
Abstract
Objective
The transverse maxillary deficiency frequently observed in patients with cleft lip and palate (CLP) is usually treated by rapid maxillary expansion (RME). Considering that RME causes a significant increase of the internal nasal dimensions in children with unilateral CLP (UCLP), this study aimed to characterize the internal nasal geometry of children with bilateral CLP (BCLP) and transverse maxillary deficiency using acoustic rhinometry. The study also aimed to analyze changes caused by RME.
Design
Cross-sectional prospective study.
Setting
Laboratory of Physiology, Hospital for Rehabilitation of Craniofacial Anomalies, University of São Paulo, Bauru, SP, Brazil.
Participants
Fifteen children with repaired BCLP of both genders, aged 8 to 15 years, referred for RME, were prospectively analyzed.
Interventions
Subjects underwent acoustic rhinometry before the expander installation and after the active phase of expansion. Cross-sectional areas (CSA) and volumes (V) of the nasal valve regions (CSA1 and V1) and turbinates (CSA2, CSA3, and V2), were measured after nasal decongestion.
Main Outcome Measures
In the majority of the subjects, an increase of internal nasal dimensions was observed.
Results
Percent changes of CSA1, CSA2, CSA3, V1, and V2 were: +25%, +11%, +9%, 20%, and +12%, respectively. Differences were significant for all variables studied, except CSA3 (P < .05).
Conclusions
RME promotes an increase in the internal nasal dimensions of children with BCLP, suggesting that RME is capable of substantially improving nasal patency in this population.
Cleft lip and palate (CLP) is often associated with nasal deformities such as septal deviation, nostril atresia, and turbinate hypertrophy (Wetmore, 1992; Trindade et al., 2009). In bilateral clefts, the most evident alterations are a very short, or even absent, columella, and a flattened and enlarged nasal tip. These deformities frequently reduce the nasal cavity dimensions and nasal patency, leading to oral breathing (Wetmore, 1992; Fukushiro and Trindade, 2005), which in turn may impair craniofacial development (Linder-Aronson, 1979). On the other hand, the impairment of maxillary growth, commonly observed in individuals with cleft palate, often leads to nasomaxillary retraction associated with anterior crossbite and unilateral or bilateral posterior crossbite. In these cases, treatment often involves orthopedic procedures such as rapid maxillary expansion (RME).
Radiographic studies after RME have shown transverse movement of the nasal lateral walls and consequent pulling away of nasal turbinates in relation to the nasal septum. This observation led authors such as Haas (1965) and Wertz (1970) to suggest that improvements on nasal breathing were a beneficial effect of RME.
Different techniques have been used to assess the impact of RME on nasal geometry, such as radiographic imaging and, more recently, cone-beam computed tomography (Ribeiro et al., 2012; Smith et al., 2012), rhinomanometry (Hershey et al., 1976; Langer et al., 2011), and acoustic rhinometry (Ceroni Compadretti et al., 2006; Trindade et al., 2010). Acoustic rhinometry, specifically, allows consecutive measurements of different segments of the nasal cavity from the nostrils to the nasopharynx. Thus, it is possible to accurately identify the location of constrictions that contribute to nasal resistance. Moreover, this method is fast and noninvasive, provides topographic information of the nasal cavity, and does not require the active participation of the patient (Hilberg, 2002; Trindade et al., 2009).
Previously, our research demonstrated that RME caused a significant increase of the internal nasal dimensions, as assessed by acoustic rhinometry, in the majority of children with complete unilateral CLP (UCLP) (Trindade et al., 2010). Considering that subjects with bilateral CLP (BCLP) present with more severe maxillary transverse deficiencies due to the width of the cleft, the involvement of both sides of the face, and the more affected nasal conditions in adulthood (Fukushiro and Trindade, 2005), it was prudent to investigate the effects of RME in this population as well.
The present study aimed to characterize the internal nasal dimensions of children with repaired complete BCLP and transverse maxillary deficiency, and to analyze, prospectively, the changes caused by RME on the nasal cavity. For this purpose, the nasal cross-sectional areas and volumes of the regions corresponding to the nasal valve and the nasal turbinates were analyzed by means of acoustic rhinometry.
Materials and Methods
Institutional Review Board and Parent/Patient Consent
This study was approved by the local institutional review board (protocol 386/2010-SVAPEPE-CEP). Parents were initially informed about the procedures involved in the study, then invited to have their child participate and sign an informed consent form.
Study Population
All subjects included in this study were treated regularly at a Quaternary Craniofacial Hospital during a period of 12 months. Subjects met the following criteria: bilateral complete cleft lip and palate, primary plastic surgeries performed in early childhood, regular orthodontic treatment, and referred for RME during mixed dentition. Patients with syndromes or other obvious craniofacial anomalies and/or allergic or respiratory symptoms that resulted in nasal congestion when examined were excluded from this study. Table 1 reports the demographic characteristics of the study population.
Demographic Characteristics of the Study Population, Regarding Age, Race, Gender, and Social Status
Criteria adopted by the Brazilian Institute of Geography and Statistics (IBGE) for race (Brazilian government).
Procedures Performed and Outcomes Examined
A Haas fixed expander with tooth-tissue borne anchors was used for correcting the transverse maxillary deficiency. In the case of insufficient palatal depth, a Hyrax expander device was used. The screws were activated twice per day, completing one turn, from 7 to 11 days depending on the severity of the transverse maxillary deficiency. Each complete turn of the expansion screw corresponded to an opening of approximately 0.8 mm. After the active expansion phase, the expander was kept in position for at least 3 months and replaced with a fixed appliance. All of the appliances were made at the in-house laboratory of the Hospital for Rehabilitation of Craniofacial Anomalies, University of Sao Paulo.
Rhinometry was performed using the same equipment following the same protocol used by Trindade et al. (2010), which evaluated the effect of RME on internal nasal dimensions of children with UCLP. An Eccovision Acoustic Rhinometer system (Hood Laboratories, Pembroke, MA) was used, consisting of a 24-cm tube with a loudspeaker positioned at the distal end and a recording microphone at the proximal end. This apparatus measured reflected sound waves that emerge from the nasal cavity in response to incident sound waves. The tube is placed against one of the nostrils and then a sound wave generated by the loudspeaker propagates through the tube and enters the nasal cavity. Any constrictions that reduce cavity diameter reflect the sound waves back into the tube. The pressure signals are sensed by a microphone, amplified, digitalized, and then analyzed by a computer with specific software. Nasal cross-sectional areas (CSA) were calculated from echo intensity. Distances were calculated based on the wave speed and the time for the echo to arrive. These data were converted into an area-distance function and displayed as a graph, rhinogram, on a monitor. The area under the curve was graphed using a semi-logarithmic scale for the y-axis (cm2) as a function of distances (cm) on the x-axis, as shown in Figure 1.
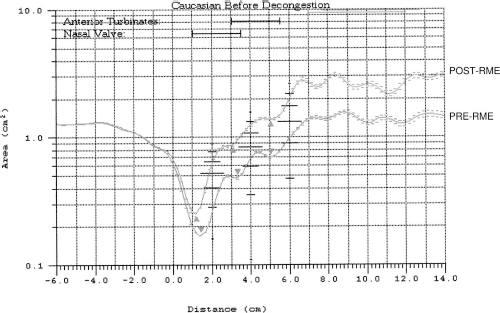
A patient's rhinograms obtained before (PRE-RME) and after (POST-RME) rapid maxillary expansion from the right nasal cavity after application of a nasal vasoconstrictor, illustrating the increase in cross-sectional areas.
Measurements were performed during voluntary interruption of nasal breathing at the end of an exhalation. After nasal decongestion, three measurements were taken for each nasal cavity, and the values were averaged together for analysis. In particular, nasal decongestion was achieved via topical application of 0.1% xylometazoline hydrochloride 10 minutes prior to the exam in an effort to minimize the interference of nasal mucosa with CSA and nasal volume (V) measurements and, thus, exclusively determine the effect of RME on the skeletal aspect of the nasal cavity. The nasal CSA was measured (cm2) in the second deflection of the rhinogram corresponding to the nasal valve (CSA1), the third deflection corresponded to the anterior end portion of the inferior nasal turbinate (CSA2), and the fourth deflection (CSA3) corresponded to the posterior portion of the inferior nasal turbinate (Corey, 2006). Nasal V was also determined by integrating the areas under the curve at the segments located between 10 mm and 32 mm in relation to the nostril (V1), which includes the nasal valve, and at the segment located between 33 mm and 64 mm, which includes the nasal turbinates (V2) (Antila et al., 1997). Individual changes in CSA and V produced by RME (increases or decreases) were considered significant when greater than 10% (Trindade et al., 2014).
Statistical Analysis
To assess if the sample of the present study came from a normally distributed population, the Shapiro-Wilk test was used. Considering that all variables, except CSA1 followed normal distribution, Student's t test for paired samples was used to analyze the statistical differences between pretreatment and posttreatment for CSA2, CSA3, V1, and V2; whereas, the Wilcoxon signed-rank test was used to assess the statistical differences between pretreatment and posttreatment for CSA1. Results were expressed as mean (±standard deviation). Values of P < .05 were considered significant.
Results
Twenty-six subjects underwent acoustic rhinometry immediately before the installation of the expansion device (PRE-RME). Of these 26 subjects, 15, aged 8 to 15 years, returned for RME and rhinometric follow-up exams 30 to 270 days after treatment (POST-RME). The remaining 11 patients dropped out of the study. More specifically, six did not return because they received orthodontic follow-ups away from the hospital, and the other five were excluded from the study because they did not adhere to the study protocol (i.e., the activation of the expander was not performed properly by the subjects). Moreover, all subjects had BCLP without any related craniofacial anomalies.
In order to characterize the effect of RME on the nasal cavity overall, values were presented as the sum of the right and left sides of the nasal cavity. Table 2 shows the cross-sectional mean areas and volumes assessed in the 15 subjects after decongestion, PRE- and POST-RME. Mean values (±SD) of CSA1, CSA2, and CSA3 PRE-RME were 0.89 (0.17), 2.18 (0.46), and 3.16 (0.72) cm2, respectively. POST-RME, mean values (±SD) increased to 1.11 (0.27), 2.43 (0.46), and 3.43 (0.85) cm2, respectively. Differences for both CSA1 and CSA2 PRE- and POST-RME were statistically significant. More specifically, the percentage increase between the mean PRE-RME and POST-RME values were +25%, +11 % and +9%, for CSA1, CSA2, and CSA3, respectively. Figure 1 shows PRE-RME and POST-RME rhinograms, illustrating the increases in the CSA1, CSA2, and CSA3, seen in one subject after RME.
Mean Nasal Cross-Sectional Areas (CSA1, CSA2, and CSA3)and Volumes (V1 and V2), of Children With Bilateral Complete Cleft Lip and Palate, Assessed by Acoustic Rhinometry After Nasal Decongestion, Before (PRE-RME) and After (POST-RME) Rapid Maxillary Expansion, and the Percentage Variation (Δ%)

P < .05.
Mean (±SD) values of V1 and V2 PRE-RME were 2.96 (0.58) and 8.82 (1.88) cm3, respectively. POST-RME, values increased to 3.55 (0.49) and 9.89 (1.89) cm3, respectively. Differences for both V1 and V2 PRE- and POST-RME were statistically significant. In particular, the percentage increase between mean PRE-RME and POST-RME values were +20% for V1 and +12% for V2.
Regarding individual changes of nasal CSA after RME, 73% and 47% of the subjects showed a significant increase in CSA1 and CSA2, respectively. The remaining subjects had no significant changes. For the CSA3, 47% of the subjects showed a significant increase, while 20% showed a significant decrease between PRE-RME and POST-RME. Regarding nasal volumes, 67% of the patients showed a significant increase in V1 after RME. No significant changes in V1 were observed for the remaining subjects. After RME, significant increase in V2 was observed in 47% of the patients, and in only one case was a significant reduction observed (6%).
Discussion
Considering that bilateral complete clefts are commonly associated with nasal and maxillary deformities and that a previous study (Trindade et al., 2010) had demonstrated that RME increases internal nasal dimensions in unilateral complete cleft lip and palate, the primary objective of this study was to characterize the internal nasal dimensions of children with BCLP. Additionally, the impact of RME on the nasal cavity of children was assessed.
The results showed that nasal cross-sectional areas and volumes of patients with BCLP are similar or slightly greater than in patients with unilateral complete clefts (Trindade et al., 2010). These findings are in agreement with those obtained by Warren et al. (1988), who reported that children with BCLP presented the “best nose”—the most patent nose as assessed by rhinomanometry. The columella lengthening, usually performed at this age range, may have contributed to this finding, considering that 10 of the 15 patients from the present study underwent columella surgery. Conversely, Fukushiro and Trindade (2005) observed that the nasal airway dimensions of adults with BCLP are smaller than that of subjects of the same age with unilateral cleft lip and palate. The authors attributed this difference to a growth deficit of the nose that occurs in bilateral cases as compared to unilateral cases.
Considering the classical view of Aduss and Pruzansky (1967) that “the roof of the mouth is the floor of the nose,” our initial hypothesis was that the orthopedic correction of the transverse maxillary deficiency would lead to a substantial improvement of nasal patency, estimated by internal nasal dimensions. The results of the present study indicated that RME was indeed capable of positively impacting the nasal airways by increasing nasal cross-sectional areas and volumes of patients with bilateral cleft lip and palate. Results also indicated that the mean CSA1, CSA2, CSA3, V1, and V2 increased by approximately 9% to 25%. The observed increases in CSA3 between PRE-RME and POST-RME were less than 10% and thus classified as not clinically significant. The other variables increased significantly after RME, displaying the impact of this procedure on the nasomaxillary complex.
When compared to changes in CSA and V in children with unilateral clefts (Trindade et al., 2010), proportionally greater changes in area and volume were observed following RME in children with bilateral clefts. Most likely, this finding is a result of greater maxillary atresia in children with bilateral clefts, which requires a greater degree of expansion. This finding suggests a reduction of the nasal resistance to airflow and, thus, a significant improvement in nasal breathing.
When analyzing individual data, it was observed that 73% of the subjects had increases in their CSA1 and 67% in their V1 after RME. Among children evaluated more than 3 months after RME (n = 6), where a stabilization of nasomaxillary structures or eventually a return of the nasal dimensions to their original values would be expected, four maintained a significant increase in CSA1, suggesting a satisfactory and lasting effect of RME on the nasal cavity. The two subjects who underwent RME at ages greater than 12 years also had a significant increase in their CSA1 and V1, supporting our notion that age did not interfere with the results. However, it should be confirmed with a larger sample size.
The most common method used to characterize nasal patency is rhinomanometry, which involves the simultaneous measurement of differential transnasal pressure and nasal airflow during nasal breathing when quiescent. Based on the ratio between these variables of pressure and flow, rhinomanometry allows one to calculate nasal resistance. Alternatively, it is possible to calculate the minimum cross-sectional nasal area, which has the advantage of being a flux-independent measurement. In this respect, values obtained will be the same during any respiratory flow, unlike nasal resistance, which vary depending on the patient's breathing effort (Warren and Drake, 1993).
Authors like Enoki et al. (2006) and Halicioğlu et al. (2010) demonstrated, by means of rhinomanometry, that the transversal increase in the upper dental arch promoted by RME results in a significant decrease in nasal resistance in a considerable number of patients without cleft lip and palate. On the other hand, Langer et al. (2011) verified that RME does not permanently decrease nasal resistance. Additionally, rhinomanometry requires the collaboration of the patient and does not indicate the location of the constrictions of the nasal cavity. Conversely, acoustic rhinometry allows consecutive measurements on different segments of the nasal cavity from the nostrils to the choanae, and thus the location of the constrictions that contributed to the nasal resistance can be accurately identified in a quick and noninvasive manner without the need for active participation of patients, providing topographic information about the nasal cavity (Hilberg, 2002; Trindade et al., 2014).
The rhinomanometry findings previously mentioned were corroborated by others who used acoustic rhinometry to assess nasal patency. For example, both Bicakci et al. (2005) and Ceroni Compadretti et al. (2006) found significant variations in nasal resistance and/or in nasal cross-sectional area after RME. Sökücü et al. (2010) also observed significant increase in internal nasal volume after expansion.
Cone-beam computed tomography is another method widely used to assess internal nasal dimensions. For instance, Smith et al. (2012) conducted a retrospective study of 20 adolescents using CT scans to measure changes in nasal volume after RME and found significant increases in these nasal volumes 3 months after treatment when compared to the volume before RME. However, this method to assess internal nasal dimensions involves the emission of high doses of ionizing radiation to the patient and, consequently, follow-up exams become unfeasible due to uncontrolled systemic risks inherent with the use of x-rays. In contrast, acoustic rhinometry does not expose patients to radiation, yet it allows an evaluation of nasal areas and volumes as accurate as CT scans allow, without the risk to the patient. Furthermore, acoustic rhinometry is easy, painless, and noninvasive.
Finally, the data obtained in the present study can be universally applied to patients from other rehabilitation centers. In other words, the rapid maxillary expansion procedure is capable of substantially increasing the upper airway of subjects with cleft lip and palate, especially in bilateral cases, regardless of the primary rehabilitation protocol used.
The results found in this study based on acoustic rhinometry showed that children with complete bilateral cleft lip and palate have equivalent or slightly larger internal nasal dimensions than children with unilateral cleft lip and palate. Furthermore, RME positively impacts nasal geometry, and thus nasal patency which is known to impair children with clefts.
Footnotes
Acknowledgments
The authors thank Coordination for the Improvement of Higher Education Personnel (CAPES), Brasilia-DF, Brazil, and São Paulo Research Foundation, São Paulo-SP, Brazil, for their financial support.