatric) database is a national cohort of perioperative risk factors and 30-day morbidity and mortality outcomes. The ACS NSQIP Pediatric offers a unique platform to study 30-day outcomes in procedures with relatively low incidences and is particularly suited to improving the process of care in high-risk patients through evidence-based practice measures. We aimed to use the ACS NSQIP Pediatric to determine the incidence of postoperative complications after CP repair and the associated risk factors to improve perioperative care in these patients.
Materials and Methods
The ACS NSQIP Pediatric is a Health Insurance Portability and Accountability Act compliant data set and therefore exempt from institutional review board review. Information on the 129 variables collected can be found on the ACS NSQIP Pediatric website (http://www.pediatric.acsnsqip.org/). This is the first year the database has been made available and included data from January 1, 2011, to December 31, 2011. The database is maintained by an ACS-trained surgical clinical reviewer, and the data are entered into a database maintained by Outcome Sciences, Inc., a Quintiles company located in Durham, North Carolina. Cases were selected from operative logs of more than 50 hospitals and abstracted for review using an 8-day cycle based on surgical service. Exclusion criteria included age 18 years or older; re-operations; a Current Procedural Terminology (CPT) code different from that of the Principal Operative Procedure; cases with CPT codes not on the inclusion list; or a trauma, transplant, or concurrent case. Hospitals with a 30-day follow-up rate of 80% or greater and an interrater reliability audit (IRR audit) disagreement of 5% or less were included. Case files are regularly audited by the IRR audit, and overall disagreement is approximately 2% (American College of Surgeons 2013).
According to the operations manual given to the surgical clinical reviewer, the 10 International Classification of Diseases, 9th edition (ICD-9) codes describing congenital malformations were collected according to a Provided Collect List (version date: July 1, 2013). Often the cleft diagnosis was included as a congenital malformation, and this created an artificially raised percentage of congenital malformations. To better standardize data regarding congenital malformations, the congenital malformation variable was recoded, per the Provided Collect List, to exclude ICD-9 codes related to the cleft diagnosis and codes not included in the protocol.
Patients older than 1096 days (36 months) or who had undergone an additional surgery that altered the risk, such as other pharyngeal procedures, were excluded. Additional surgeries were categorized by similar CPT codes. Several variables, including birth height and weight, were also excluded from analysis due to lack of data. Surgical-site infections (superficial incisional, deep incisional, and organ/space), wound disruption, pneumonia, unplanned intubation, pulmonary embolism, mechanical ventilation >12 hours after surgery (including continuous positive airway pressure [CPAP] and bilevel positive airway pressure [BiPAP], called prolonged ventilation), progressive renal insufficiency, acute renal failure, urinary tract infection, coma, seizure, cerebrovascular accident, nerve injury, intraventricular hemorrhage, cardiac arrest, bleeding/transfusion, graft/prosthesis/flap failure, venous thrombosis, sepsis, central line–associated blood stream infection, death, and reoperation were combined to create a complication variable. An additional adverse airway event variable was created for using unplanned intubation or mechanical ventilation >12 hours after surgery (including CPAP or BiPAP). Fisher's exact, Pearson chi-square, and Wilcoxon rank-sum tests were used for analysis on Stata software, version 13 (College Station, Texas). A P value <.05 was considered statistically significant.
Results
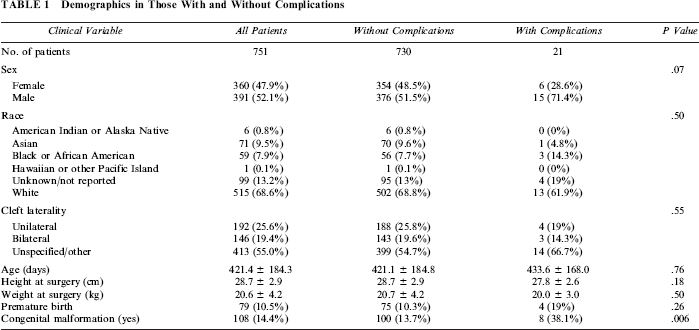
Of the 1004 patients identified with CPT codes 42200 and 42205, 751 met eligibility criteria. Demographic data are shown in Table 1. There were 192 (25.6%) unilateral clefts, 146 (19.4%) bilateral clefts, and 413 (55.0%) unspecified. Furthermore, 108 (14.4%) patients had an additional congenital malformation. The most common comorbidities were cardiac (15.4%), impaired cognitive status (15.3%), and esophageal/gastric/intestinal disease (13.6%) (Tables 2 and 3). The average operative time was 136.2 ± 69.9 minutes and 149.2 ± 77.1 minutes for those with and without complications, respectively (P = .40). The most common concurrent procedures performed were ear, nose, and throat (ENT) procedures (57.3%) (Table 4). The average age of surgery for those without and with complications was 421.1 ± 184.8 days and 433.6 ± 168.0 days, respectively (P = .76) (Table 5).
Demographics in Those With and Without Complications
General Preoperative Risk Factors

Cardiopulmonary and Neurologic Preoperative Risk Factors

Concurrent Surgeries Performed During Palatal Repair

Operative Details, Length of Stay, and Readmissions
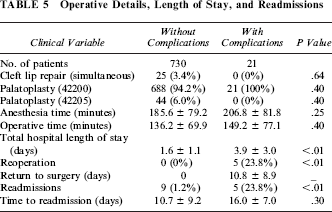
Of the 21 (2.8%) patients with complications (Table 6), respiratory complications were the most common, including seven mechanical ventilations for >12 hours after surgery, four unplanned reintubations, and one case of pneumonia. Other complications consisted of four wound dehiscences, five total reoperations (three for unknown reasons), and two graft/prosthesis/flap failures with one patient having an additional surgical site infection. The four wound dehiscences indicate disruption of the palatal mucosa and translate into palatal fistulas as advised from the ACS NSQIP Pediatric Operations Manuel (version date: January 1, 2014). The readmission rate was 1.9%.
Complications Details
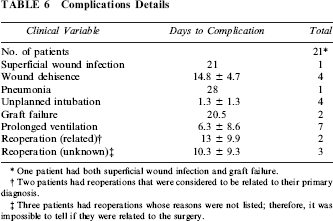
One patient had both superficial wound infection and graft failure.
Two patients had reoperations that were considered to be related to their primary diagnosis.
Three patients had reoperations whose reasons were not listed; therefore, it was impossible to tell if they were related to the surgery.
Risk factors (Tables 2 and 3) associated with complications included congenital malformation (P = .006), American Society of Anesthesiologists (ASA) physical status classification of 3 (P = .003), nutritional support (P = .013), esophageal/gastric/intestinal disease (P = .016), preoperative oxygen support (P = .003), structural pulmonary/airway abnormality (P = .011), and impaired cognitive status (P = .009). Patients undergoing additional surgeries (Table 4), such as laryngoscopy (P = .048) or other surgeries (P = .047), were also found to be associated with increased complications. Of note, cardiac risk factors were not found to be significant. Age was then examined, and patients with cardiac risk factors were found to be about 18 days older than other patients (437.9 ± 158.4 versus 419 ± 187.6; P = .013).
When adverse airway events were examined, congenital malformations (P = .002), ventilator dependency (P = .043), oxygen support (P ≤ .001), esophageal/gastric/intestinal disease (P = .050), impaired cognitive status (P = .003), neuromuscular disease (P = .045), nutritional support (P ≤ .001), ASA classification of 3 (P = .001), and ENT procedure (P = .012) were found to be significantly associated with risk of complications. Patients with respiratory complications had an increased length of stay compared with those with other complications (1.6 ± 1.1 versus 5.5 ± 3.2 days, P ≤ .001) (Table 7).
Risk Factors for Adverse Airway Events

This is reported as mean ± standard deviation, whereas the rest of the data are shown as counts (percentages).
Discussion
Overall, complication and readmission rates for CP repairs were low, at 2.8% and 1.9%, respectively. Adverse airway/pulmonary events, not including pneumonia, occurred with the greatest frequency. Other issues in patients with complications are wound related in 28.6% and need for reoperation in 23.8%. Airway complications prolonged hospital stays by 3.9 days on average; by comparison, the average increase across all complications was 2.3 days. This is especially important given that the cost of inpatient stay increases $7,663 per day, according to charge data (Owusu et al., 2012). Congenital malformation, ASA classification of 3, nutritional support, esophageal/gastric/intestinal disease, oxygen support, structural pulmonary/airway abnormality, impaired cognitive status, and a concurrent surgery of laryngoscopy or “other” were associated with increased overall complications. When examined separately, adverse airway events were associated with congenital malformation, ventilator dependence, oxygen support, esophageal/gastric/intestinal disease, impaired cognitive status, neuromuscular disease, nutritional support, ASA classification of 3, and ENT procedure. By identifying modifiable risk factors, evidence-based protocols can be developed to improve the quality of cleft care and decrease adverse events.
Previous single-institution studies examining adverse airway events in CP repair have found associations with preoperative obstructive sleep apnea (OSA), congenital abnormalities, syndromes, jaw or tracheal anomalies, history of difficult airway, operative time, and surgeon and anesthesiologist (Antony and Sloan, 2002; Jackson et al., 2013; Smith et al., 2013). Anesthesiologist experience and pediatric-specific training have been found to be associated with better outcomes across pediatric specialties. In Mamie et al. (2004) study, patients not under the care of a pediatric anesthesiologist had a 1.7 times increased risk for perioperative respiratory adverse events. When these factors were compared with those from the ACS NSQIP Pediatric, OSA could be a marker for ventilator dependence, given that ventilator dependence includes those on CPAP and BiPAP, both treatments for OSA. Surgeons and anesthesiologists are becoming increasingly aware of OSA as a risk factor for adverse airway events, and in populations undergoing adenotonsillectomy, adverse airway events have been linked to data collected by polysomnogram studies and OSA questionnaires (Jaryszak etal., 2011; Tait et al., 2013).
The risk factors of ventilator dependence, oxygen support, and greater ASA classification to surgery make intuitive sense when thinking of respiratory complications. Not surprisingly, tracheostomy, which bypasses the palate as a potential site for airway obstruction, has not been found to be associated with adverse airway events in this study or the study of Jackson et al (2013). ASA classification has been associated with duration of postoperative ventilation and postoperative complications (Wolters et al., 1996).
Esophageal/gastric/intestinal disease may be considered a marker of gastroesophageal reflux disease (GERD). The ACS NSQIP Pediatric includes patients taking medication for GERD in esophageal/gastric/intestinal disease, and because the condition is common, it is likely that many of the patients have GERD, though this would be impossible to verify. GERD has been associated with complications and adverse airway events in patients younger than 3 year undergoing adenotonsillectomy (McCormick et al., 2011). In addition, ENT procedures also have a history of increasing risk of airway complications (Mamie et al., 2004).
Impaired cognitive status, neuromuscular disease, and nutritional support are newly reported perioperative risk factors for palatoplasty. Of note, although learning disabilities have been linked to multiple exposures to anesthesia before the age of two (Flick et al., 2011), no studies have associated impaired cognitive status to operative morbidity in children. Reasons for this association may be that these patients include those with a higher preoperative disease burden, and that interaction would not be accounted for in a univariate analysis. It could be that children with cognitive disabilities may have more difficulty protecting their airway. The same could be true for those with neuromuscular disease and those who require nutritional support.
Of note, cardiac risk factors were not significant. Cardiac anomalies have been associated with postoperative complications, and in other studies it has been suggested that CP repair is delayed in those with cardiac conditions (Ramamoorthy et al., 2010; Harry et al., 2013). In our cohort, surgery in patients with a cardiac diagnosis was delayed by 18 days on average, and this difference in age was statistically significant. Further study is needed to understand the complex interaction of cardiopulmonary disease and palatoplasty risk.
While institution-based risk factors are intuitive and should be considered, the retrospective nature of those studies is both beneficial—in that very detailed data can be collected on patients—and troublesome—in that collection points are biased toward hypothesized risk factors and a less general examination of the patient. In addition, risk factors are difficult to compare across studies, especially when population sizes are small, as in most cleft studies. Not all studies collect the same risk factors the same way. The largest institution-based study of CP perioperative airway events contains only 300 patients (Jackson et al., 2013). The ACS NSQIP Pediatric collects more generalized and comparable data across many institutions and, even in its first year, has a much larger population (n = 751). Because of the continued morbidity of adverse airway events across multiple specialties, ACS NSQIP Pediatric should consider additional data oriented toward preventing these events, such as perioperative respiratory complications, OSA status, and separation of GERD from other gastrointestinal anomalies. Despite this, the ACS NSQIP Pediatric is a new database that shows promise in helping to address these clinical concerns.
Thus far the risk factors identified by the ACS NSQIP Pediatric seem to differ from previous studies on surgical risk factors, although this is only the first year to be made available to users. This current study is limited in the use of univariate analysis because of the large number of risk factors available and the still relatively small data set (Voorhis and Morgan, 2007). Examining this broader univariate, analysis is useful in determining how more targeted studies using the ACS NSQIP Pediatric may be approached. Future studies can benefit from the way the ACS NSQIP Pediatric approaches defining risk factors and complications as well as determining what deficiencies the ACS NSQIP Pediatric currently contains in order to better advocate for changes within the data collection that better reflect the CP population. In addition, our study is limited in the way congenital malformations are collected, a significant lack of granularity.
The ACS NSQIP Pediatric has several inherent limitations in that it collects general information on surgical risk factors and outcomes and does not include information on surgical technique, preventive measures taken for perioperative risk, geographic region, or long-term functional outcomes. Because it is a central, offsite database, it is not possible to gain additional information on patients who are included in a given study; as relates to our study, more than 50% of patients' clefts were unspecified, making risk stratification based on cleft type difficult. Only 30-day complications are tracked and long-term data are not available. Hospitals choose to participate in the program; therefore, there may be a bias in the hospitals included. Data on birth history and laboratory data are not often collected and were not included in the analysis of this study. Despite these limitations, the ACS NSQIP Pediatric offers the possibility of exploring risk factors in a large national cohort of patients with CP and can be used to improve processes of care, patient and parent counseling, and overall outcomes. It also offers clear and comparable patient risk factors and outcomes for future research.
Conclusion
Overall, complication and readmission rates for CP repair are low, but adverse airway events continue to cause morbidity and prolonged hospital stays. Risk factors identified using the ACS NSQIP Pediatric differ from those identified in earlier studies and require more detailed research to understand their contribution to surgical risk. These results help target those at greatest risk for complications and allow for appropriate interventions to mitigate risks.