
Abstract
Objective
To determine the repeatability and reproducibility of using three different viewing media to assess the outcomes of the dental arch relationships of patients with unilateral cleft lip and palate (UCLP) using the GOSLON Yardstick.
Design
The GOSLON Yardstick was used to rate the dental arch relationships of 29 patients with UCLP. Three experienced calibrated orthodontists rated the plaster study models, digital study models, and stereoscopic projected three-dimensional (3D) study models separately. There was a minimum of a 1-week interval between each rating session. All three rating sessions were repeated 1 month later. A linear weighted kappa statistic was performed to assess intrarater repeatability and inter-rater reproducibility, as well as the comparison between different viewing media using Kendall's Coefficient of Concordance (Kendall's W) statistic.
Results
Intra-rater repeatability was very good for all three viewing media (kappa = 0.83-0.92). Inter-rater reproducibility was good to very good across the three viewing media (kappa = 0.63-0.88). Agreements between plaster study models and digital study models or stereoscopic projected 3D study models were good to very good (kappa = 0.78-0.97 and kappa = 0.72-0.97, respectively), and a Kendall's W ranging from 0.86 to 0.92 (P < .001).
Conclusions
Stereoscopic projected 3D is an alternative method to assess the outcomes of dental arch relationships in patients with cleft lip and palate using the GOSLON Yardstick. It could also be used for viewing patient records, as it recovers the full 3D information captured at the time of the clinical examination.
Cleft lip and palate is the most common congenital craniofacial dysmorphology (Lages et al., 2004; Oliveira et al., 2014; Gassling et al., 2015). Treatment involves numerous surgical interventions from birth to adulthood. Although the primary aim of surgery is to improve facial appearance and function, there is a well-reported iatrogenic negative effect on maxillary growth, often resulting in three-dimensional (3D) dental arch constriction (Liao and Mars, 2005; Oliveira et al., 2014).
The outcomes of these surgical interventions have been evaluated by various indices or scoring methods. The GOSLON Yardstick was found to be the most commonly used method; it categorizes the dental arch relationships in the late mixed or early permanent dentitions of patients with unilateral cleft lip and palate (UCLP) (Mars et al., 1987; Altalibi et al., 2013; Jones et al., 2014). The GOSLON Yardstick was originally designed to rate dental arch relationships on plaster study models (Mars et al., 1987); it was later applied to three-dimensional (3D) digital study models (Dogan et al., 2012; Nicholls et al., 2014). Digital models have advantages over plaster models with respect to archiving and retrieval. However, any 3D surface scanned model is viewed on a conventional flat two-dimensional computer screen using “perspective projection.” Perspective projection is a technique of visualizing three-dimensional points on a two-dimensional plane, that is, an LCD monitor. The use of this type of projection is widespread—especially within the computer graphics industry—and produces images that are now routinely seen.
The true perception of depth, as in the human visual system, cannot be experienced until the image is viewed using a “stereoscopic viewer”; for example, passive or active 3D projection systems. Passive 3D projection systems utilize two projectors to respectively project two images with a spacial disparity onto a special screen. Using polarized 3D glasses, each image is viewed by each eye at the same time, thereby creating a stereoscopic effect and producing a 3D image within the brain (Chen et al., 2014).
It remains unknown whether stereoscopic projected 3D viewing is a valid and reproducible method of assessing outcomes in a clinical environment, as there are no reported uses of this technology in dentistry. Therefore, the aim of the study was to compare the repeatability and reproducibility of using three different viewing media (plaster study models, digital study models, and stereoscopic projected 3D study models) to assess the outcomes of the dental arch relationships in 9-year-old patients with unilateral cleft lip and palate using the GOSLON Yardstick.
Materials and Methods
Subjects
Following approval by the Institutional Review Board (IRB), the records of all patients with unilateral cleft lip and palate (UCLP) treated at the Cleft Lip and Palate Joint Clinic at the Prince Philip Dental Hospital from 2007 to 2013 were screened. Inclusion criteria were no previous orthodontic treatment or alveolar bone grafting, and intact plaster study models. Patients with craniofacial syndromes or anomalies were excluded. In total, 29 sets of plaster study models were included. The average age of the UCLP patients was 9.4 years ± 3.4 months (range 9-9.9 years); 6 were right-sided and 23 left-sided UCLP, 17 were women and 12 were men.
Conversion of Plaster Study Models to Digital Models
For each patient, the full upper and lower plaster study models were manually scanned, as were the buccal surfaces of the study models in occlusion, using a surface scanner (Lythos™ Digital Impression System, Ormco, Glendora, CA) and saved as STL files. Using VRMesh Design (Version 5.0, VirtualGrid, Bellevue, WA) the upper and lower digital study models were realigned to the buccal surface scan and saved as one STL file, producing full surface models in the correct occlusion for each patient (Fig. 1).
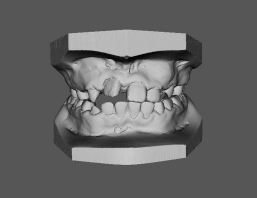
Digital models in occlusion.
Viewing Media
The dental arch relationships were evaluated using three viewing media: plaster study models, digital study models, and stereoscopic projected 3D study models.
Digital Study Models
Digital study models were viewed on a Dell PC computer (Dell Precision T5600) with a 24-inch LED wide screen monitor (Dell Inc., Austin, TX) using Di3Dview (Dimensional Imaging, Glasgow, U.K.) software. The digital study models could be rotated, magnified, and translated.
Stereoscopic Projected 3D Study Models
For stereoscopic 3D viewing, each STL file was reformatted using VRMesh Design (Version 5.0 VirtualGrid) and MeshLab (SourceForge, Urbandale, IA) and saved again in STL format. This pipeline was necessary to allow the viewing software to open the images. A passive 3D projection system (EB-W16SK; Epson, Suwa, Nagano, Japan), polarized glasses and 3D-Hub software (WSPav, Essex, U.K.; Instant Effects™, Santa Barbara, CA) were utilized to view the stereoscopic projected 3D study models on a large projector screen (Da-Lite Versatol Tripod Screen 99” [70 × 70] Silver Lite 2.5, Da-Lite®, Warsaw, IN; Fig. 2).

Raters viewing stereoscopic projected 3D study models (A). Note the horizontal disparity of the study models (B) that creates the depth perception.
Rating Scale
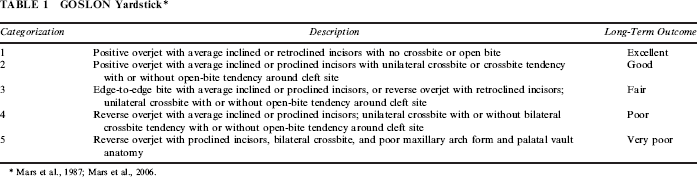
The GOSLON Yardstick was used to categorize the dental arch relationships in patients with unilateral cleft lip and palate into five groups (Mars et al., 1987). The details of categorization were shown in Table 1. The GOSLON Yardstick took sagittal, vertical, and transverse dental base relationships into consideration, while the anteroposterior relationship was of paramount importance.
GOSLON Yardstick*
Raters
A panel of raters comprised of three experienced orthodontists. All had previous experience in the treatment of patients with cleft lip and palate.
Rating Procedure
Considering stereoscopic projected 3D was a new concept to the three raters; a pilot study using six sets of study models were shown to the raters to acclimatize them to the three different viewing media. These six sets of study models were not included in the main study.
Calibration Session
A calibration session was conducted to discuss the rating procedure, as well as the rating scale. Raters were provided with the original paper describing the GOSLON Yardstick criteria as well as the master GOSLON models. These formed the basis of a discussion for the raters to reach a consensus regarding the GOSLON Yardstick. Raters were also instructed to keep the plaster study models in occlusion when rating all subsequent models.
Following calibration, three separate rating sessions were carried out on a total of 29 sets of study models. During the initial session (T1), the raters assessed the plaster study models, digital study models, and finally the stereoscopic projected 3D study models, all in standardized viewing conditions. Each rating session had a minimum of a 1-week interval in between. All three rating sessions were repeated 1 month later (T2) (Al-Omari et al., 2003). The order of the images was randomly allocated for each session by author (S.Z.) to reduce memory bias.
Statistical Analysis
As the GOSLON Yardstick is an ordered categorical scale, a linear weighted kappa statistic was performed to determine the intra-rater repeatability and the interrater reproducibility for the three raters, as well as the comparison between different viewing media using the Kendall's Coefficient of Concordance (Kendall's W). The null hypothesis stated there was no agreement (P < .05) in the GOSLON score among the three viewing media. Weighted kappa value indicated the level of reliability: less than 0.20 = poor; 0.21 to 0.40 = fair; 0.41 to 0.60 = moderate; 0.61 to 0.80 = good; and 0.81 to 1.00 = very good (Landis and Koch, 1977). The Statistical Analysis System (version 9.13: SAS Institute, Cary, NC) was used for the analysis.
Results
Intra-Rater Repeatability
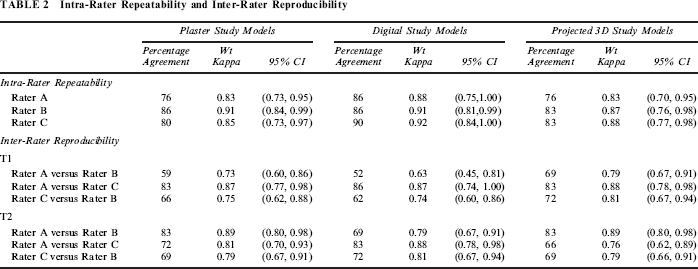
The intra-rater repeatability to assess the plaster study models, digital study models, and stereoscopic projected 3D study models was “very good” in between the two sessions (T1 and T2), with a weighted kappa score ranging from 0.83 to 0.92 (Table 2).
Intra-Rater Repeatability and Inter-Rater Reproducibility
Inter-Rater Reproducibility
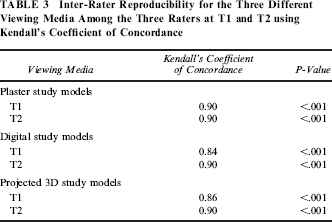
Inter-rater reproducibility showed “good” to “very good” agreement, with a weighted kappa score ranging from 0.63 to 0.88 (Table 2). This was confirmed with the Kendall's Coefficient of Concordance ranging from 0.84 to 0.90 (P < .00; Table 3).
Inter-Rater Reproducibility for the Three Different Viewing Media Among the Three Raters at T1 and T2 using Kendall's Coefficient of Concordance
Agreement Between Different Viewing Media
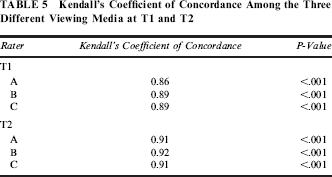
The weighted kappa value for the agreement between plaster study models and digital study models among the three raters had inter-rater reproducibility ranging from 0.78 to 0.97, indicating “good” to “very good” agreement. The agreement between plaster study models and stereoscopic projected 3D study models was also “good” to “very good,” ranging from 0.72 to 0.97 (Table 4). This was confirmed with the Kendall's Coefficient of Concordance ranging from 0.86 to 0.92 (P < .001; Table 5).
Intra-Rater Repeatability Between Different Viewing Media at T1 and T2

Kendall's Coefficient of Concordance Among the Three Different Viewing Media at T1 and T2
Discussion
The objective of this investigation was to determine if stereoscopic projected 3D study models could be used to assess the dental arch relationships in patients with UCLP at 9 years of age using the GOSLON Yardstick.
Although the GOSLON Yardstick was originally developed to assess the dental arch relationships of 10-year-old children with unilateral cleft lip and palate in the early permanent dentition (Mars et al., 1987; Hathorn et al., 1996; Mars et al., 2006), the application of the GOSLON Yardstick to 9-year-old plaster study models and digital study models have also been previously reported (Southall et al., 2012; Nicholls et al., 2014).
The results of the present study were similar to previous studies regarding the intra-rater repeatability and inter-rater reproducibility (Dogan et al., 2012; Nicholls et al., 2014). The studies involved two raters comparing plaster study models and digital study models found “very good” intra-rater agreement for both types of viewing media. In addition, the present study found the intra-rater agreement for rating the models using a stereoscopic 3D projector was also “very good” (weighted kappa 0.83-0.88). Similar results were found for inter-rater reproducibility with both studies reporting “good” to “very good” agreement for plaster study models and digital study models. The present study also found “good” to “very good” inter-rater agreement when scoring models using the stereoscopic 3D projector.
The basis for taking clinical records is to take a “snapshot” of the patient at that point in time, either for treatment planning, assessing outcome, or monitoring intervention or growth. Plaster study models fit this purpose well. However, there are storage and degradation problems over time; to overcome this, 3D digital study models were suggested. Digital study models provide 3D coordinate data for accurate angular and linear measurements (Tran et al., 2003; Luu et al., 2012) and allow viewing on a flat computer screen by creating the illusion of depth. Their use in rating the outcome of UCLP treatment based on the GOSLON score has previously been reported (Dogan et al., 2012; Nicholls et al., 2014). Advances in virtual reality technology allow individuals to view 3D images not on a flat screen but in “true 3D,” thus restoring the snapshot in time to provide a more realistic clinical representation. The GOSLON Yardstick is an ordered and categorical classification system based on visually assessing the dental study models and determining the score. It is essential that any viewing media should maintain the correct visual perspective to ensure the correct scores are given.
Stereoscopic 3D projection uses the same principles of human depth perception to “recover” the 3D image. It has been reported that there is no significant difference between active and passive 3D projection systems (Chen et al., 2014). Active 3D projection systems require “active shutter 3D glasses,” while passive 3D use “polarized 3D glasses.” In common with the human visual system, passive 3D projection uses dual projection to generate two images with a horizontal separation (disparity). The two slightly different images are viewed through the polarized filters in the glasses and the special screen. This allows the rater to simultaneously see the left image in the left eye and the right image in the right eye. The brain then uses the disparity to calculate depth. It is important to obtain the correct disparity to produce the correct amount of depth perception and prevent image distortion. Any optical distortion—for example, perceived size of overjet or extent of posterior crossbite—may affect the GOSLON score. As in previous studies, the present study found “good” to “very good” agreement of the GOSLON score when using plaster study models and digital study models to assess the dental arch relationships in patients with unilateral cleft lip and palate (Dogan et al., 2012; Nicholls et al., 2014). In addition, we found “good” to “very good” agreement of the GOSLON score when using plaster study models and stereoscopic projected 3D study models.
Since plaster study models are regarded as a gold standard in diagnoses, treatment planning, and patient records, the high levels of agreement between plaster study models and digital study models or stereoscopic projected 3D study models indicate that they could be utilized as alternative viewing media. On a broader scale, this technology may lend itself to future aspirations of providing clinicians with a simulated training environment based on 3D projection, augmented reality, and haptic technology in an attempt to replicate the physical world.
Conclusions
Stereoscopic projected 3D is an alternative method to assess the outcomes of dental arch relationships in patients with cleft lip and palate using the GOSLON Yardstick. It could be utilized as an alternative method in diagnoses, treatment planning, and viewing patient records that can recover the full 3D information captured at the time of the clinical examination.
Footnotes
Acknowledgments
The authors would like to thank Dr. Hassan Yang Rafidah for locating the plaster models of the UCLP patients, Dr. Zamri Radzi, Faculty of Dentistry, University of Malaya, Malaysia, for providing a copy of the master GOSLON models, Ormco for access to the Lythos scanner, and the Faculty of Dentistry, University of Hong Kong, for access to the 3D projection system.