
Abstract
Accurate and early diagnosis of benign fibroosseous lesions is important because the treatment and resulting outcomes of each differ. Juvenile ossifying fibromas typically occur in young patients and grow rapidly with a high recurrence rate. Their monostotic nature has previously differentiated these tumors from other fibroosseous lesions. We describe an interesting and extremely rare case of polyostotic juvenile ossifying fibromas in a 14-year-old boy with involvement of the maxilla and mandible. The available literature on juvenile ossifying fibromas is also briefly reviewed. When diagnosing a polyostotic fibroosseous lesion, it is important to not exclude the possibility of juvenile ossifying fibromas because this may warrant a different treatment.
The term benign fibroosseous lesions encompasses a spectrum of rare tumors, of which the most frequently discussed are fibrous dysplasia, adult ossifying fibroma (AOF), and most recently, juvenile ossifying fibroma (JOF). In the past, the rare nature of these tumors has made developing a standardized classification challenging. Inconsistent and competing nomenclatures has led to frequent misdiagnosis and mismanagement of JOF (Brannon and Fowler, 2001; Osunde et al., 2013).
It is important that JOFs are distinguished from other fibroosseous lesions because they each have a different disease progression. Patients with JOF typically present at a young age (under 15 years old), with rapid tumor growth from a single site (monostotic tumor). The recurrence rate tends to be high (30% to 58%), warranting early accurate diagnosis, surgical resection, and long-term follow-up (Abuzinada and Alyamani, 2010; Urs et al., 2013).
We present an exceptionally rare and interesting case of JOF in an adolescent. In reviewing the literature, this is the only reported case of JOF that is polyostotic.
Patient
A 14-year-old boy presented to an outside hospital with left maxillary and mandibular masses. Because these masses were thought to be fibrous dysplasia, he was initially managed with observation. Histologic analysis of these masses from a subsequent debulking procedure showed findings of ossifying fibroma. Several months later, the patient then presented to our practice at Loma Linda University Craniofacial Clinic (Fig. 1). By this time, both masses had grown in size. The maxillary mass involved the ipsilateral alveolus, zygoma, ethmoid sinuses, nasal bone, and bilateral palatine bones. On examination, superolateral displacement of the left orbit was noted from the mass effect. The mandibular mass involved the ipsilateral alveolus and angle of the mandible and partially involved the contralateral mandibular parasymphyseal region (Fig. 2).

A 14-year-old boy presenting with facial asymmetry from large left maxillary and mandibular masses. Left orbit is superolaterally displaced from the mass effect of the tumor. Left oral commissure and nasal base are displaced inferiorly.
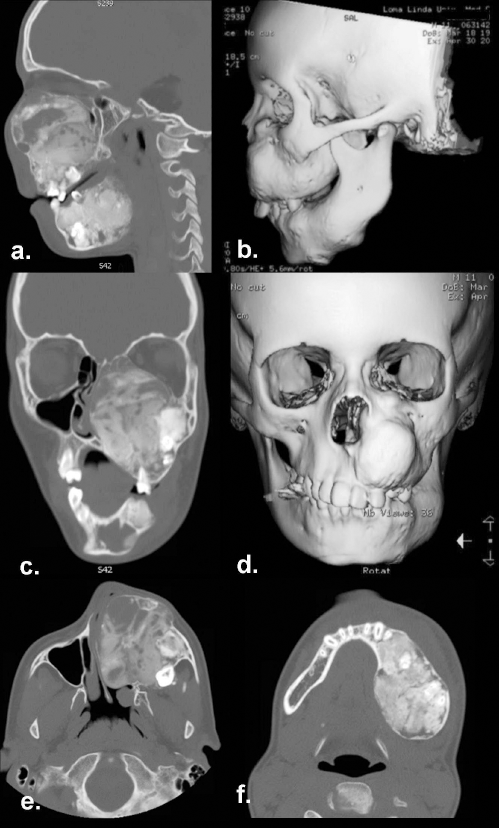
Computed tomographic images of polyostotic fibro-osseous tumors. a: Sagittal and b: lateral views of the left maxillary and mandibular tumors with involvement of teeth. c: Coronal and d: anteroposterior views demonstrating the superolateral displacement of the left orbit by the fibro-osseous lesion. Axial views demonstrating the extent and size of the e: maxillary and f: mandibular tumors.
The involved left hemimandible, left maxilla, left zygoma, left orbit, ethmoids, nasal bone, and bilateral palatine bones were surgically resected. Histologically, the specimens were fibroosseous lesions with ovoid eosinophilic cementumlike material (Fig. 3). This hypercellular lesion had narrow, thin trabeculae and was sharply demarcated from adjacent normal bone. Thinning and focal disruption of the cortical surfaces was also seen.
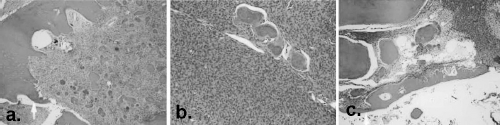
Histological findings of juvenile ossifying fibroma. a: Well-demarcated lesion can be seen where there is a clear, sharp edge of fibro-osseous process adjacent to normal unaffected mandibular bone. b: Hypercellularity with ovoid cementum-like material in the mandibular tumor. c: A focally hypercellular fibro-osseous lesion of the maxillary bone with thinning of the normal adjacent maxillary bone.
Once margins were confirmed histologically to be free of tumor, the maxillary defect was reconstructed with a combination of patient-specific implants (Synthes, Inc., West Chester, PA) and a right free fibula flap (Fig. 4). The mandibular defect was reconstructed with a patient-specific reconstruction plate (Synthes) and a left free fibula flap. The patient was discharged to home at 2 weeks once he had been fully ambulating and eating an oral diet. He is doing well and is being followed closely in the clinic (Fig. 5).
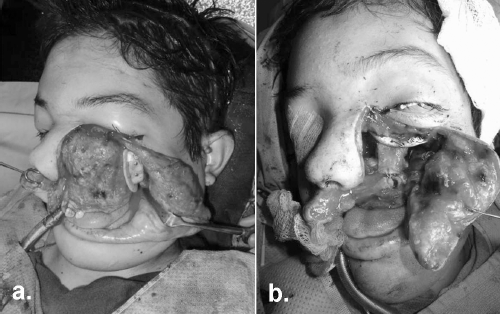
a: Weber-Ferguson incision pattern was used to expose the maxillary tumor and a portion of the mandibular tumor. b: The maxillary defect was reconstructed with a patient-specific implant (Synthes, Inc., West Chester, PA) and free fibula flap.
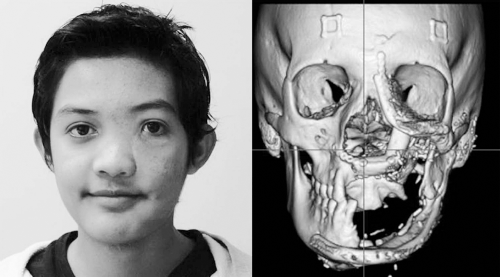
Left: Improvement in facial symmetry and correction of previous distortion are noted at 10 months postoperatively. Right: Excellent symmetry and well-integrated fibula osteocutaneous flaps are seen in the corresponding computed tomography image results at 10 months postoperatively.
Discussion
Ossifying fibromas are rare benign tumors that are well demarcated and tend to grow in a concentric, expansile pattern. They encompass AOF and JOF. Adult ossifying fibromas are thought to originate from periodontal ligament; whereas, JOF arise as a neoplastic myxoid tissue from cartilage and bone precursors (Urs et al., 2013). Two histologic subsets of JOF have been described: trabecular and psammomatoid (El-Mofty, 2002). Juvenile trabecular ossifying fibromas (JTOF) consist of slender trabeculae of immature bone that may form a lattice (Slootweg, 2012). These tumors contain cell-rich fibrous tissue and are lined by a rim of enlarged osteoblasts (Slootweg and El-Mofty, 2005). Juvenile psammomatoid ossifying fibromas (JPOF) are characterized by fibroblastic stroma with calcified psammomatoid bodies and spindle-shaped fibroblasts (Slootweg and El-Mofty, 2005; Sarode et al., 2011). Round and ovoid collections of bone with osteoid rim can also be seen in these lesions.
The patient described here has the only reported case of JOF that is polyostotic. A review of the literature found reports of 123 patients with JOF Table 1). Every case described a monostotic lesion with a near-equal predilection for the mandible (44.7% of cases) and the maxilla (42.3% of cases). Juvenile ossifying fibromas occurred less frequently in the ethmoid sinuses, frontal bone, orbit, and parietal bone. A majority of the patients were diagnosed in Europe (36.6%), a third in India (31.7%), and a smaller portion in North America (14.6%). Juvenile ossifying fibromas occurred in males slightly more frequently than in females (52% and 48%, respectively). Of the patients where the JOF subtype was described, JPOF occurred more frequently than JTOF (54.0% and 46.0%, respectively). Patients with JTOF presented at an average age of 11.8 years; whereas, those with JPOF presented at an average age of 17 years.
Characteristics of Juvenile Ossifying Fibroma (JOF)

* JTOF = juvenile trabecular ossifying fibroma; JPOF = juvenile psammosatoid ossifying fibroma.
Accurate diagnosis of fibroosseous lesions can be challenging. The rare incidence, rapidly progressive nature, and various inconsistent classifications of JOF have made these lesions especially difficult to diagnose (Osunde et al., 2013). The monostotic nature of ossifying fibroma has been previously described as a major differentiating factor from fibrous dysplasia (Osunde et al., 2013); however, the polyostotic JOF case described indicates that this may no longer be accurate. When diagnosing a polyostotic fibroosseous lesion, it is important to not exclude the possibility of JOF because this may warrant a different treatment.
A diagnosis of JOF is based on the clinical, radiographic, and histological characteristics of the lesion in question. Juvenile ossifying fibroma is characterized by a more aggressive clinical course and a higher recurrence rate compared with fibrous dysplasia, and surgical intervention is thus recommended. Asymptomatic, incidentally discovered lesions consistent with fibrous dysplasia may be followed clinically (Saglik et al., 2007); although, these lesions may be unpredictable in nature (Urata et al., 2007). Radiographic examination of JOF demonstrates a well-circumscribed, spherical lesion. In contrast, fibrous dysplasia is characterized by a lesion that maintains the shape and configuration of the involved bone, with a poorly defined border blending in with the surrounding normal bone (Owosho et al., 2014). If a diagnosis of JOF is unable to be made from either clinical or radiographic characteristics, a tissue diagnosis is warranted, whereby the histologic features (Voytek et al., 1995) and both molecular and immunologic characteristics may assist in differentiating between fibrous dysplasia and ossifying fibroma (Toyosawa et al., 2007). The patient presented was initially observed at an outside facility. Whereas initial observation may be reasonable in the management of fibro-osseous lesions with a more benign course, the aggressive nature of his rapidly growing lesions warranted early surgical biopsy to direct therapy.
Surgical resection is the preferred management of JOF, the extent of which depends on the anatomic location and behavior of the lesion (Brannon and Fowler, 2001; Abuzinada and Alyamani, 2010). Some authors recommend conservative excision or curettage (Slootweg and Muller, 1990; Terry, 1997). However, recurrence rates as high as 25% to 58% are possible with subtotal resection (Johnson et al., 1991; Waldron, 1993; Brannon and Fowler, 2001; Leimola-Virtanen et al., 2001; Osunde et al., 2013). Recurrence is generally attributed to incomplete resection, resulting in residual disease (El-Mofty et al., 2001). In a review of 86 cases, no recurrence was noted in patients who were followed for upto 7 years after complete surgical resection (Makek et al., 1983). To decrease the rate of recurrence, many authors thus advocate complete excision (Slootweg et al., 1994; Leimola-Virtanen et al., 2001; Slootweg and El-Mofty, 2005). Complete block resection is indicated in aggressive lesions showing rapid growth, thinning of cortical bone or tooth displacement (Abuzinada and Alyamani, 2010). The tumor mass must be removed to the level of normal bone with preservation of possible nearby vital structures (Sarode et al., 2011). Patients require long-term follow-up for surveillance for recurrence.