
Abstract
Background:
Blood loss during cleft palate surgery has been investigated in previous research, but there is no report regarding blood loss when performing Furlow's double opposing Z-plasty (DOZ). In the present study, we evaluated intraoperative blood loss in patients with cleft palate who underwent the DOZ procedure.
Materials and Methods:
Intraoperative blood loss was prospectively investigated in 59 patients undergoing palatoplasty with DOZ by a single surgeon between August 2012 and July 2013. Demographic factors and clinical status, including cleft type and palatal gap, were recorded. Blood loss was evaluated by measuring the change in weight of a suction bottle, suction line, and gauze balls.
Results:
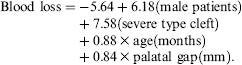
Mean blood loss was 16.61 ± 10.33 mL, which accounted for 5% of total blood volume. Male sex, older age, severe cleft type, larger palatal gap, relaxed incision, and increased operative time contributed to greater blood loss. The amount of intraoperative bleeding could be predicted by the following equation: Blood loss = -5.64 + 6.18 (male patients) + 7.58 (severe type cleft) + 0.88 X age (months) + 0.84 X palatal gap (mm).
Conclusions:
We found that the DOZ technique causes mild blood loss, but bleeding amount tended to increase in older male patients with a severe cleft and a larger palatal gap. The use of relaxed incisions during palatoplasty and prolonged operation times also contributed to greater blood loss.
Cleft lip and/or palate is the most common congenital craniofacial anomaly. Historically, primary repair of a cleft palate was usually conducted within the first 3 years of life, but it was not long before cleft palate surgery was carried out in infancy (Denk and Magee, 1996). Developments in anesthesiology and improved long-term outcomes led to earlier surgical correction. A recent study conducted by Katzel et al. (2009) revealed that most cleft surgeons perform palatoplasty when patients are between the ages of ± and 12 months to increase normal oral intake and to achieve better speech outcomes after surgery.
The whole blood volume of an infant can be roughly estimated as 70 to 80 mL per kilogram body weight; therefore, a small volume of blood loss may be a considerable burden in cleft patients. Furthermore, younger infants have a higher percentage of fetal hemoglobin, which has a lower oxygen delivery capacity. The precise assessment of blood loss during palatoplasty is a major concern because of the relatively small hemodynamic capacity in cleft patients.
Many cleft surgeons have presented information regarding blood loss during cleft palate surgery (Dingman et al., 1949; Mladick et al., 1967; Moore et al., 1988; Senders and Sykes, 1995; Kane et al., 2000). However, these data were derived from various surgical procedures by different surgeons. Detailed methods for blood loss estimation were not described, and the relationship of blood loss with cleft types was not fully discussed.
The purpose of the current study was to assess accurate blood loss during Furlow's double opposing Z-palatoplasty (
Materials and Methods
This prospective clinical study was designed to evaluate the amount of bleeding during palatoplasty. Approval for the study was granted by the institutional review board (no. 1209-107-429). Patients with isolated cleft palate or cleft lip and palate were candidates for the present study. Patients were excluded if they had syndromic anomalies, such as Pierre Robin sequence, Apert syndrome, DiGeorge syndrome, or VACTERL syndrome. Preterm infants and patients with accompanying congenital problems in other organs were also excluded. Finally, patients with laboratory abnormalities indicating a bleeding tendency or anemia were excluded from this study.
The DOZ palatoplasty was performed by a single surgeon (S.K.) in all patients. Briefly, the DOZ line was designed using Gentian violet. A local anesthetic solution of 2% lidocaine mixed with 1:100,000 epinephrine (Huons, Seongnam, Korea) was injected into the mucoperiosteum and the submucosal level in the velum along the line of the incision. The first incision was made 5 minutes later. On the oral surface, a right anteriorly based mucosal flap and left posteriorly based mucomuscular flap were developed with a central limb located on the cleft margin. Conversely, a right posteriorly based mucomuscular flap and left anteriorly based mucosal flap were created on the nasal surface. To close the hard palatal gap, mucoperiosteal flaps were elevated from the palatal shelf and brought together horizontally. In three patients with severe palatal gap (Veau 4), Vomer flaps were created to close the hard palate. In cases of a wide palatal gap, lateral relaxing incisions were made in the gingival hard palate of one or both sides to facilitate wound closure. We did not perform hamulus fracturing, transection of the tensor tendon, or dissection in the space of Ernst. We attempted to reduce the dissection area to minimize postoperative scarring and the risk of velopharyngeal insufficiency or maxillary retrusion. Bipolar cauterization and gauze ball compression were employed to control surgical bleeding. Hemostasis using bipolar cauterization was restrictively used to control evident bleeding that was not naturally controlled by gauze ball compression.
The amount of bleeding was calculated by measuring the change in weight of the suction bottle, suction line, and gauze balls. We prepared two separate suction systems: one for the bleeding from the surgical field and the other for the saliva or betadine solution. The rubber suction line contained a small volume of blood; therefore, we calculated the weight change of the suction line. Each gauze ball was used until fully soaked with blood and then wrapped in a plastic basket to prevent vaporization from the air exposure.
Demographic factors of sex, age, and weight were noted. Individual cleft type, the width of palatal gap, and operative time were measured. Cleft type was divided into mild and severe based on the Veau classification. Mild cleft includes Veau type I soft palate defects only and type II hard and soft palate defects. Severe cleft includes Veau type III involving the soft palate to the alveolus, usually involving the lip, and type IV of complete bilateral clefts of soft and hard palate, alveolus, and lip. The palatal gap was measured intraoperatively at the line traversing both sides of maxillary tuberosity using a Castroviejo caliper (Storz, Bausch & Lomb Corp., New York, NY). A complete blood count was performed preoperatively and 3 days postoperatively to examine the relationships between blood loss and change in laboratory indices.
Statistical Methods
Statistical analysis was conducted using the SAS program (version 9.3; SAS Institute Inc., Cary, NC). The relationship of blood loss with categorical and numeric variables was evaluated by using an independent t test and a correlation analysis, respectively. Scatterplots showed the relevance as a whole, and the degree of correlation was quantitatively evaluated using the Pearson correlation coefficient. A multiple linear regression analysis was used to assess significant independent variables influencing bleeding. The stepwise selection method was used to control multicollinearity between independent variables. P values < .05 were considered statistically significant.
Results
A total of 59 patients were enrolled (25 boys, 34 girls). No patient experienced immediate postoperative complications, such as active bleeding, wound dehiscence, or airway problems such as asphyxia or pneumonia. No patient required a blood transfusion. Of the cases, 45 (76.3%) were mild clefts that involved soft and/or hard palate, and 14 (23.7%) were severe clefts involving up to the alveolus or lip. Among the 14 severe clefts, 12 were male patients. Relaxing incisions were performed in 18 cases (30.5%), whereas in 41 cases (69.5%) wound closure was possible without additional techniques. The mean measured blood loss volume was 16.61 mL (± 10.33 mL). Among these categorical independent variables, male sex, severe cleft type, Veau type III and IV, and the use of relaxing incision were significantly associated with increased blood loss (Table 1). Patients who had all of the risk factors for increased blood loss (male sex, severe cleft type, and additional relaxing incisions) revealed greater bleeding of 27.56 mL (± 13.86 mL) when compared with the blood loss of 11.14 mL (± 7.08 mL) in patients who did not have any risk factors (P = .02).
The Relationship Between Categorical Variables and the Amount of Bleeding
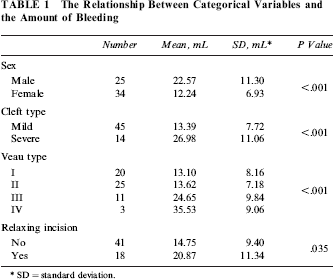
SD = standard deviation.
The mean age at the time of operation was 13.71 ± 4.05 months, and the mean weight was 9.91 ± 0.88 kg. The palatal gap was 6.69 ± 2.97 mm, and the mean operation time was 78.47 ± 39.47 minutes. Preoperatively measured hemoglobin was 12.29 ± 0.67 g/dL, whereas 3 days postoperatively it was decreased to 11.35 ± 0.60 g/dL. Similarly, hematocrit was reduced from 36.36 ± 1.74% to 34.32 ± 2.00%. Although the decreases in hemoglobin and hematocrit were significant (P < .001) at 3 days postoperatively by paired t test, there was no significant relationship between blood loss and change in hemoglobin or hematocrit.
Scatterplots showed a relationship between blood loss and the measured numeric variables (Fig. 1). The correlation analysis revealed that age, palatal gap, and operation time were significantly associated with blood loss (Table 2). The multiple linear regression analysis revealed that the amount of intraoperative bleeding could be assessed as follows:
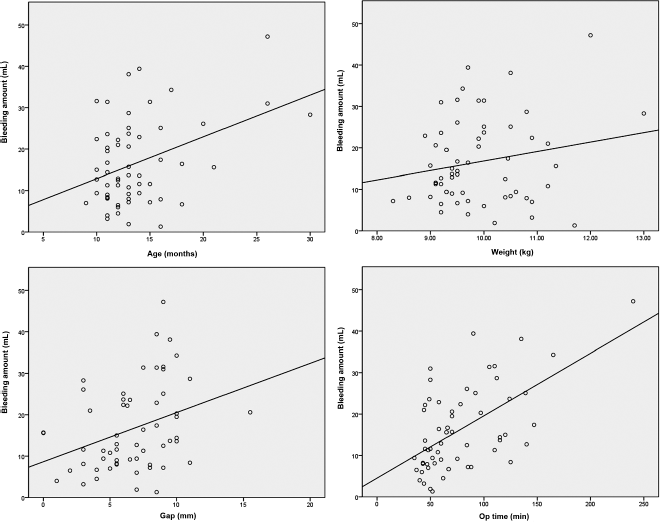
Scatterplots showing the relationship between blood loss and numeric variables.
Pearson Correlation Analysis Between Numeric Variables and the Amount of Bleeding
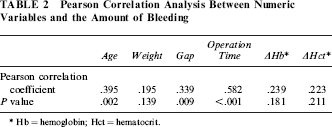
Hb = hemoglobin; Hct = hematocrit.
Discussion
Clinical studies of cleft palate have focused on comparing the long-term surgical outcomes among various operative techniques in terms of fistulae, speech, or growth of the jaw (Ross, 1987; Koh et al., 2009; Hardwicke et al., 2014; Timbang et al., 2014). However, although early correction of cleft palate has become a general trend, few studies have been investigated the safety of palatoplasty. As a first step in investigating the safety, we evaluated intraoperative blood loss during DOZ palatoplasty.
Previous reports have used various indirect methods to estimate blood loss during surgery, such as colorimetry or the osmolality dilution technique (Evelyn and Malloy, 1938; Kaplan, 1978; Daabiss, 2009). However, these indirect methods are not intuitive, and they are usually used in estimating larger blood loss. They are not reliable for estimating the relatively small volume of blood lost in cleft palate surgery. Herbert et al. (1990) developed more intuitive methods for assessing blood loss in cleft surgery. However, the single suction system they adopted can be contaminated by betadine solution or secretion from saliva.
We adopted a dual suction system in which one system was used for blood and the other for the antiseptic or saliva. A closed suction system from the open air prevented blood loss from dehydration. The blood volume of the suction bottle was estimated by calculating perioperative weight change. The average density of human blood is known to be approximately 1,060 kg/m3, very close to that of pure water (Cutnell and Johnson, 1998). Therefore, the change of the suction bottle weight in milligrams can be converted to the same amount of volume in milliliters. The weight change of the suction line was measured to assess the blood trapped in the suction line using the same method. In the aforementioned study by Herbert et al. (1990), a suction tube 3-m long with a 5-mm internal diameter was used. They reported that around 5 mL of blood was trapped in the suction tube. However, a suction line of standardized size is not always available. We used gauze balls to swab blood from the operative field, and the weight change of the gauze balls was considered to be the bleeding amount. Keenan et al. (1998) investigated the accuracy of measuring swab weight and concluded that accuracy increases in proportion to the swab weight. They also showed that the weight of the swab reduced to approximately two-thirds of its initial weight when exposed to the open air for 1 hour. Therefore, we attempted to use the gauze balls until they were thoroughly soaked with blood to increase accuracy. Soaked gauze balls were wrapped in a plastic bag to minimize weight loss from open air exposure.
Previous studies investigating the blood loss during palatoplasty have shown variable results, ranging from 7.2 to 82.0 mL (Dingman et al., 1949; Mladick et al., 1967; Moore et al., 1988; Senders and Sykes, 1995; Kane et al., 2000). These studies did not report detailed methods for measuring blood loss, and the descriptions of cleft type and surgical methods were not clear. Many surgeons performed various surgical methods, so achieving consistent information was difficult. On the contrary, in our study a single surgeon (S.K.) performed only the DOZ technique. We also categorized patient-related factors to investigate their correlations with blood loss.
The mean blood loss was 16.61 ± 10.33 mL, relatively smaller than that previously reported. This discrepancy is thought to be a result of waiting a sufficient amount of time for the epinephrine to take effect and the surgical skill minimizing the dissection area. According to pediatric transfusion guidelines, blood loss less than 15% of the total blood volume does not require any specific transfusion (Liumbruno et al., 2011). In the current study, there was blood loss of approximately 5% of the total blood volume, which represents a low risk for transfusion. In male patients, the bleeding amount was larger than that in the female patients, which may be explained by the greater incidence of the severe cleft type in male patients. Older patients showed a tendency toward increased blood loss, perhaps because of the more developed musculature.
The hemoglobin and hematocrit were significantly decreased at 3 days postoperatively, but we could not find any significant relationship between blood loss and change in hemoglobin or hematocrit. The relatively small amount of blood lost and postoperative fluid intake could account for this. We performed a complete blood count at 3 days postoperatively because it is known that after a sudden single blood loss, hematocrit gradually falls during the 2 to 3 days following reninangiotensin-aldosterone system activation to restore fluids (Hillman, 1995).
There are several limitations of the present study. The relatively small sample size, especially of the severe cleft type, is one of the weak points. Although we made every effort to measure blood volume as accurately as possible, insensible loss and blood stained on the surgical instruments or gloves can cause the real blood loss to be underestimated. We were unable to measure postoperative bleeding through the nasal and oral cavities because of technical difficulties. In addition, the volume of injected epinephrine and the depth of anesthesia could also be confounding factors. We only performed DOZ; therefore, blood loss in other palatoplasty techniques should be investigated in the future studies.
Our results suggest that the DOZ procedure is relatively safe in terms of intraoperative bleeding. Bleeding amount tended to increase in older male patients with a severe cleft and a larger palatal gap. Palatoplasty at an earlier age and the shortening of overall operation time can contribute to minimizing blood loss.
Footnotes
Acknowledgments
The authors appreciate the statistical analysis from the Medical Research Collaborating Center at the Seoul National University Hospital and the Seoul National University College of Medicine.
There is no source of funding to declare.