
Abstract
Objective
Review of patients who underwent secondary alveolar bone grafting for total inpatient stay, postoperative complications, and postoperative analgesic requirements.
Design
Retrospective analysis of medical records.
Setting
Tertiary care center as part of a regional cleft lip and palate network.
Patients
All patients who underwent secondary alveolar bone grafting from the iliac crest.
Interventions
Local anesthetic was infiltrated overlying the anterior iliac crest. An incision was made to conform to the future skin crease and avoid muscle dissection. The cartilaginous cap was incised and raised, and cancellous bone was then harvested. The cavity was packed with hemostatic cellulose and closed in layers. All patients received postoperative antibiotics. All patients were prescribed regular paracetamol (acetaminophen) and ibuprofen if there were no contraindications. Oral morphine was available when requested.
Main Outcome Measures
Length of stay, postoperative analgesic requirements, and postoperative donor site and oral complications.
Results
From 100 consecutive patients, 92 (92%) of the patients were discharged the day after surgery; one (1%) patient required four nights of monitoring for postoperative pyrexia of unknown origin. All patients received regular paracetamol, and the majority (86%) did not require oral morphine. Complications included seroma (4%), superficial donor site abscess (1%), postoperative pyrexia of unknown origin (2%), gingival bleeding (2%), and oral infection (2%).
Conclusion
The findings suggest that donor site pain may be well controlled with simple, regular analgesia. Children tolerated this procedure well and were safely discharged the day after surgery. Alveolar bone grafting from the iliac crest was found to have low complication rates.
The North West, Isle of Man and North Wales regional Cleft Lip and Palate Network provides services for 3000 children and adults. Part of this service is to deliver multidisciplinary management in alveolar bone grafting. Closure of the residual alveolar cleft with bone graft was recorded as early as the 20th century, and primary and early secondary grafting was routinely performed in the 1950s (Lilja, 2009). Secondary grafting provides a means of stabilizing the maxillary arch and adjacent teeth, thereby facilitating canine eruption and enabling orthodontic and restorative treatment (Enemark et al., 1985).
Maxillary expansion and cancellous bone graft into the mucoperiosteal pocket beneath the nasal floor allows spontaneous eruption of the canine through a stable segment (Felstead et al., 2010). In addition, the alar base is raised to a more desirable anatomic location with the opportunity to close preexisting oronasal fistulae (Lilja, 2009). The mainstay of current management has largely remained with the approach of Koberg and Ross: identifying restrictions in maxillary growth when performing primary bone grafting (Ross, 1987). Secondary grafting during mixed dentition is now accepted practice worldwide. Success rates are closely monitored in the United Kingdom (UK) since the Department of Health charged the Clinical Standards Advisory Group (CSAG) to investigate outcomes in UK children. This was in response to 60% of UK children acquiring successful grafts compared with 97% from equivalent European centers (Grunwell et al., 2000).
Survival of donor graft with low donor site complications is imperative with the current gold standard, the iliac crest. As Johanson and Röckert (1961) demonstrated in histologic specimens, bone harvested from the iliac crest conformed to a similar construct to that of alveolar native tissue. Microradiographic analysis 6 months after the graft procedure showed that the graft site was indistinguishable from unaffected palate. The functional requirements of the graft were found to persist long-term (Lilja, 2009).
Up to 50 cm3 of bone can be harvested with ease of access utilizing a posterior or anterior approach with favorable osteoconductive and osteoinductive properties. (Vura et al., 2013). Though debated, morbidity is largely considered minimal upon physical, clinical, and radiologic examination (Kolomvos et al., 2010). Radiographic assessment of the donor site reveals a degree of individual variation during the development of new bone stock (Vura et al., 2013). Formation of new bone is stimulated on the surface of remaining trabeculae and allows in-growth from adjacent surrounding native segments (Lilja, 2009). Cortical bone cells require restoration of flow in existing vessels and therefore are unlikely to survive at the recipient site and are not often described in the literature (Al-Asfour et al., 2013).
With 11 regional specialist cleft teams in the UK, we decided to evaluate current donor site outcomes from a single surgeon, with primary focus upon inpatient analgesic requirements, length of inpatient stay, and complication rate.
Methods
A retrospective review was conducted for 100 consecutive cases under the supervision of a single surgeon (June 2011 to January 2015). All children with a cleft involving the lip were assessed clinically and radiographically by a cleft surgeon and orthodontist at the age of 8 years. An alveolar bone graft and, if required, presurgical orthodontic expansion was planned for children with a confirmed alveolar defect. Alveolar bone grafting is performed when the canine root is between one-third to two-thirds formed. All patients who underwent secondary alveolar bone grafting from the iliac crest were included. The donor site was assessed for the following:
In-patient postprocedure analgesic requirements
Total inpatient stay (days)
Postoperative complications
This study was registered and approved by the clinical audit department.
Standard Operative Procedure
All patients underwent the procedure under general anesthesia and antibiotic prophylaxis. A sandbag was placed beneath the donor hip. While supine, all patients underwent our preferred method of harvest (45 minutes), a two-team approach was employed to minimize operative time. Local anesthetic (long-acting 0.25% bupivacaine + 1:200,000 adrenaline) was infiltrated at the incision site: 4 mL was infiltrated to the subcutaneous tissues and a further 6 mL to the deeper layers to the level of the cartilaginous cap. A 3-cm incision overlying the anterior iliac crest was made through skin (Fig. 1). This is a different angle of incision from that often described in the literature, but it was done in an attempt to conform to a future skin crease. The future skin crease is the groin crease that is expected to remain consistent as the child ages. This is delineated by applying gentle pressure to the superior groin surface, which develops a crease that can be used to estimate the future groin crease. Skin incisions overlying the iliac crest also lead to delayed healing (Laurie et al., 1984). Skin is then transposed, with an incision lateral to iliacus and medial to the gluteal muscles to avoid muscle dissection. The overlying cartilaginous cap was sharply incised in a longitudinal fashion parallel to the crest, with a Y-incision distally. The cartilage flaps were raised (Fig. 2). Cancellous bone was harvested with a Gouge and Volkmann spoon. The cavity is packed with hemostatic cellulose with meticulous closure in layers: cartilage (2/0 Polysorb™), periosteum and subcutaneous tissue (3/0 Polysorb™), and skin (3/0 Biosyn™) (Medtronic, Minneapolis, MN). A small dressing was applied after placement of wound adhesive strips.

Planning of a skin incision for bone harvest to an anterior iliac crest that conforms to a future skin crease.

Cartilaginous cap reflected and cancellous bone harvest using a gouge.
Perioperative Protocol
Antibiotics
Intravenous antibiotics were administered on induction with two postoperative doses. Broad spectrum oral antibiotics were then supplied for 1 week.
Analgesia
Paracetamol (acetaminophen) was given intravenously every 6 hours, and this was converted to oral equivalent when oral intake was adequate. Ibuprofen was given orally every 8 hours if there were no contraindications. Analgesia was alternated to avoid peaks and troughs in an attempt to maintain analgesic steady state. Oral morphine was available when requested. All analgesia was prescribed according to weight. A further week supply of oral paracetamol and ibuprofen was prescribed upon discharge.
Feeding
Patients were encouraged to limit oral intake to a soft diet for 3 weeks. Meticulous oral hygiene with supplementary mouthwash was also recommended.
Discharge
Children were deemed suitable for discharge when a soft diet was tolerated and they were able to ambulate freely on the ward. All parents were involved in the discharge decision. Parents were asked if the child had returned to normal intake. Any parental concerns were addressed, and the authors had a low threshold for a period of observation in hospital if there were any clinical concerns.
Statistics
A Student's t test and a χ2 test were used for statistical analysis. A P value <.05 was considered significant.
Results
The study had the following characteristics:
One hundred consecutive patients were reviewed: 62 boys and 38 girls.
Distribution of clefts was seven bilateral, 93 unilateral.
Patients’ ages ranged from 7.75 to 16.34 years.
Mean age for graft placement was 9.8 ± 1.8 years.
The study period ranged from June 2011 to January 2015.
Gender (P = 1.00) and age (P = 0.72) were not found to influence length of stay. Most of the patients (92%) had an uncomplicated overnight stay (Fig. 3). Before they were discharged on the first postoperative day, patients had to have adequate oral intake and had to be moving freely. Seven patients (7%) required a further night's stay in the hospital for a variety of reasons: pain control, poor oral intake, postoperative pyrexia of unknown origin, or facial swelling. These patients were discharged on the second postoperative day after a further period of observation determined that their symptoms had improved. One patient (1 %) required an extended stay of 4 nights for postoperative pyrexia that was extensively investigated though no clear cause was identified.
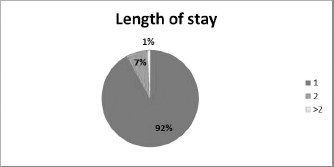
Length of stay in days.
All patients received regular paracetamol. Regular ibuprofen was administered in 95 patients (95%). One patient (1%) had severe asthma, and thus ibuprofen was avoided. Most patients did not require oral morphine (86%, Fig. 4).
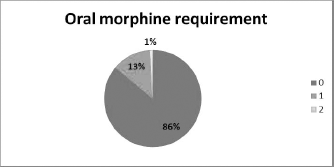
Oral morphine requirement in doses.
No gait disturbance was observed or recorded during postoperative visits. All patients were followed up for 3 months postoperatively to assess for long-term complications.
Complication rates were low and comparable to those of other studies (Vura et al., 2013). There were four seromas (4%), all of which resolved spontaneously with no surgical intervention. One patient (1 %) had a superficial donor site abscess that required incision and drainage 3 weeks postoperatively. Two patients (2%) had postoperative pyrexia of unknown origin, which resolved spontaneously.
In addition, there were oral complications. Two patients (2%) had postoperative gingival bleeding, which resolved after a period of observation, and an additional two patients (2%) had oral infections that required a course of oral antibiotics. None of the oral complications required operative management.
Discussion
It has been suggested that iliac bone graft harvest leads to significant pain, poor ambulation, and increased hospital stay when used as donor site in alveolar bone grafting (Meara et al., 2011). Alternative donor sites include calvarium, mandibular symphysis, and tibia (Vura et al., 2013). The ideal donor must consider viability, morbidity, volume, type of bone (cortical versus cancellous), regenerative properties, and psychological and functional outcomes from the surgery (Lilja, 2009). Our findings suggest that this donor site is well tolerated and has minimal impact on children resuming daily activities. Harvesting bone from the iliac region was sufficient in all children from a single donor site. Children usually returned to school by day 10. Studies of adults noted that pain persisted for up to 4 months in 10% of individuals as a result of muscular or periosteal injury or damage to local sensory nerves. This was not the case in our pediatric series, as sensory branches were carefully avoided to prevent concomitant muscle injury. We have shown that very few patients request opiate supplementation in addition to simple analgesia (paracetamol and ibuprofen). From experience, the authors and nurses have found that children in this age group will request analgesia when desired. This approach prevents added complications of drug toxicity and nausea.
Attempts to provide a solution to potential increased pain involved the use of continuous infusion with local anesthesia (Meara et al., 2011), neural blockade of the thigh (Paut et al., 2001), and bupivacaine-soaked absorbable gel foam at the donor site (Dashow et al., 2009) all of which suggest a benefit in reducing inpatient stay and promoting ambulation. We do not believe any of these methods are significantly beneficial in expediting discharge but potentially prolong it. One study found that pump use resulted in admission figures of 1.09 days versus 1.12 days (in the placebo group). The findings from our series suggest that the use of such pumps is not required and may potentiate complications from catheter use, infection, restricted mobility, migration, incorrect placement, and drug administration errors. In addition, at a cost of $100 per operation, use of a pump poses financial implications long term (Meara et al., 2011). Our findings are in keeping with those of Dawson et al. (1996), which demonstrated minimal use of PCA when offered (Dawson et al., 1996). Our preferred method in assessing pain was direct questioning and clinical observation of the child, including input from supervising nursing staff and parents.
Hospital stay in a similar series ranged from 3 to 5 days, with a median stay of 3 days; each of those patients received continuous infusion of bupivacaine and wound drainage systems (Swan and Goodacre, 2006). The current policy of our unit is to aim for discharge within 24 hours, thereby minimizing nosocomial infection and maximizing health service resources. Though we did not record specific validated pain scores in our series, such correlation with injury and severity in children is not representative (Baxt et al., 2004). Subjective and objective scores of children are unreliable compared with those of an adult population. Parental behavior affects children's reported pain scores, further compounding true outcomes. This may explain the placebo effect for continuous infusion, which had a high acceptance rate by families, independent of the amount of local anesthetic administered as identified in iliac bone graft harvest in adults in a randomized controlled study (Morgan et al., 2006). In our unit, months before surgery children are primed with a cartoon booklet describing the sequences involved in their procedure; there is also an adult version for parental review. The surgical, anesthetic, and nursing teams emphasize the importance of mobility and pain management. We have found that parents often respond favorably to the small size of the dressing placed over the wound. Studies have shown that wound size and appearance affect patient engagement in wound care (Gaind et al., 2011). Our scars measure no more that 3 cm, and 92% of the patients in a study were pleased when the length of incision was small (30 to 50 mm) (Albert et al., 2006).
Potential iliac crest complications include chronic pain, gait disturbance, numbness, (Eufinger and Leppanen, 2000), vascular injury, pathological fracture, herniation, hematoma, infection, and cosmetic deformity. A rare delayed complication is the development of an abscess years after harvest secondary to foreign body granuloma (De Riu et al., 2008). Our complication rates were low, and the seroma rate of 4% was comparable to those of other studies. There were no hematomas. Only one patient had a superficial donor site abscess requiring incision and drainage. This was complicated by delayed presentation and loss to follow-up secondary to social circumstances.
Limitation of the study include formal assessment of symptom-free recovery and time to return to normal function. In addition, our short follow-up period warrants revisiting to isolate long-term complications. A prospective study provides more accurate measures of data collection; however, the retrospective nature of the study lends itself to the assessment of outcome from analgesic protocol and surgical process.
Conclusion
Alveolar bone graft procedures utilizing iliac crest harvesting was determined to be a safe technique, provided that the operating surgeon has sound knowledge of anatomy and potential complications. We believe our incision and technique for iliac bone graft harvest has a role in minimizing postoperative pain by limiting deeper muscle dissection. We observed a better aesthetic scar that conforms to the future groin crease as the child ages.
This study demonstrates that children tolerate this procedure well and can be managed with simple analgesia. Other studies have promoted the use of infusion catheters for local analgesia, but our study shows that this is unnecessary as it limits mobility and carries the risk of potential complications. Children can be safely discharged after the first postoperative day with no restrictions on mobility. This minimizes inpatient stay and the potential side effects from more advanced analgesic methods or medications.