
Abstract
Through a collaborative partnership with administrators at a university, nurse leaders at a local hospital worked to create a culture in which nurses could provide evidence-based practice (EBP). The Best Practice Series was started, and two participants ‘experiences of implementing EBP in their units are described with encouraging results.
All professionals are called to work together to solve health care issues and provide quality care. One issue is having enough nurses, and one strategy to promote quality care is creating a culture of evidence-based practice (EBP). Building a culture of EBP requires administrative support and buy-in from those expected to implement the evidence-based interventions (Ogiehor-Enoma, Taqueban, & Anosike, 2010). John Peter Smith Health Network (JPS) nurse leaders in Fort Worth, Texas were interested in hiring qualified nurses for positions in a new unit and creating a culture of EBP. Through a collaborative partnership with administrators at Harris College of Nursing & Health Sciences at Texas Christian University (TCU), the needs of both institutions were met. A qualified registered nurse (RN) was provided by JPS to teach a TCU clinical group of nursing students at JPS. A doctorally (PhD) prepared research consultant was provided by TCU to meet the health network's EBP goals.
Best Practice Series
The consultant led a series of breakout sessions called the Best Practice Series during monthly shared governance council meetings. This series was open to those interested in learning about evidence to support and guide their practice (see Table 1). Participation at the start of each year was large and dwindled over time to a consistent group of five. A strong relationship developed between the consultant and the four nurses and one librarian. They acknowledged the consultant's enthusiastic support, listening skills, and nonthreatening nature. The participants were willing, eager action takers who valued EBP. Two participants ‘experiences of implementing EBP in their units are described in the following sections.
Best Practice Series
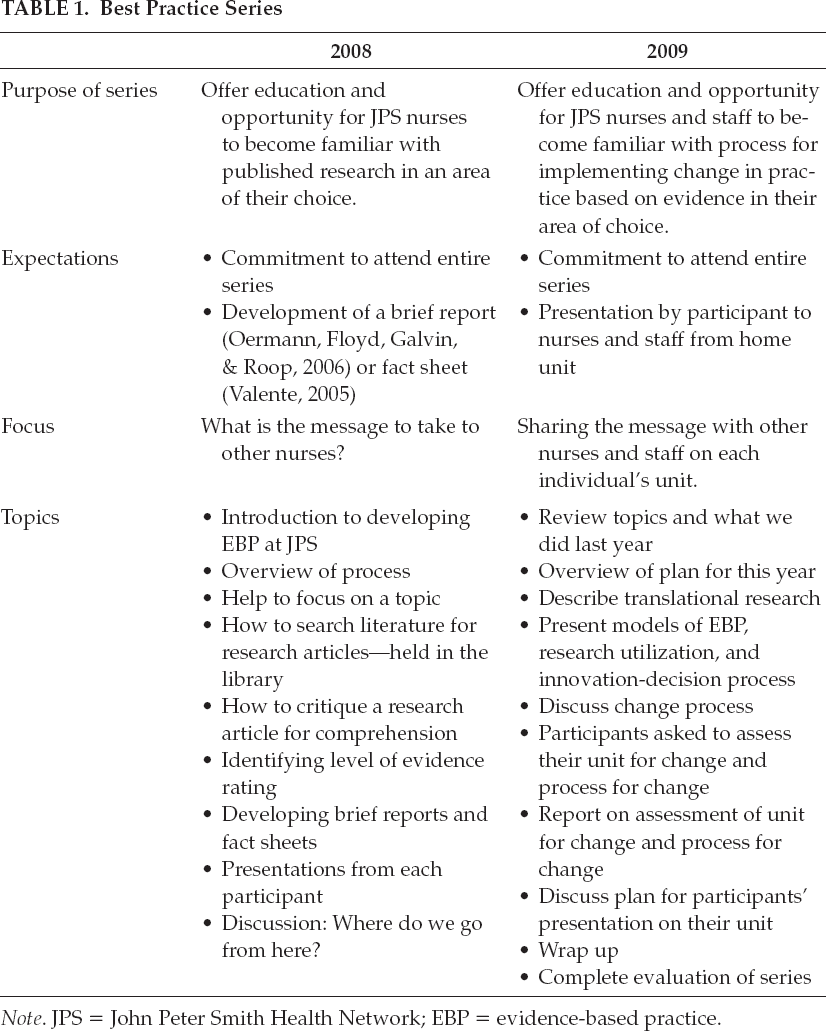
Note. JPS = John Peter Smith Health Network; EBP = evidence-based practice.
Department Supervisor in Psychiatry
The department of psychiatry embarked on a performance improvement journey in January 2007 called Psychiatric Project Prevention (P3). This project focused on abolishing the use of seclusion and restraint, thereby preventing injury to patients and staff. Implementing this project was the dream of the department supervisor. Through a review of the literature and networking with national contacts, she determined that legislative, accrediting, and paying entities would eventually mandate discontinuance of seclusion and restraints as an intervention in the psychiatric area; thus the time was right to begin the project.
The supervisor recognized the need for buy-in by people around her who would bring about this practice change (or not) by their actions. She sought and obtained the support of hospital leaders. Through networking, she also acquired the support of psychiatric technicians, nurses, a psychologist, and physicians (attending and resident).
The last Wednesday of each month at noon was selected for staff education and processing for the P3 Project. Administrators agreed to pay one hour of education time to any off-duty staff attending, and lunch was provided to encourage attendance. The supervisor cared for the staff by structuring the sessions with ground rules and a time frame. Ground rules included starting and concluding on time, encouraging the free expression of views and perceptions of an event without fear, and respecting each person by listening. The first 15 minutes of each session was for attendees to discuss their past month's reality. Once trust was established, sharing became less scary. The key topic of education was presented in the next 40 minutes. Answering questions and/or forming subgroups for further work took the last five minutes of the hour-long session.
Staff were asked to commit to attending ten out of twelve sessions a year. Managers and supervisors were expected to attend the education sessions, thus demonstrating their support. The supervisor set the tone for building relationships by communicating prior to and at the first session that each person has value, is included, and belongs. Invitations with the inscription “Cast from shackles which bound them, this bell shall ring out hope for the mentally ill and victory over mental illness” (Mental Health America, 2011) were sent to the staff and the Chief Nursing Officer. A name card, workbook, and multicolored paper keys with the numbers one, two, and three were made for each attendee and placed on the table. The message on the front of the workbooks communicated, “Let us decide on our destination and let us chart the course.” On their paper keys, attendees were asked to write three tools they would add to their toolkit to take away. Orange ribbons and pens stating “P3 Ambassador” were given to attendees, who were asked to wear the ribbons on their name badges. The ribbons and pens served as advertisements and reminders of the charted course—to eliminate the use of seclusion and restraint in the psychiatric area.
The success of the P3 program was in the people. It started with the supervisor's vision of changing the culture. She ignited interest in the journey with her passion, enthusiasm, dedication, cheerleading, and encouragement. Her strength was her faith in God throughout the entire process. Support was gained from the department leaders and hospital administrators next. Then, the people were mobilized to act. The staff in the psychiatric area were provided information, time to address issues, compensation to attend the education sessions, reminders of their goal (ribbons and pens), and a lunch incentive. The supervisor used the knowledge and experience she gained from the Best Practice Series to support and strengthen what was already underway. She reminded staff that the whole P3 program was grounded in the evidence.
The outcome is a staff from all disciplines committed to providing a safe and truly therapeutic environment. They are dedicated to the abolition of the use of seclusion and restraint in the psychiatric department. The numbers demonstrate the overwhelming outcome. Comparing the data collected from October 2008 to August 2009 (after implementation of the P3 program in January 2007) to October 2005 to August 2006 (prior to implementation), the number of restraint events was reduced by 68% and the number of seclusions decreased by 45%. These significant decreases are viewed in relation to the increasing numbers of people served in the department of psychiatry (includes the psychiatric emergency center, adult inpatient unit, and the adolescent inpatient unit).
Reviewing the literature, the PACU RN discovered that a local anesthetic administered before hand/wrist surgery reduced postoperative pain, thus making it easier to control with as-needed narcotics.
Staff Rn in the Postanesthesia Care Unit
While attending the Best Practice Series, a staff RN in the postanesthesia care unit (PACU) discovered evidence in relation to a clinical situation she witnessed. Many hand/wrist surgery patients complained of incredible postoperative pain not relieved by narcotics. Reviewing the literature, the RN discovered that a local anesthetic administered before surgery reduced postoperative pain, thus making it easier to control with as-needed narcotics. The challenge she encountered was obtaining buy-in from the surgeon who performed many of these cases. The following is her story and how she persevered to develop a relationship with the surgeon and the incredible outcome achieved.
This RN of 17 years remembers hearing in nursing school that “being pain-free helps the healing process.” Her passion to comfort her patients with pain relief and emotional support is a big part of what she does. She sees herself as a patient advocate.
About four years ago, she noticed an influx of patients undergoing carpal tunnel and other hand/wrist surgery. These patients did not receive any local anesthetic, which is different than common practice of giving local anesthetic in some facilities. As soon as they woke up, they were usually crying with pain. The PACU nurses found themselves giving large doses of intravenous narcotics to this patient population, and most of the patients stated that the medicine did nothing for the pain. Some patients stated that they had had this surgery before and never remembered this degree of pain. The patient satisfaction scores concerning pain control were not satisfactory. This staff RN decided that it was time to speak with the surgeon. After dealing with four patients crying from uncontrolled pain, she went to doctor's lounge to convey her concerns. She found the surgeon sitting at the computer, politely introduced herself, and explained her reason for speaking with him. She called him “sir” and stated that over the last few months, she had noticed his patients having uncontrolled pain after carpal tunnel surgery in particular.
She explained that the nurses had been giving large amounts of narcotics to try to control the pain, without success, and added that she noticed he did not use a local anesthetic for carpal tunnel surgery. He explained that patients who cannot feel their hand may burn themselves badly and not even know it. She calmly thanked him for his time, but after thinking about it, she became very concerned that he would not consider local anesthesia—he did not have to deal with the patients ‘crying with pain. As a patient advocate, she began to examine the evidence regarding this issue.
While gathering evidence and dealing with patients ‘uncontrolled pain, she started developing a relationship with this surgeon. Every time he came to the PACU, they talked about topics unrelated to patients. They discovered they shared a birthday and both had season tickets to the Dallas Cowboys with their seats only two rows apart. He would find her to share a joke every week. Over time they developed an excellent working relationship.
One day an unexpected shift occurred. A patient with a history of chronic pain presented for carpal tunnel surgery. The surgical team discussed what would benefit this particular patient and decided to give a local anesthetic. Following surgery, the RN thanked the surgeon for making a major difference in this patient's surgical experience. She decided to show him. When they arrived at the bedside, the patient talked about how fast the surgery was and how she was not hurting badly. Neurovascular checks revealed that the patient had good sensation in her arm and hand. When the next patient, who had not received local anesthesia, came to the recovery room, the RN showed the surgeon that patient's reaction. From that time, the surgeon started ordering preoperative local anesthetic for more, but not all of his patients.
People, support, relationships, and passion are the key ingredients in a recipe for success when implementing evidence-based nursing practice.
Building a relationship with the surgeon played a huge part in the success of this RN's patients ‘pain being controlled. She shared the evidence with him and his residents, and all have been able to discuss options for pain control for the patients. She truly believes she made a difference, one patient at a time, and carried out JPS ‘mission, “To improve the health status of the families and individuals in the communities we serve.”
Conclusions
People, support, relationships, and passion are the key ingredients in a recipe for success when implementing evidence-based nursing practice. People are the only ones who can bring about a change in practice. Support from nurse leaders in administration is necessary for a successful program. EBP has a better chance of transforming the culture if relationships are built with those who are asked to change their thinking, attitudes, and/or behavior. Passion is the energy driving the perseverance to implement EBP and thereby change culture.
Footnotes
Acknowledgment.
The authors thank Elaine Evans, PhD, RN, for the review of this manuscript.
Susan M. Rugari, PhD, RN, CNS, was assistant professor at Harris College of Nursing & Health Sciences at Texas Christian University and research consultant at John Peter Smith Health Network (JPS) in Fort Worth, Texas. She is currently associate professor in the Department of Nursing at Tarleton State University in Stephenville, Texas.
Lynette Alcorn, BSN, RN, is a staff RN in the Post Anesthesia Care Unit at JPS Diagnostic and Surgery Hospital of Arlington in Arlington, Texas.
Theresa Baird, MBA, RN, is nursing administration manager at JPS Health Network in Fort Worth, Texas.
Basnot E. Phillips-Williams, RNC, is department supervisor in the Department of Psychiatry at JPS Health Network, Trinity Springs Pavilion, in Fort Worth, Texas.
Wendy F. Spagnuolo, MLS, is clinical medical librarian at JPS Health Network in Fort Worth, Texas.
Mei-Yi Lee, MSN, RN, P/MH CNS-BC, is house supervisor and clinical nurse specialist in the Department of Psychiatry at JPS Health Network in Fort Worth, Texas.
Pamela A. Berglund, RN, BC, CCE, is a nurse educator in health promotion at JPS Health Network in Fort Worth, Texas.