
Abstract

Allareddy V, Ross E, Bruun R, Lee MK, Shusterman S. Operative and immediate postoperative outcomes of using a Latham-type dentomaxillary appliance in patients with unilateral complete cleft lip and palate. Cleft Palate Craniofac J. 2015:52:405-410.
Here we go again! Failure to accept longitudinal outcome studies but accept unproven surgical procedures! The article by Allareddy et al. (2015) shows that the authors perhaps failed to read and understand the existing literature on the use of presurgical orthopedics with lip adhesion (POPLA) as described by Millard and Latham (1990) and later by a modification of their procedure by Grayson et al. (1999) called nasoalveolar molding. This procedure describes the modification of the Millard and Latham presurgical appliance (POPLA) that has been shown to have long-term negative effects on facial development (Berkowitz et al., 2004). Although the POPLA use was not extended into adolescence, I was able to do this and wrote a 40-year comparative study article (Berkowitz et al., 2004) on the ultimate negative occlusal outcome. This comparative occlusal study dealt with two procedures: a 20-year use of the conservative (non-presurgical orthopedic treatment [PSOT]) appliance compared with the occlusal outcome of POPLA appliance treatment.
The surgical literature often tends to report only new initial neonatal studies, believing the good facial findings of that period will extend into adolescence and adulthood. They are completely wrong! For example, those presurgical orthopedic appliance treatment (PSOT) procedures that bodily retrude the protruding premaxilla in complete bilateral cleft lip and palate cases caused a synostosis of the premaxillary vomerine suture, which negatively affected future palatal growth and dental occlusion. Many authors who lack longitudinal clinical knowledge falsely predict that modifications of a premodification, or yet another modification of a similar presurgical orthopedic appliance, will correct the problems that arose from an earlier version by another surgeon. Millard (1980), in his three-volume review of cleft palate surgery, Cleft Craft, reports on the many surgical modifications of previous procedures that have failed. Unfortunately, no long-term objective records of dental casts, cephalograms, or photographs were ever used to determine which biological concepts have been considered as the reason for failure (Fig. 1). Latham's thinking was a result of working in England with James Scott, an anatomist, who specialized on facial growth concepts. He left England, went to Canada, on to the University of North Carolina and then to Duke Medical School to join Georgiade (a plastic surgeon). They wrote an introductory article (Georgiade and Latham, 1975) introducing their new PSOT procedure but did not follow up with a subsequent review article describing the reasons why they abandoned the technique.
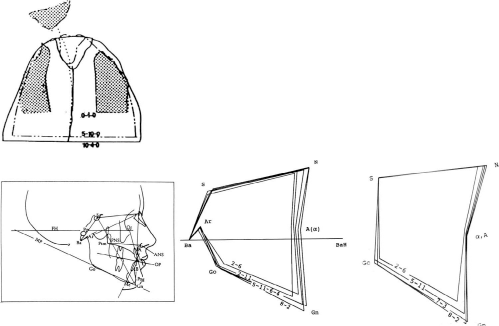
Complete bilateral cleft lip and palate. In NAM+GPP- and POPLA-treated patients with complete unilateral cleft lip and palate and complete bilateral cleft lip and palate, the premaxilla would be severely retruded, so much so that one or both lateral incisor cleft spaces would be closed and ultimately bridged by bone, thus preventing the orthodontic-orthopedic correction of the anterior crossbite. The lack of subsequent anterior maxillary and mandibular arch congruency would prevent the achievement of a good dental overbite/overjet relationship, even after midfacial surgical advancement. A slight anterior crossbite can be easily corrected orthodontically by using the maxillary protraction mechanics of a facial mask. In the non-POPLA complete unilateral cleft lip and palate cases, it was necessary to orthodontically advance a retrusive large alveolus and expand the smaller segment out of crossbite. The superimposed cephalograms show normal face tracings on the left compared with a recessive midface on the right caused by physically retruding the protruding premaxilla within the arch during the neonatal period.
Since Millard (Miami) strongly believed that for total longitudinal success it was important to complete all palatal surgery by 2 years of age, he asked Latham to join him and accept his modification of a lip adhesion and a periosteoplasty, thinking it would eliminate the need for secondary alveolar bone grafting (Millard and Latham, 1990). Between 1960 and 1980, and prior to the use of PSOT, Millard and I used a conservative treatment procedure that entailed the use of lip adhesion at 3 months for the molding of the cleft lip and palate followed by a lip revision between 6 and 8 months and palatal cleft closure between 18 and 24 months. Although speech language pathologists in the United States wished to close the cleft space between 6 and 8 months to obtain “good speech,” the European speech therapist, on the other hand, believed that good speech could still be obtained when cleft surgery was postponed to 5 to 9 years of age and that this timing would lead to more normal palatal and facial development. Their hypothesis of using delayed palatal surgery was relatively successful, and we therefore compromised at setting the age of palatal cleft closure at 18 to 24 months, thinking that although it would eventually necessitate some speech therapy, the attainment of all treatment goals of good facial aesthetics, dental occlusion, and psychological development could be achieved. The comparative 40-year outcome study using serial dental casts and photographs from the conservative treatment of complete unilateral and bilateral cleft lip and palate cases compared with the 20-year POPLA series procedures clearly showed that facial-palatal growth was of the essence and that any surgical-mechanical procedure that was performed at the neonatal period was highly disruptive to facial, dental, psychological, and speech development. Both Cutting (New York University) and Mulliken (Harvard) had adopted the POPLA technique, thinking that early surgery after palatal manipulation would yield the best long-term results. However, Cutting, after 15 years of using the POPLA technique, discontinued the procedure and introduced his modification: nasoalveolar molding (NAM) and gingivoperiosteoplasty (GPP). Even after using the POPLA procedure, he and Mulliken never published an outcome study. Contrary to Grayson's conclusion, a report by Hsin-Ye Hsieh et al. (2010) and some European clinics proved that there were no long-term benefits to support their use.
It would be very helpful to expect that every new or modified treatment procedure that is published in the Cleft Palate–Craniofacial Journal, Plastic & Reconstructive Surgery, or any other journal would be followed to 8 years of age with an outcome study report on facial growth changes so the surgeon can accept or reject the trial procedure.
The American Cleft Palate–Craniofacial Association's (ACPA's) program committee was dissatisfied that Millard and Latham failed to publish a follow-up study. They asked Matic (a surgeon who worked with Latham in Canada) and me to debate Latham and Morales (a surgeon) over their unreported long-term findings. Unfortunately, Latham did not produce any long-term records. Two other failed debates with Latham followed for the same reasons. The ACPA's program committee also had similar dissatisfaction with the lack of objective long-term NAM+GPP records. They again asked Matic and me to debate Cutting and Grayson for the same reasons, but Grayson failed to show up, leaving Cutting the sole defender of his procedure. He limited his presentation to the neonatal aesthetic improvement of the nose and lip, but no records on facial growth were presented.
Allareddy et al. (2015) did a good review of the United States and European literature concerning use of the PSOT procedure, citing studies against the use of PSOT (Chan et al., 2001; Prahl et al., 2001; Berkowitz et al., 2004; Brattstrom et al., 2005; Berkowitz, 2006; Bongaarts et al., 2006; Lee et al., 2008; Matic and Power, 2008; Berkowitz, 2009; Power and Matic, 2009; Nazarian Mobin et al., 2011; Dec et al., 2013) as well as studies for the use of PSOT (Millard and Latham, 1990; Grayson et al., 1999; Mulliken and Martinez-Perez, 1999; Grayson and Cutting, 2001; Grayson and Maull, 2004; Sato et al., 2008). Many of these authors support my criticism of PSOT of any design. Furthermore, the Taiwanese study (Hsin-Ye Hsieh et al., 2010) is the only clinic that performed a longitudinal cephalogram study on NAM+GPP and reported that severe midfacial recessiveness had occurred. Despite their review of the literature, Allareddy et al. chose to support the different modes of PSOT treatment. Why?
To achieve more successful treatment for patients and obtain all treatment goals, it is necessary that more orthodontists become involved with the study and guidance of growth and development from birth to adolescence. As a result of their special training, their role includes diagnosis of changing facial morphology and jaw function as a result of the anomaly, followed by its influence on growth. They provide orthodontic/orthopedic treatment and general expertise for consultation with all of the other members of the cleft and craniofacial team. Orthodontists are involved in one way or another with virtually all of the treatment procedures provided by all of the cleft palate–craniofacial team's specialists. Since palatal clefts vary in the extent of osteogenic and muscular deficiencies, surgeons should recognize that all clefts, although similarly classified, are not the same. Therefore, each case requires differential diagnosis and treatment planning. What may be the treatment of choice for one patient may be different for another, even if they have the same cleft type. As to the use of POPLA and NAM, I reject that either treatment procedure be considered in any case.