
Abstract
This report describes a case of successful orthodontic treatment using maxillary anterior segmental distraction osteogenesis with an internal maxillary distractor and bilateral sagittal split ramus osteotomy in a girl with cleft lip and palate. A 16-year-old girl with unilateral cleft lip and palate exhibited midface retrusion because of growth inhibition of the maxillary complex and mandibular excess. After the presurgical orthodontic treatment, 6.0-mm advancement of the maxillary anterior segment and 4.0-mm set back of the mandible were performed. After a retention period, the patient's midface convexity was greatly improved and the velopharyngeal competence was preserved without relapse.
The treatment outcomes of cleft lip and palate (
However, there remain patients with severe maxillary deficiencies requiring orthognathic surgery. Anterior maxillary repositioning via Le Fort I osteotomy is a common option in such cases, although it may result in speech problems because of the side effect of nasopharyngeal incompetency. Furthermore, patients treated with conventional Le Fort I osteotomy tend to relapse in cases that require moderate to large advancements of the maxilla (Rachmiel et al., 2012). Distraction osteogenesis (
Maxillary anterior segmental osteogenesis (
In this report, we describe the case of a patient with CLP, severe concave profile, a long face, negative overjet, and class III malocclusion as a result of maxillary hypoplasia who underwent successful orthodontic treatment combined with MASDO.
Case History
The patient was a girl aged 16 years and 6 months with a repaired unilateral CLP on the right side. Her chief complaints were a concave facial profile and anterior crossbite at the start of the second phase of orthodontic treatment. The patient's first visit to our orthodontic clinic was at 5 years of age, and she had a history of cheiloplasty and palatoplasty in infancy. During the first phase of orthodontic treatment, maxillary lateral expansion using a quad-helix appliance and maxillary protraction headgear was performed. A 0.022-inch preadjusted edgewise appliance was placed in the upper dental arch at 10 years of age, followed by alveolar bone grafting at 11 years of age. The upper anterior teeth were effectively aligned, and all appliances were removed with the placement of a removable retainer in the upper arch at 12 years of age. The growth of the mandible was subsequently monitored until 16 years of age. At the start of the second phase of treatment, a facial analysis showed a severe concave profile without facial asymmetry (Fig. 1). The profile included a long lower third of the face despite the patient's short upper lip and acute nasolabial angle. The occlusion was classified as an angle class III molar relationship on both sides with an overjet of–6.0 mm and overbite of+2.0 mm (Fig. 1). The upper right lateral incisor was congenitally missing, and the upper left second premolar was palatally dislocated. In addition, a lateral crossbite was noted on the left side, and the upper skeletal and dental midlines both deviated 1.5 mm to the right relative to the facial midline, whereas the lower skeletal and dental midlines coincided with the facial midline.
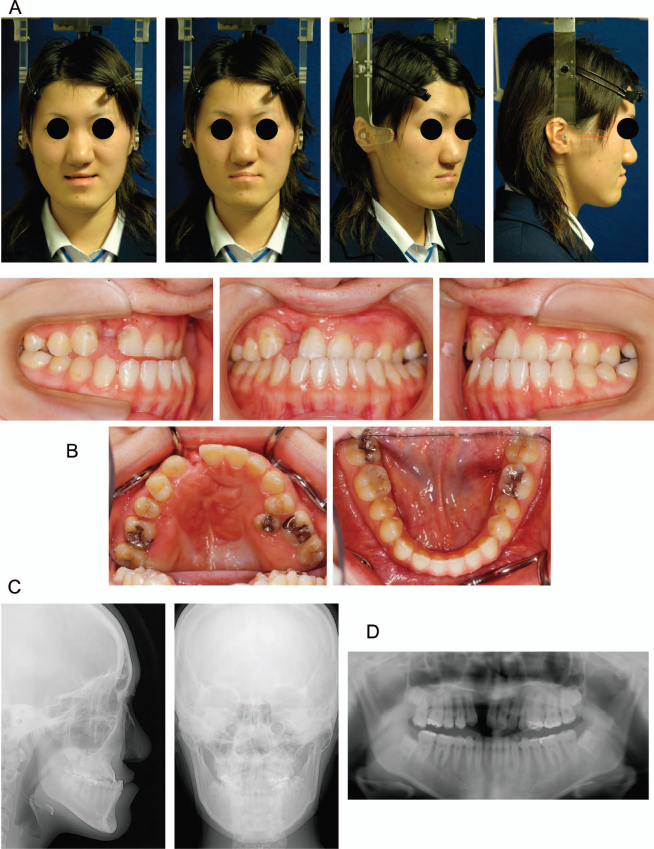
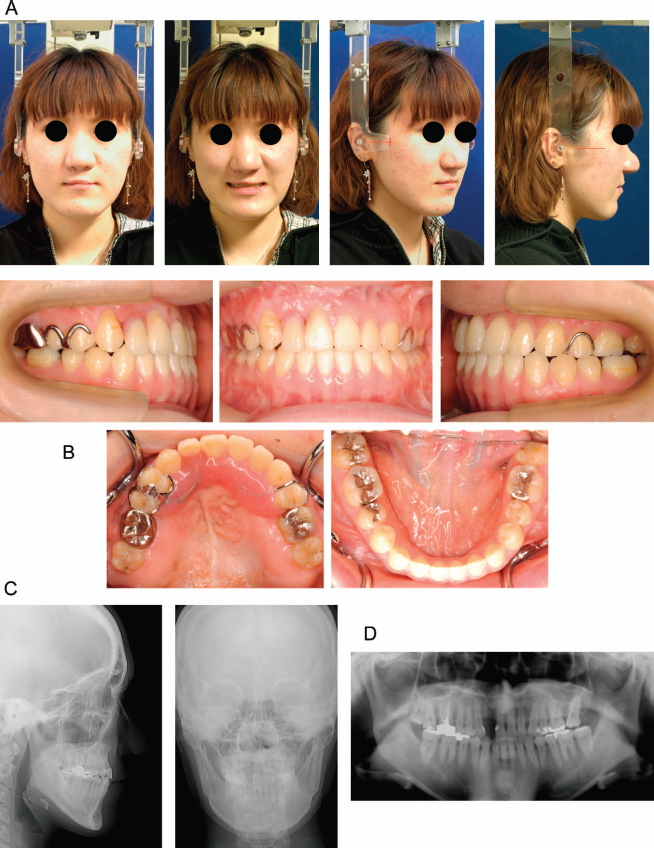
Pretreatment records (age, 16 years and 6 months). A: Facial photographs. B: Intraoral photographs. C: Frontal and lateral cephalograms. D: Panoramic radiographs.
A cephalometric analysis (Table 1) showed a skeletal class 3 jaw base relationship (point A-nasion-point B angle [ANB] = –7.9 degrees) with a small retropositioned maxilla and comparatively large mandible (articulare [Ar] to gonion [Go] = 51.8 mm) in comparison with the normative Japanese mean (Wada, 1977). The upper incisors showed normal inclination, whereas the lower incisors were lingually inclined (lower incisor [L1] to Frankfort horizontal plane [FH] = 72.0 degrees, L1 to mandibular plane [Mp] = 74.5 degrees). A speech evaluation and nasoendoscopy were conducted by a speech therapist prior to treatment. The patient's speech was judged to be acceptable, and it was feared that any alterations would carry a risk of velopharyngeal incompetence following maxillary advancement.
Lateral Cephalometric Measurements
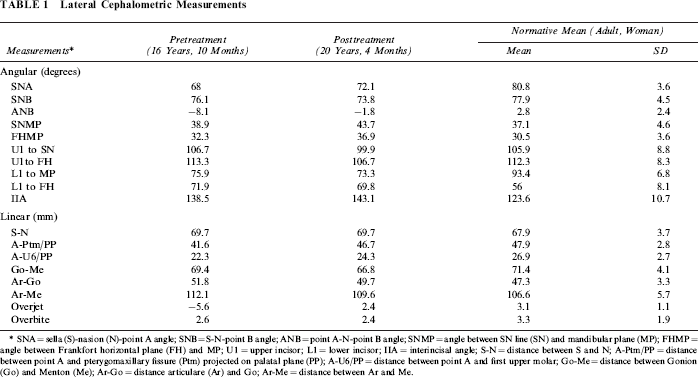
SNA = sella (S)-nasion (N)-point A angle; SNB = S-N-point B angle; ANB = point A-N-point B angle; SNMP = angle between SN line (SN) and mandibular plane (MP); FHMP = angle between Frankfort horizontal plane (FH) and MP; U1 = upper incisor; L1 = lower incisor; IIA = interincisal angle; S-N = distance between S and N; A-Ptm/PP = distance between point A and pterygomaxillary fissure (Ptm) projected on palatal plane (PP); A-U6/PP = distance between point A and first upper molar; Go-Me = distance between Gonion (Go) and Menton (Me); Ar-Go = distance articulare (Ar) and Go; Ar-Me = distance between Ar and Me.
Treatment Plan and Progress
The treatment objectives were to correct the patient's concave type profile caused by the maxillary retrusion and mandibular prognathism and simultaneously improve the anterior crossbite while establishing proper occlusion. The following treatment plan was proposed: (1) the placement of a preadjusted edgewise appliances in both arches; (2) maxillary forward advancement with MASDO; (3) closure of the distracted space and alignment of the malposed teeth; (4) mandibular set back via bilateral sagittal split ramus osteotomy (
At 16 years and 9 months of age, 0.022-inch slot preadjusted edgewise appliances were placed on all teeth, except for the upper second premolar. The patient subsequently underwent MASDO 8 months after appliance placement. An osteotomy line was drawn on the palate between the molars and premolars on the right side and canines and first premolar on the left side because of palatoversion of the second premolar. The distractor (Dynaform system; Stryker Leibinger Micro Implants, Kalamazoo, MI) was fixed to the hard palate with microscrews in the planned position (Fig. 2). After a 7-day consolidation period, distraction was started at 1 mm a day. During this time, we assessed the amount and direction of movement of the maxillary anterior segment on radiography. Both maxillary protraction headgear and class III intermaxillary elastics were used to support the internal device. Advancement was carried out without complications, and the maxillary anterior segment was distracted 6-mm forward in total. The segmented teeth sections were continuously fixed with a 0.019 × 0.025 stainless steel arch wire. After a 3-month retention period, the distractor was removed and fixation of the maxilla with titanium mini-plates was conducted under local anesthesia. We initially planned to align the upper second premolar dislocated palatally using the space produced by the MASDO procedure. However, the patient wished to complete the orthodontic treatment with braces as soon as possible, and we decided to extract the second premolar. The distracted space was subsequently closed by mesializing the molars using the end of the mini-plates, which were exposed from the gingival mucosa for absolute anchorage. Two years after the MASDO procedure, bilateral SSRO was performed to correct the patient's mandibular prognathism and anterior crossbite (Fig. 3). The amount of mandibular setback was approximately 4.0 mm on both sides. At the same time, bone grafting was performed to repair the alveolar ridge. Postsurgical orthodontic treatment was then applied to gain good occlusion. All appliances were removed at 20 years and 4 months of age, and Begg-type retainers with an artificial tooth for the upper right lateral incisor were placed in both dental arches. Nose and lip revision surgery was carried out the following year. Finally, the upper right lateral incisor was replaced with a removable partial denture.
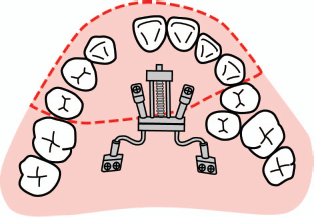
Schematic image of distracter placement on the palate. The dotted line designates the osteotomy line for maxillary anterior segmental osteogenesis.
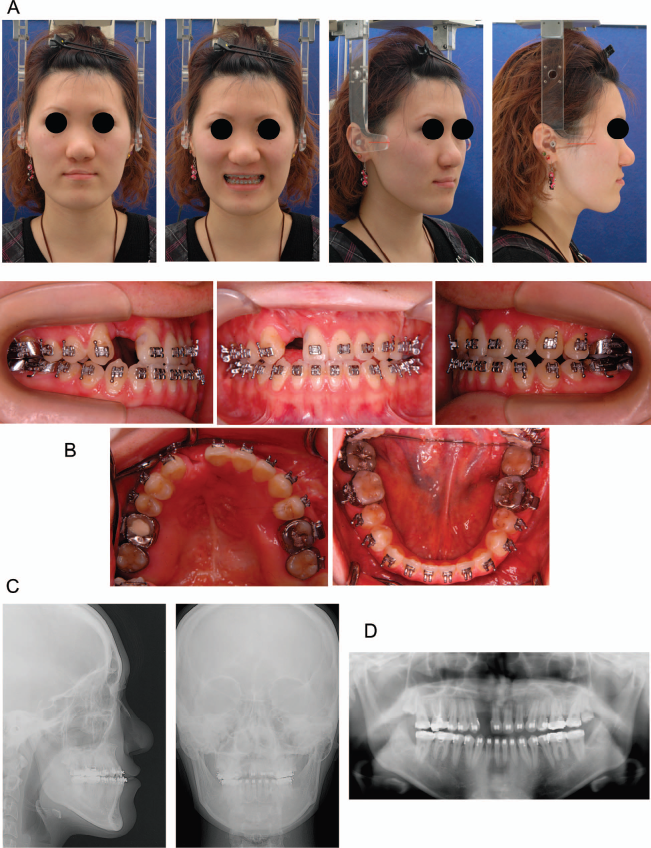
Preoperative of sagittal split ramus osteotomy records (age, 19 years and 5 months). A: Facial photographs. B: Intraoral photographs. C: Frontal and lateral cephalograms. D: Panoramic radiographs.
Treatment Results
The orthodontic treatment resulted in favorable facial aesthetics and occlusion; the patient's concave-type facial profile changed to a straight-type profile, and the nasolabial angle increased. The results of the cephalometric analysis are presented in Table 1. The maxillary anterior segment was successfully advanced 6.0 mm at A point, and the mandible was set back 4.0 mm at B point relative to the FH perpendicular line. The ANB angle changed from –7.9 to –1.9 degrees. Both arches were well aligned, and a proper overjet and overbite with a tight occlusal relationship between the maxillary and mandibular teeth were achieved. In addition, a class I molar relationship on the right side and class II molar relationship on the left side with tight intercuspation were obtained, and the dental midlines were coincident with the facial midline (Figs. 4 and 5).

Posttreatment records (age, 20 years and 4 month). A: Facial photographs. B: Intraoral photographs. C: Frontal and lateral cephalograms. D: Panoramic radiographs.
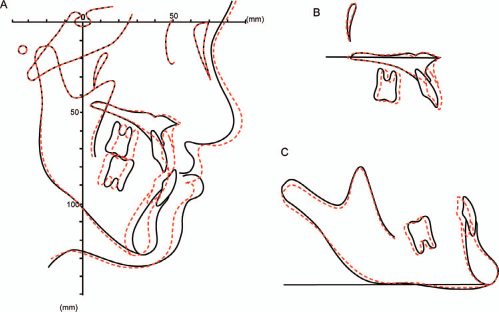
Superimposed cephalometric tracings: pretreatment (solid line) and posttreatment (dotted line). A: Superimposed on the sella-nasion plane at sella. B: Superimposed on the palatal plane at anterior nasal spine. C: Superimposed on the mandibular plane at menton.
Postoperative speech assessments showed no changes in the patient's velopharyngeal function after the surgery. These results remained stable during the retention phase (Fig. 6).
Postretention records (age, 22 years and 4 months). A: Facial photographs. B: Intraoral photographs. C: Frontal and lateral cephalograms. D: Panoramic radiographs.
Discussion
A previous study demonstrated that 25% to 60% of CLP patients require maxillary advancement to correct maxillary hypoplasia and improve the aesthetic facial proportions (Figueroa et al., 1999). The patient achieved an improved posterior crossbite and ameliorated crowding of the upper frontal teeth during the first phase of treatment; however, concavity of the soft tissue profile and an anterior crossbite remained. These problems were caused by both maxillary retrusion and mandibular protrusion, which required upper and lower jaw surgery. The major objectives of treatment in CLP patients undergoing orthognathic surgery are to establish an aesthetic profile with harmonious dental occlusion. However, the use of surgical maxillary advancement to improve severe skeletal discrepancies makes stabilization more difficult and increases the risk of speech problems.
Conventional Le Fort I osteotomy is often performed to improve maxillary hypoplasia in CLP patients. However, varying degrees of relapse have been reported, depending on the magnitude and direction of the surgical movements (Tong et al., 2003; Karakasis and Hadjipetrou, 2004).
In contrast, DO provides an alternative method for achieving maxillary advancement. Many studies have reported the efficiency of maxillary DO over conventional Le Fort I osteotomy in terms of stability (Cheung et al., 2003; Figueroa et al., 2004; Satoh et al., 2004; Rachmiel et al., 2012). For example, Gateno et al. (2003) found DO of the maxilla to be superior to conventional orthognathic surgery in CLP patients who require more than 6 mm of maxillary advancement.
On the other hand, the possible effects of maxillary advancement on speech and the velopharyngeal function must be taken into consideration. Anterior advancement of the entire maxilla in CLP patients carries a risk of shortening the soft palate, which may result in velopharyngeal insufficiency (Guyette et al., 2001; Satoh et al., 2004).
Several surgical procedures for MASDO have been reported, and tooth- or bone-borne extraoral distractors can be applied to adjust the force vectors three-dimensionally, although the use of bulky rigid external distractors may induce mental stress for the patient (Wang et al., 2009; Gao et al., 2014). The Dynaform system was originally developed to promote mandibular distraction osteogenesis, and we applied this device as an intraoral maxillary distractor secured on the palatal bone (Iida et al., 2007). The distractor was carefully positioned on the palate so that the anterior segment could be elongated in the proper direction. This method, in which the posterior segment theoretically receives a force in the posterior direction, does not cause unexpected widening of the pharyngeal depth. In past reports, no patients have exhibited signs of velopharyngeal morphologic changes or speech deterioration (Karakasis and Hadjipetrou, 2004; Iida et al., 2007; Wang et al., 2009; Aikawa et al., 2010; Okushi et al., 2011). The patient showed no speech deterioration in the postoperative period, and an excellent aesthetic profile and stable occlusion were simultaneously achieved in this case. The formation of a space between the anterior and posterior segments of the dental alveolus is one of the disadvantages of this procedure when compared with conventional treatments (Iida et al., 2007). In this case, the distracted space was closed orthodontically via mesial movement of the molars.
The Dynaform system can allow linear advancement of the maxillary segment in a single vector. To achieve sophisticated three-dimensional positioning of the anterior segment, face mask-type protraction headgear was also used as auxiliary treatment in this case, and careful observation and continuous anterior traction with elastics during both the distraction and consolidation periods helped to obtain precise positioning of the maxilla. Close interdisciplinary cooperation between the oral surgeon and orthodontist should be encouraged in such cases. Combined orthodontic and orthognathic surgery with MASDO is expected to become an established standard treatment option for maxillary correction in CLP patients.
Conclusion
In the present case, orthodontic and orthognathic treatments were applied in a CLP patient with midface retrusion and mandibular excess. Maxillary advancement via MASDO and subsequent mandibular set back using SSRO were performed for the patient. MASDO appeared to be superior to conventional Le Fort I osteotomy in stabilization and the effect on speech. On the other hand, the direction of advancement is limited, and the generated space in the dental arch should be closed. The present case obtained remarkable improvements in the patient's facial aesthetics and occlusion without disturbing her speech mechanisms.