
Abstract

Vyas RM, Kim DC, Padwa BL, Mulliken JB. Primary premaxillary setback and repair of bilateral complete cleft lip: indications, technique, and outcomes. Cleft Palate Craniofac J. 2016:53:302-308.
We read with interest the paper written by Vyas et al. (2016) evaluating the outcome of primary premaxilla setback in cases with complete bilateral cleft lip with or without cleft palate. Indications for the primary premaxilla setback were failed active preoperative orthopedics, late referral for orthopedic treatment, or in cases with intact palate. It is interesting to see an old controversial topic still under discussion and, perhaps, more interesting are the encouraging results in their limited patient series.
However, the historical reference omits key stages in the evolution of the premaxilla setback. The authors gave credit to Banderleben (1865) for the introduction of the premaxilla setback, which is not fully correct. The seminal work about the premaxilla setback procedure is attributed to von Bruns (1857), who first provided a detailed drawing proposing a vomer/septal wedge excision posterior to the premaxilla, published in von Brun's Surgical Atlas (Fig. 1); subsequently, to the best of our knowledge, this drawing has never been reprinted before. In a corresponding textbook to the atlas, Handbuch der praktischen Chirurgie (Textbook of Practical Surgery), he revised single cases published on premaxilla setback from France (Blandin, 1843; Verneuil, 1856; Debrou, 1844, among others) and Germany (Mayer, 1856). Von Bruns informed about the terrible results after premaxilla resection, routinely performed until the first half of the 19th century. He also discussed extraoral orthopedic forces on a prominent premaxilla that produce septal distortion, and he encouraged his peers to perform the premaxilla setback procedure as reliable and safe but calling for further refinements. Bardeleben, professor of surgery in Greifswald and Berlin, edited a four-volume textbook set titled Lehrbuch der Chirurgie und Operationslehre (Textbook of Surgery and Surgical Techniques). A translation of the French textbook, Vidal's Traité de Pathologie Externe et de Medicine Operatoire (Vidal's Treatise of External Pathology and Medical Preoperative Medicine) into German is included in Vol. 3. Bardeleben provided a brief historical review about the evolution of the premaxilla setback procedure, which he continuously updated (1852-1882). In the 6th edition, published in 1871, Bardeleben proposed a vertical vomer/ septal incision via a subperiostal approach as shown in the Figure (line e-f); the author did not provide an original drawing. The procedure was previously published by his fellow, Dr. Ostertag, as a doctoral thesis presented in Geifswald in 1868. Bardeleben gave credit to von Bruns for his contributions to the understanding of the premaxilla and septal vascularization. Von Esmarch and Kowalzig (1892) mentioned the setback procedure according to Bardeleben, providing a drawing authored by Kowalzig (medical illustrator and fellow of von Esmarch), the original illustration by von Bruns with his contributions omitted. Subsequently, the illustration by Kowalzig was reprinted by others (Joseph, 1931; Millard, 1977), and the contribution by von Bruns was not mentioned thereafter.
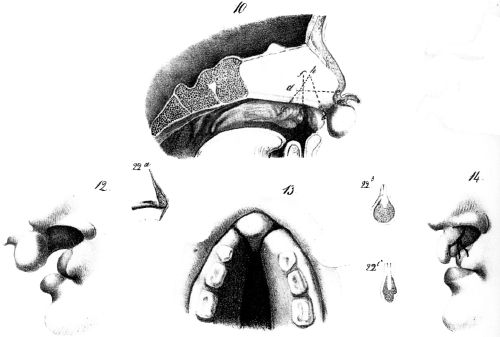
Premaxilla setback procedure as described by Victor von Bruns in the Surgical Atlas [in German] in 1857. Translated from German (marked 10): “Sagittal view of septal cartilage with prominent premaxilla in double cleft lip and palate. Dotted lines denote incision line as described in v. Bruns (1859). The drawing was taken from an infant aged 3 months in an almost original dimension.” Von Bruns stated that the more convenient line of incision is vertical, producing a wedge, as demonstrated in the figure (line g-h-b). A vertical line (f-e; no wedge incision) should be avoided, septal cartilage overlap is obtained, and no stable healing is expected. The horizontal line (c-d) should be avoided since the premaxilla segment is not stable and the vascularization is not appropriate. Profile view preoperative (left, marked 12); repositioned premaxilla in occlusal view 6 years after surgery (below middle, marked 13); profile view postoperative with suture in place (right, marked 14). Small drawing (marked 22a) shows the excised vomer/septal wedge with reflected mucosa. The drawing marked 22b denotes a coronal view of resected wedge in the anterior osteotomy (proximal); the drawing marked 22c denotes the coronal view of resected wedge posterior (distal; drawings 22a-c correspond to a different patient who underwent premaxilla setback); four drawings taken from the original, Plate #VIII/ (48.5 cm × 33.3 cm) in von Bruns, 1857. The plate includes 37 drawings, each drawing sized 6 cm X 4.5 cm. Reprinted with permission: Mohr Siebeck, Tuebingen, Germany.
Nevertheless, the current preferred procedure for the premaxilla setback is based on a vomer resection, as advised by von Bruns, and not as a vertical osteotomy producing a sliding retrusion of the mobile osteotomized premaxillary segment, as proposed by Bardeleben. The main contribution of Bardeleben was the subperioteal approach to the vomer, as mentioned by Millard (1977).
Footnotes
Disclosures: None of the authors has a financial interest in any of the products, devices, or drugs mentioned in this manuscript.