
Abstract

The gap between the worlds of nursing education and nurses in practice has been highlighted over the past four decades. Cyclical efforts to bridge this gap have met with varying degrees of success. A recent attempt to unite nursing education and practice is the Quality and Safety Education for Nurses (QSEN) initiative, generously funded by the Robert Wood Johnson Foundation (Cronenwett et al., 2007). The major goal of QSEN is to prepare future nurses with the knowledge, skills, and attitudes necessary to continuously improve the quality and safety of care delivery in health care systems. This article summarizes and discusses QSEN's accomplishments and upcoming activities within a framework of the factors contributing to the separation of the education and practice worlds and makes recommendations for building on the progress derived from QSEN activities.
Historical Perspectives
The early days of nursing education relied on an apprentice model of education. Diploma nursing programs were created by hospitals, with instructors selected for their excellent performance and clinical skills. Most instructors continued to practice, thus ensuring the currency of their knowledge. Nursing students received limited formal instruction and spent many hours working in the wards. Close supervision of new students (often called “probies,” short for “probationers”) was a serious undertaking to protect patients and to instill the necessary values related to nursing practice. As students progressed, they assumed more responsibilities and eventually served as charge nurses. As new graduate registered nurses, these individuals were fully prepared and had in fact “practiced” in the role for some period of time. For better or worse, there were few surprises in the demands and expectations of the workplace.
Several factors led to the migration of nursing programs into colleges in the United States. Support for Florence Nightingale's vision of nursing as a true profession grew steadily, along with the body of knowledge associated with the practice of medicine. The amount and variety of knowledge required by nurses expanded significantly. In 1923 the Goldmark Report recommended that nursing education should reside within institutions of higher education. Over time, many U.S. diploma programs transitioned into colleges or were closed in response to professional nursing organizations ‘position statements and goals. However, the financial contribution that hospital-based nursing schools made to their institutions (a factor that continues today) was a significant disincentive to closing these programs.
The major goal of QSEN is to prepare future nurses with the knowledge, skills, and attitudes necessary to continuously improve the quality and safety of care delivery in health care systems.
Origin of the Education-Practice GAP
The movement of nursing education into college settings accomplished many goals established by nurse leaders and other stakeholders. Nursing education incorporated liberal arts, science, and social science knowledge taught by experts in those fields, providing a firm foundation for professional nursing practice. Exposure to other professional disciplines and the value of generating and applying new knowledge to improve practice were emphasized. Nurse faculties strengthened their educational credentials and methods to enhance the academic experience and to produce professional nurses with a commitment to lifelong learning and to expanding scientific knowledge within the discipline.
The unanticipated consequences of nursing education's transition into colleges are at the core of the education-practice gap. With most nursing faculty no longer employed in health care facilities, access to appropriate practice experiences to maintain current knowledge and skills was lost. The nature of nursing practice makes it difficult to be involved intermittently. Increasing technology, complex health care systems and practices, cost implications, and risk management considerations further complicate faculty practice arrangements. Many nursing instructors find it challenging to balance their full-time roles as academicians with the need for ongoing clinical exposure; some have described this challenge as having two full-time positions! Although clinical supervision of students helps some faculty stay connected to practice, they often describe the experience as being a visitor in rather than a member of a health care organization.
Clinical rotations provide the learning laboratory in which cognitive, psychomotor, and affective skills as well as professional values are synthesized into desired nursing practice competencies. The typical college nursing program includes a day or two a week of clinical experiences over a 2- to 3-year period that may or may not include summer terms. Over time, the practice of having students rotate to many clinical sites to be exposed to different types of patients and facilities evolved, with students spending as little as 2 or 3 weeks in one location. This approach prevented students from gaining a realistic sense of the pattern of nursing work, experiencing meaningful interactions with other members of the health care team, or developing an understanding of patients ‘trajectories of care.
Beginning with early research on the concept of reality shock (Kramer, 1974) through more recent evidence-based approaches to transitioning new graduate nurses into practice (Goode, Lynn, Krsek, & Bednash, 2009), programs have been designed to promote a graduated introduction to the realities of the professional nurse role. Two strategies in use today are extended orientation programs and graduate nurse internships. In summary, the challenges of nursing faculty engagement with contemporary clinical practice and the patterns of student involvement in clinical learning venues are two major factors in the education-practice gap.
The QSEN Initiative: An Overview
The late 1990s found an increasing focus on the need to improve the quality and safety of health care delivery. A series of reports issued by the Institute of Medicine (IOM, 2003) generated the most attention, especially the statistic that more than 98, 000 lives per year were lost in the United States from medical errors. Efforts to enhance quality and safety in practice settings led to dramatic changes in the practice of nursing, medicine, and other health disciplines. Specifically, quality improvement and safety analysis techniques borrowed from cutting-edge industry practices (especially aviation) became standard expectations for practitioner performance.
As the nursing practice environment embraced this focus on quality and safety with its attendant new skills, it became clear that graduating nursing students were missing critical competencies. A group of nursing educators led by Dr. Linda Cronenwett and Dr. Gwen Sherwood of the University of North Carolina at Chapel Hill developed a proposal to better prepare nursing graduates for the realities of the practice environment and submitted it to the Robert Wood Johnson Foundation. The result was QSEN, a major national initiative centered on patient safety and quality topics. A team of faculty experts and a cadre of pedagogical leaders, along with an interprofessional advisory board, collaborated to accomplish the project goals. QSEN's primary goal was to address the challenge of preparing future nurses with the knowledge, skills and attitudes (KSAs) necessary to continuously improve the quality and safety of the health care systems in which they work (Cronenwett et al., 2007). The QSEN project consists of three phases.
Clinical rotations provide the learning laboratory in which cognitive, psychomotor, and affective skills as well as professional values are synthesized into desired nursing practice competencies.
Qsen Phase I: Defining Competencies
Phase I of QSEN sought to clearly define quality and safety competencies for prelicensure (and later for graduate level) nursing students using an adapted version of the IOM competencies. The prelicensure QSEN competencies along with their respective definitions are listed in Table 1.
Quality and Safety Education for Nurses Competencies and Definitions
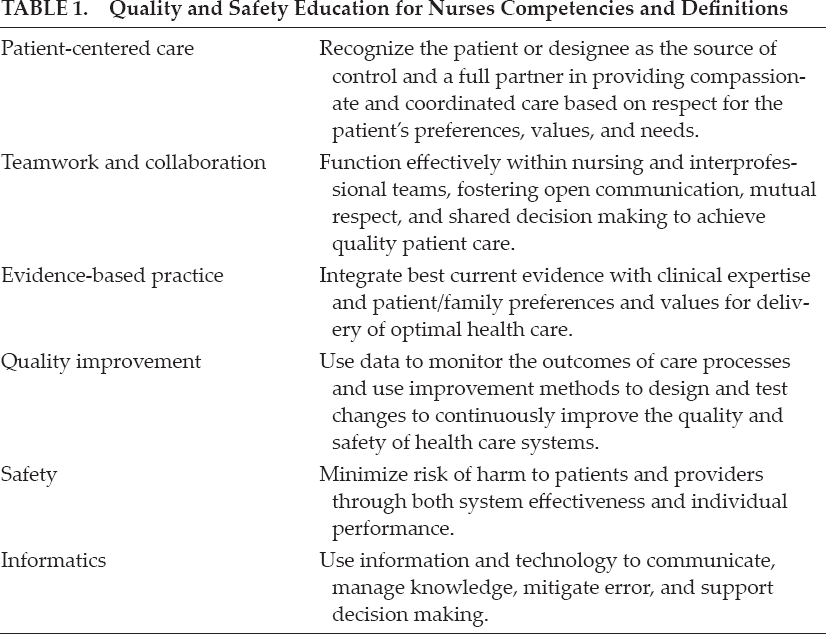
Each QSEN competency was further explicated through statements regarding KSAs that should be developed during prelicensure nursing education programs (Cronenwett et al., 2007). Graduate nursing competencies, finalized with the input and endorsement of major advanced practice specialty organizations, have been recently published (Cronenwett Sherwood, Pohl, et al., 2009).
During phase I, a descriptive study using survey methodology documented the current state of prelicensure nursing education with respect to the six QSEN competencies (Smith, Cronenwett, & Sherwood, 2007). Member schools (n = 572) of the American Association of Colleges of Nursing (AACN), plus a convenience sample of all associate degree nursing programs in North Carolina, were surveyed. The response rate was 30% for AACN schools and 40% for associate degree programs. More than 95% of respondents indicated that content related to QSEN competencies was included in their curricula, with 10% to 18% reporting dedicated courses. Quality improvement and informatics content were least often included, while patient-centered care and safety were most often included. However, follow-up focus groups suggested that there were significant differences in how faculty defined these concepts versus the definitions promulgated by QSEN. Many faculty members indicated that their ability to teach content using the QSEN definitions was lower than initially reported because of their lack of familiarity with current use in practice settings. Ratings of faculty expertise in teaching quality and safety content were lowest for evidence-based practice, informatics, and quality improvement. The most popular teaching-learning strategies (in descending frequency) were lecture, clinical experience, and readings. Simulation was used less frequently than all other pedagogical strategies except return demonstration.
Qsen Phase Ii: Teaching Tools and a Learning Collaborative
Phase II of QSEN focused on identification and sharing of effective teaching tools for quality and safety topics via a comprehensive Web site (http://www.qsen.org) begun in phase I. Additionally, 15 pilot schools of nursing across the country were selected to participate in the QSEN Learning Collaborative. Participating schools designed and implemented curricular innovations reflecting quality and safety content, sharing methods and materials, and lessons learned (Cronenwett Sherwood, & Gelmon, 2009). Two of the sample schools were associate degree programs, one of which spanned five campuses and is counted as one program for the purposes of this study. Fourteen were BSN programs, and one was a diploma school of nursing. The sample schools are located in 14 different states.
Part of the assessment of the QSEN Learning Collaborative was an evaluation of graduating student's perceptions of quality and safety content and competencies in their nursing programs. Published reports of nursing student skills related to QSEN competencies were very limited and tended to focus on informatics and evidence-based practice (Sullivan, Hirst, & Cronenwett, 2009). The QSEN Student Evaluation Survey (SES) consisted of three primary questions related to KSAs:
Knowledge: Rating whether quality and safety content was covered in the curriculum
Skills: Self-reported level of preparedness to perform quality and safety actions and skills
Attitudes: Perceived importance of the quality and safety actions and skills
The SES was e-mailed to 1, 665 students from QSEN Learning Collaborative schools and two additional universities. A total of 575 students completed the SES, a response rate of 35%.
Knowledge
The most frequently included content in the curricula belonged to three of the six competencies: patient-centered care, safety, and evidence-based practice. In contrast, the least frequently or not included content areas were from the quality improvement, teamwork, and collaboration competencies. Teaching-learning techniques employed were (from most to least frequent) classroom, course assignments/readings, clinical experience, and lab/simulation. Collectively, these results are similar to findings from the quality and safety curriculum program survey of prelicensure program leaders reported by Smith et al. (2006).
Skills
Students were asked to report their preparedness to perform a list of 22 actions or skills representing the six QSEN competency subscales, with higher scores indicating perceptions of being better prepared. Generally, students from all schools felt somewhat or very prepared to perform actions representing each of the six competencies. Respondents felt most prepared for skills related to patient-centered care and informatics and least prepared for skills related to evidence-based practice and quality improvement.
Attitudes
Students were asked to rate the importance of the 22 quality and safety skill items as a proxy for their attitudes regarding quality and safety competencies. Respondents said that the most important skills for new nurses were in the areas of patient-centered care and least important in evidence-based practice and quality improvement; however, safety was seen as the second most important competency versus informatics in the skill preparedness questions. Graduating students expressed strong support for the importance and value of the QSEN competencies in their professional nursing practice; in many cases the reported importance ratings exceeded self-reported levels of preparedness.
Respondents said that the most important skills for new nurses were in the areas of patient-centered care.
An interesting survey result was that 66% of the students reported having patient care experience outside their nursing education programs. This experience was associated with higher self-rated performance in selected QSEN competencies. Students expressed their perceptions of the gap between theoretical classroom content and the realities of clinical practice and also commented that more clinical time should have been included in their programs.
Qsen Phase Iii: Faculty Preparation and a National Safety Forum
The third phase of QSEN consists of two major activities. The AACN launched the QSEN Education Consortium to prepare nurse faculty to lead curricular change related to quality and safety derived from earlier QSEN work. A series of faculty development workshops will be held around the country over the next 2 years supported by QSEN experts on the original team and leaders from the QSEN Learning Collaborative schools, among others. Robert Wood Johnson Foundation funding will partially support faculty attendees.
The University of North Carolina team will convene a national safety forum in June 2010, promoting a focus on quality and safety in nursing education to foster sharing of innovative approaches and assessment results. Additionally, a focus on instructional materials that provide quality and safety as the framework for professional practice is in process.
Possibilities for Bridging the Education-Practice GAP
The lessons learned from the QSEN initiative have great potential for helping bridge the nursing education-practice gap. Among the most promising are redesigning curricula using the QSEN framework, reconfiguring clinical experiences to promote recognition and practice of QSEN competencies, assessing cognitive and affective learning outcomes, enhancing faculty's ability to teach QSEN-related content within contemporary scenarios, and recommitting to innovative and realistic ways to engage faculty in clinical practice.
Through the QSEN Learning Collaborative and other examples of curricular change, it is clear that faculty, students, and practicing nurses can easily relate to content organized using the QSEN competencies as a framework. Reading, discussions, simulations, and clinical activities focused on quality and safety topics have proven to be powerful tools in joining students with practicing nurses.
There is increasing data to suggest that current methods of clinical exposure for students are not promoting the best experiences. A strong theme of the need to translate theoretical information into practice emerged from the student survey. How can we harness the rich learning about quality and safety that students found so valuable? Would clinical intensives or immersions create better outcomes related to the QSEN competencies? To professional roles, values, and self-concept? In other areas? And wouldn't it be wonderful if newer clinical experience approaches consumed fewer resources (for schools and for health care organizations) so that savings could be redeployed into value-added activities instead of administrative processes?
If learning is expected in areas that students or practicing nurses do not believe are highly relevant, it is unlikely that those topics will be valued and embraced for the long term.
Assessment of cognitive and affective learning outcomes will generate important data to guide more effective teaching-learning strategies. If learning is expected in areas that students or practicing nurses do not believe are highly relevant, it is unlikely that those topics will be valued and embraced for the long term. On the other hand, with a data-driven approach that includes evidence-based practice and related learning activities, we can adjust our focus and techniques to achieve desired outcomes. For example, if students do not appreciate the role of handoffs in quality of care, how likely are they to embrace practices that have been shown to improve this activity?
Practicing staff welcome the informed perspectives that faculty and students offer to more creatively frame or solve care issues.
Enhancing faculty's ability to teach QSEN-related content within contemporary scenarios is a win for all major stakeholders. Student comments on the SES clearly showed their level of connection to faculty who related QSEN to all learning venues (classroom, reading, lab, and clinical). Practicing staff welcome the informed perspectives that faculty and students offer to more creatively frame or solve care issues. And faculty themselves will feel more confident when they have recognized expertise in the QSEN competencies, especially related to evidence-based practice and quality improvement. However, achieving this will require faculty to be meaningfully involved in clinical settings.
We must recommit to identifying innovative yet realistic ways to engage faculty in clinical practice activities. Continuity of sites for clinical supervision promotes increased knowledge of the health care organizations and their practices, improved opportunities to develop relationships, and the real potential for academic partners to collaborate to improve important aspects of clinical care.
In summary, QSEN has provided rich learning about how the nursing education-practice gap may be bridged. While a survey of graduating students indicated that they felt relatively prepared to perform QSEN competencies and believed that these competencies were important to their practice, there were specific topics where improvement or less variation would be highly desirable. Enhancing faculty expertise in QSEN content and reconfiguring clinical experiences could contribute to strong education-practice partnerships that will benefit all.
Footnotes
Dori Taylor Sullivan, PhD, RN, NE-BC, CNL, CPHQ, is associate dean for academic affairs at Duke University School of Nursing in Durham, North Carolina.