
Abstract
Objective
To identify an additional objective measure to aid in the evaluation of children with isolated metopic craniosynostosis.
Design
This is a retrospective study comparing specific computed tomography scan measurements between surgical and nonsurgical cohorts of children with isolated metopic craniosynostosis. Children were included if they were diagnosed with isolated metopic craniosynostosis and ultimately underwent computed tomography scan imaging as part of their evaluation. The subjects were placed in the surgical or nonsurgical cohorts on the basis of the final treatment recommendation after they completed a full multidisciplinary, multimodality evaluation. Comparisons were made with a control group of unaffected patients from our institutional trauma registry.
Setting
Tertiary academic institution.
Patients, Participants
The subjects are patients who had been previously evaluated in our clinic for isolated metopic craniosynostosis and received a computed tomography scan as part of their workup.
Results
The average intercoronal distances were significantly different among all three groups (P ≤ .002). The average cephalic width-intercoronal distance ratio for children who received a recommendation for surgery differed significantly from that of both the observation cohort and the control group (P ≤ .001). However, the cephalic width-intercoronal distance ratio did not differ between the observation cohort and the control group (P = .927).
Conclusions
The cephalic width-intercoronal distance ratio may be an additional objective measurement to aid in the clinical evaluation of children with metopic craniosynostosis.
Craniosynostosis is the premature fusion of one or more cranial sutures. It is a relatively common craniofacial anomaly with a reported incidence of approximately 1 in 2000 live births (Cohen, 2000). The metopic suture is the first to undergo physiologic closure and can begin to close as early as 3 months of age (Vu et al., 2001). The metopic suture was previously thought to be the least commonly affected suture in craniosynostosis; however, multiple recent reports have documented a significant increase in the incidence of isolated metopic craniosynostosis (IMC) (Selber et al., 2008; Di Rocco et al., 2009; van der Meulen et al., 2009; Kweldam et al., 2011).
Isolated metopic craniosynostosis is classically associated with trigonocephalic dysmorphology. It is well documented, however, that the severity of cranial dysmorphology in children with IMC varies significantly (Posnick et al., 1994; Birgfeld et al., 2013). This spectrum of dysmorphology ranges from mild bitemporal narrowing with a metopic ridge to overt trigonocephaly. The evaluation of children who fall into the middle of this spectrum can be complex because the severity of dysmorphology does not appear to correlate with the severity of developmental delay, behavioral problems, or increased intracranial pressure (Martinez-Lage et al., 1999; Shimoji and Tomiyama, 2004; Mendonca et al., 2009; Starr et al., 2010; Eley et al., 2012). Therefore, it is possible that there are children with less severe dysmorphology who would benefit from surgical intervention.
The Craniosynostosis Working Group has recommended that all children with craniosynostosis be cared for by a multidisciplinary team (McCarthy et al., 2012). In addition, given the developmental and behavioral problems that have been described in children with IMC, we feel that the assessment of these children should be based on a multidisciplinary, multimodality evaluation and not solely on the surgeon's assessment of the dysmorphology. The multidisciplinary, multimodality evaluation performed at our institution is presented in Table 1. We do note, however, that the subjective evaluation of dysmorphology is important.
The University of Missouri Multidisciplinary, Multimodality Initial Evaluation for Patients With IMC
In this study we consider a number of additional quantitative measurements in an effort to identify an additional objectively defined characteristic to aid in the evaluation and formulation of treatment recommendations for these children with IMC. We set out to determine whether there are radiographic skull measurements that correlate with our clinical impression of children with IMC.
Methods
After obtaining institutional review board approval, we retrospectively reviewed the University of Missouri craniosynostosis database and identified all children who presented to our clinic with concerns for craniosynostosis between 2006 and 2012. Children were included in the study if they were diagnosed with IMC and ultimately underwent computed tomography (CT) scan imaging as part of their evaluation. A total of 119 children were included. Children were excluded if they had distorting, noncraniosynostosis anatomic anomalies; their imaging was inadequate to obtain accurate measurements; or their evaluation was incomplete and they did not receive a final treatment recommendation. A total of 15 children were excluded: seven for distorting, noncraniosynostosis anatomic anomalies, one for inadequate imaging, and seven for incomplete evaluations; therefore, 104 subjects were ultimately included in the study.
The 104 subjects were divided into two groups: those who received a recommendation for surgery (frontoorbital advancement and anterior calvarial vault remodeling; n = 52) and those who received a recommendation for close observation (n = 52). Recommendations were based on the multidisciplinary, multimodality evaluation described in the previous paragraph and in Table 1. Demographics of the surgical and observation cohorts are presented in Table 2.
Demographics of Surgical and Nonsurgical Cohorts

A control group of 35 children, aged 3 years or less (to reflect the age distribution of the patient samples) was populated with patients from the University of Missouri Trauma Registry who had previously undergone CT scans of the head for noncraniosynostosis indications. These children's CTs were performed on the same group of CT scanners and with the same standard positioning (the head in a neutral position with regard to rotation and the orbitomeatal line perpendicular to the CT table) as the subjects' CT scans.
The CT scans of all included subjects were reviewed, and five specific radiographic craniofacial measurements were performed (Table 3). All CT scans were evaluated using GE Centricity PACS imaging software (Version 4.0, Barrington, IL). Our measurement technique was based on the work of Waitzman and colleagues (1992a, 1992b). We took advantage of modern radiographic imaging software and slightly modified some of Waitzman and colleagues' techniques to obtain the most precise measurements possible. After determining the appropriate axial CT slice windowing the images for soft tissue, we then visualize that slice windowing the images for bone to make our measurements (Fig. 1). The anterior interorbital distance, lateral orbital distance, and intertemporal distance were measured on the CT slice that best transected the globe, optic nerve, medial rectus, and lateral rectus. The intercoronal distance and cephalic width measurements were made on the CT slice containing the anterolateral-most extent of the lateral ventricles. The cephalic width was measured as originally described: between the outer tables of the skull at the widest portion of the skull on the selected CT slice. However, we did not measure the intercoronal distance as described by Waitzman et al. (1992a). Instead, we measured it as the distance between the coronal sutures, which are readily visible on the images windowed for bone.
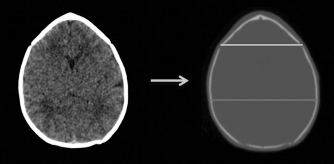
Our modification of Waitzman and colleagues' (15-16) measurement technique. Top line = intercoronal distance; bottom line: cephalic width.
Radiographic Skeletal Measurements

Modified from the original description by Waitzman and colleagues.
All CTs were obtained with the patient in a standardized position: the head in a neutral position with regard to rotation and the orbitomeatal line perpendicular to the CT table. This is a well-established position for CT scans of the head and was used by Waitzman and colleagues in their landmark craniofacial measurement articles (Waitzman et al., 1992a, 1992b). In addition, they found that with up to 8° of variance (4° in either direction) from neutral positioning, craniofacial measurements differ by less than 5% from those taken at 0° of head tilt (Waitzman et al., 1992a). Comparing those taken with 10° of tilt with measurements taken at a neutral position, their intercoronal distance measurements differed by 1.1 % and the mean difference of all measurements was 2.8%. At-10° of tilt, the intercoronal distance differed by 1.4% and all measurements differed by 3.9% (Waitzman et al., 1992a). We accepted these small degrees of variance.
The control group was statistically compared with all subjects with IMC using Student's t tests (P ≤ .05). In order to determine whether measures differed among the surgical cohort (IMC–S), observation (IMC–O) cohort, and the control group, a series of analyses of variance (ANOVAs) and Tukey post hoc analyses were performed.
Results
Initial data analysis showed that only cephalic width, intercoronal distance, and the CW-ICD ratio differed significantly among groups (Table 4). The average intercoronal distance was significantly larger in controls as compared with subjects (109.49 versus 99.93 mm; P ≤ .001), as was average cephalic width (130.83 versus 122.12 mm; P ≤ .001). In contrast, the mean CW-ICD ratio significantly increased in the subjects relative to the control group (1.22 versus 1.19; P = .004).
Comparison of Intercoronal Distance, Cephalic Width, and CW-ICD Ratio in IMC and Control Cohorts

CW-ICD = cephalic width-intercoronal distance; Group = group effect.
In comparing the control group individually with the surgical cohort and the observation cohort (Table 5), there was a significant group effect for all three measures (P ≤ .001 for all three). Average cephalic width was largest in the control group (130.83 mm), followed by the surgical cohort (122.27 mm) and then the observation cohort (121.98 mm). Post hoc tests of cephalic width show that both IMC cohorts differed significantly from the control group (P ≤ .001 for both), but the observation and surgical cohorts did not differ from each other (P = .985). Average intercoronal distance was greatest in the control group (109.49 mm), followed by the observation cohort (102.47 mm) and finally the surgical cohort (97.39 mm). Post hoc tests show that all three groups differed significantly from one another (control to observation ratio, P ≤ .001; control to surgical ratio, P ≤ .001; observation to surgical ratio, P = .002). The average CW-ICD ratio was greatest in the surgical cohort (1.25); whereas, the control group and observation cohort had similar average values (1.19 for both). Post hoc tests show that the surgical cohort differed significantly from both the observation cohort and the control group (P ≤ .001 in both cases), but the observation cohort did not differ from the control group (P = .927).
ANOVA and Tukey Post Hoc Analysis of the Control Group, Observation Cohort, and Surgical Cohort (Mean ± Standard Deviation) *

ANOVA = analysis of variance; CW-ICD = cephalic width-intercoronal distance; Group = group effect; C-O = comparison of the control group to the observation cohort; C-S = comparison of the control group to the surgical cohort; O-S = comparison of the observation cohort to the surgical cohort.
Discussion
Clinical decision making in patients who fall into the middle of the spectrum of dysmorphology associated with IMC can be highly complex. Ideally, a multidisciplinary, multimodality evaluation is used to inform the decision-making process. We retrospectively evaluated five cranial measurements to determine whether these measures accurately reflect the outcome of our comprehensive evaluation and decision-making process in our patients with IMC. Our aim was to identify additional pieces of objective data that may be used in concert with the data that are already obtained from the multidisciplinary assessment to help make treatment decisions for these patients.
Of the measurements we analyzed, the intercoronal distance and the CW-ICD ratio significantly distinguished the patients with IMC from the control group. When the patients recommended for surgery and those recommended for observation were analyzed separately, we found that the intercoronal distance is significantly different among all three groups, but it is the CW-ICD ratio that distinguishes the surgical cohort from both the observation cohort and the control group. Given that the CW-ICD ratio uniquely distinguishes our surgical cohort, we submit that in addition to other previously described radiographic findings in IMC, such as the endocranial notch and the endocranial bifrontal angle (Weinzweig et al., 2003; Beckett et al., 2012), the CW-ICD ratio can aid in the evaluation of children with IMC. These are quick, easy-to-perform, useful objective measurements. In this retrospective study, the differences in these measures reflect our clinical assessment based on a multidisciplinary, multimodality evaluation of patients to determine who would benefit from surgery and which patients should be observed.
The fact that the difference in CW-ICD ratio most significantly distinguishes the surgical cohort from both the observation and controls cohorts after initial analysis is not surprising. Beckett and colleagues (2012) have previously shown that the interdacryon and interzygomaticofrontal suture distances in children with moderate trigonocephaly are not significantly different from those in a control group. Given the similarity between the interdacryon and interzygomaticofrontal suture distances and the anterior interorbital and lateral orbital distances, which were used in our study, it is not surprising that the difference in these measurements between our operative and observation cohorts was not as significant as the difference we described in our measure. Beckett and colleagues (2012) found that the only significantly different measurement in their moderate trigonocephaly patients versus controls was the endocranial bifrontal angle (ECBFA). However, they did not perform cranial measurements similar to the CW and ICD (and we did not measure the ECBFA). Furthermore, viewing trigonocephaly macroscopically, we expected a larger difference to be observed in cranial vault measurements, rather than in those of the facial skeleton in our cohorts. Although facial skeletal dysmorphology is certainly a component of trigonocephaly, the cranial dysmorphology, particularly the bitemporal narrowing, is commonly more striking. With all of these factors in mind, it is not entirely surprising that the difference in the CW-ICD ratio between our two cohorts emerged as the most significant in our study. It is also important to note that whereas the CW-ICD ratio did not differ between the observation cohort and controls, this ratio is only a single measurement that does not describe the totality of dysmorphology and clinical presentation of the patients in the observation cohort.
There is overlap between our operative and observation cohorts with respect to the ranges of their CW-ICD ratios, and there are children with the same CW-ICD ratio who did not receive the same treatment recommendation (Fig. 2). We contend there are several key points that can be gleaned from these facts. First and foremost, the CW-ICD ratio is one piece of data and should not be used alone to develop a treatment recommendation for any given child; we submit that the same holds true for any single piece of data used to evaluate these patients. Second, this finding speaks to the broad spectrum of dysmorphology with which these children present as well as the broad spectrum of the overall clinical picture these children have. Furthermore, there are other dysmorphic features of the skull and orbits in children with metopic craniosynostosis that are not described by this ratio. It should also be noted that in their study of CT measurements, Beckett et al. (2012) found that the ECBFA was the only significantly different measurement, and there was overlap between the ECBFA of control patients and those of metopic synostosis patients (134° to 160° and 100° to 148°, respectively).
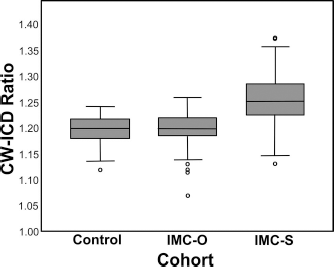
Box-and-whisker plots of CW-ICD ratio values by cohort.
After noting these overlaps, one may question the value of the CW-ICD ratio. There is no question that the CW-ICD ratio will be of little benefit in patients at either extreme of the dysmorphology spectrum. Where the ratio may be useful is in a child with intermediate dysmorphology. If that child is developing and behaving normally, does not have any ophthalmologic signs of increased ICP, has normal head growth, and does not have any other worrisome signs, then a ratio close to 1.19 would support clinical observation. Alternatively, a ratio close to 1.25 in a child with early closure of the anterior fontanelle, an endocranial notch on CT, some mild developmental delays noticed on formal neuropsychological testing, and behavioral abnormalities would support consideration of operative intervention. There will certainly be situations where the opposite is true (a ratio closer to that of the surgical group for a child in whom all other signs point toward observation and vice versa). In this scenario, it is important to remember that the ratio only evaluates the degree of frontal stenosis and does not evaluate all aspects of a child's dysmorphology. In brief, the CW-ICD ratio reflects a single data point that is meant to augment a larger, multidisciplinary, multimodality evaluation. We again emphasize that no measure should be used in isolation to make a treatment plan and that there will likely be instances where the other elements of a child's evaluation will outweigh the findings of calculating this ratio. This consideration would apply to other types of previously described measurements and CT findings as well, such as the endocranial notch and the ECBFA (Weinzweig et al., 2003; Beckett et al., 2012). These CT-based characteristics are not absolute indicators of the need for surgery, but they can serve to guide and inform clinical decision making in these patients (Weinzweig et al., 2003; Beckett et al., 2012).
It is also important to emphasize that this study is retrospective. The CW-ICD ratio was not evaluated to determine whether it can be used as a predictive tool. Rather, we sought to determine whether there is a correlation between the outcome of our multidisciplinary, multimodality evaluation and clinical decision-making process and this measurement. Although these treatment decisions are ultimately still clinical judgments, in our system these judgments are made by a multidisciplinary team using multiple types of data rather than a single surgeon imposing only his or her subjective impression of the patient. The CW-ICD ratio is another feature that can be added to the other data to create an overall profile for each patient that, taken as an integrated whole, can be used to inform clinical decision making.
This is not the first time that an increased CW-ICD ratio has been identified in children with IMC, although it has been known by slightly different names. In 1998, Bottero and colleagues (1998) in Paris retrospectively reviewed 76 children on whom they had operated for IMC. They used the CW-ICD ratio to assess the severity of frontal stenosis in their patient population and attempted to correlate this with developmental outcomes. They obtained their measurements using the measurement techniques originally described by Waitzman and colleagues (1992a, 1992b). The mean CW-ICD ratio in their operative patient population was 1.23.
As part of their work published in 2002, Shimoji and colleagues reviewed a series of CTs of 50 patients with what they defined as mild trigonocephaly who had been treated surgically. They used Waitzman and colleagues' (1992a, 1992b) measurement techniques as originally described. Their average ratio was 1.25 in their patient population and 1.21 in a normal population control group.
Neither of these studies evaluated the CW-ICD ratio as a potential component of the preoperative evaluation for a child with IMC. Due to the slight difference in measurement technique, our results cannot be directly compared with those of these previous authors. That said, our technique yields a ratio that is consistently slightly lower than that obtained by using Waitzman and colleagues' (1992a, 1992b) measurement methods. Therefore, the average ratio of our surgical cohort approximately equates to the moderate to severe range of the subjects in Bottero and colleagues' study (1998). It should be noted that they divided their subjects into cohorts based on the degree of developmental delay and learning disability and not severity of cranial dysmorphology; however, they report an overall mean CW-ICD ratio of 1.23 with means of 1.27 and 1.29 for their more severely delayed cohorts. Although, obviously, our subjects and theirs cannot be compared directly, we do note that our surgical groups appear to have similar degrees of frontal stenosis. We do not find value in comparing our results with those of Shimoji and colleagues (2002) because their indications for operative intervention were more liberal than ours, and we note that this difference in indications for operative intervention is likely to be a confounding variable in any comparison between the two groups.
Limitations of our study include its retrospective design and the fact that it is a single-center study. Because we do not perform routine serial CT scans of the nonoperative patients, it is unknown whether the ratio changes over time for these patients. With these limitations noted, we submit that the CW-ICD ratio is another useful objective measurement that can serve as a complement to other objective measurements and the subjective evaluation of cranial dysmorphology when evaluating a child with IMC and intermediate dysmorphology. The CW-ICD ratio is a single piece of data, and treatment decisions should not be based solely upon this ratio. Each child with IMC should be evaluated on a case-by-case basis with a complete multidisciplinary, multimodality evaluation. Further research is currently under way to assess the long-term neuropsychological outcomes of both the surgical and observation cohorts in our patient population.