
Abstract
The significance of good clinical reasoning skills relates to prevention of adverse patient outcomes from failure to diagnose problems, institute appropriate treatments, and/or manage complications. The clinical reasoning pedagogies described in this article are integrated across a baccalaureate curriculum designed to promote a beginner level of competence in solving patient problems. The faculty adopted the content, structure, and process model for integration that includes professional language and content, the Outcome-Present State Test (OPT) model of clinical reasoning, and reflective journaling. These strategies show promise for attaining higher levels of student thinking, focusing attention on patient problems, and promoting situated cognition. As students realize that situations are complex, faculty guidance can influence best judgments and facilitate clinical reasoning with feedback on assignments to promote student growth and competence in solving clinical problems.
The significance of good clinical reasoning skills relates to prevention of adverse patient outcomes from failure to diagnose problems, institute appropriate treatments, and manage complications (Lapkin, Levett-Jones, Bellchambers, & Fernandez, 2010). Since the early 1990s, educators in various health care disciplines have questioned the clinical reasoning abilities of new graduates because of the lack of explicit pedagogies to promote these abilities and the inability to measure outcomes (Boshuizen & Schmidt, 2000; Groves, O'Rourke, & Alexander, 2003; Hoben, Varley, & Cox, 2007; Kabanza, Bisson, Charneau, & Taek-Sueng, 2006; Liu, Chan, & Hui-Chan, 2000; McAllister & Rose, 2000; Norman & Eva, 2010; Rochmawati & Wiechula, 2010; Unsworth, 2001). Research with practicing professionals and students over the past two decades has shown very detailed descriptions of domain-specific clinical reasoning differences between novices and experts, which influenced some of the current educational pedagogies. Some authors suggest that a paradigm shift in health care education changed the focus from hypothetico-deductive reasoning within the biomedical model (Elstein, Shulman, & Sprafka, 1990) to narrative reasoning, in which truth is related to contextually constructed realities and clinical reasoning exists from multiple perspectives (Benner, et al., 2008; Edwards & Richardson, 2008; Murphy, 2004). For example, the nursing research surrounding cognitive processes has shown difficulty in demonstrating a relationship between nursing outcomes and critical thinking in clinical settings (Murphy, 2004). Clinical reasoning may be a better measure of the cognitive skills nurses use because it includes reflective thinking in practice contexts where individuals create experiential meanings.
For the purpose of this article, clinical reasoning is defined as the reflective, concurrent, creative, and critical thinking processes by which nurses collect cues, process information, come to an understanding of patient problems or situations, plan and implement interventions, evaluate outcomes, and reflect to learn from the process (Hoffman, 2007; Levett-Jones et al., 2010; Tanner, Padrick, Westfall, & Putzier, 1987; Pesut & Herman, 1999). The clinical reasoning pedagogies suggested in this paper adhere to this definition, and integration across the baccalaureate curriculum is designed to achieve a novice level of competence in solving patient problems upon graduation and beginning practice.
Background
Norman (2005) described the evolution of clinical reasoning over three decades starting with the 1970s (the “golden age of problem-solving”): using think-aloud and hypothetico-deductive methods. Learners at all levels of education were assumed to be using the same thinking strategies for decision making, so the thinking process was believed to be related to content knowledge, not to expertise (Simmons, 2010). In the 1980s, gaining expertise was thought to be a process of acquiring a large set of representative cases. Knowledge could be encapsulated until needed, and extensive practice with clinical problems aided in organizing this knowledge. During this time, nursing educators were concerned about cognitive processes for thinking about patient issues, and embraced the information processing model (Jones, 1988). The 1990s was the “age of mental representations”: basic science or causal knowledge was stored as scripts, schemas, or exemplars. Experts use experience-based, multidimensional, and encapsulated knowledge for conditional reasoning that involved understanding patients’ problems in specific life contexts (Liu et al., 2000).
More recent research focuses on the differences between experts, who use forward reasoning from data to diagnosis, and novices, who use backward reasoning from diagnosis to data. To become expert, one must practice with multiple strategies and sequence problems to maximize and optimize learning for transfer to future situations (Norman, 2005). Some educators question whether clinical reasoning exists at all, if there is no one best way to solve problems, and expert reasoning is complex and multidimensional in terms of knowledge and skill (Norman, 2005). The key may be to encourage deliberate practice with a variety of examples to facilitate the formation of scripts and schemas from conceptual knowledge that adds to the repertoire of stored information (Kabanza et al., 2006). Significant nursing research in this area shows that becoming expert in a discipline depends on practice, intuition, and insights gained through interactions in authentic situations (Benner, 1984; Benner, Hughes, & Sutphen, 2008; Greenwood & King, 1995; Tanner, 2006).
Clinical Reasoning Attributes
Clinical reasoning attributes include data analysis (interpreting information), deliberation (rumination), heuristics (informal thinking strategies), inference (speculation), metacognition (reflective thinking), logic (argument), cognition (perception or awareness), information processing (organizing data), and intuition (insight independent of reasoning; Simmons, 2010). Whether strategies are formal (decision analysis or information processing) or informal (heuristics), inductive and deductive reasoning depend on multiple internal and external factors such as cognitive ability, life experience, maturity, and skill level (Brody, 2003; Liu et al., 2000; Norman, 2005; Pottier et al, 2010; Redding, 2001; Rochmawati & Wiechula, 2010; Schunk, 2008). Most scholars agree that clinical reasoning is a context- dependent, domain-specific, recursive process that moves forward or backward to consider a situation's defining features (Gillespie, 2010; Schuwirth, 2009). Furthermore, the decisions occur within a multilayered context including micro- (nurse and patient), meso- (unit and health care agency), and macro- (professional society and government) levels that potentially include social, cultural, political, ideological, economic, historical, temporal, and physical factors (Gillespie, 2010). These complicated contexts are a barrier to clinical reasoning skills, particularly in complex and unpredictable contemporary health care environments. Three integrated pedagogical methods that have been identified to promote clinical reasoning are problem-based learning, iterative reflection and feedback, and concept mapping (Smith & Anderson, 2008). Prerequisites for success include allowing for individual student differences in the processing and storage of clinical information (Schuwirth, 2009), and use of clinical reasoning strategies in an integrative manner throughout a curriculum (Norman, 2005).
Becoming expert in a discipline depends on practice, intuition, and insights gained through interactions in authentic situations.
Clinical Reasoning Framework
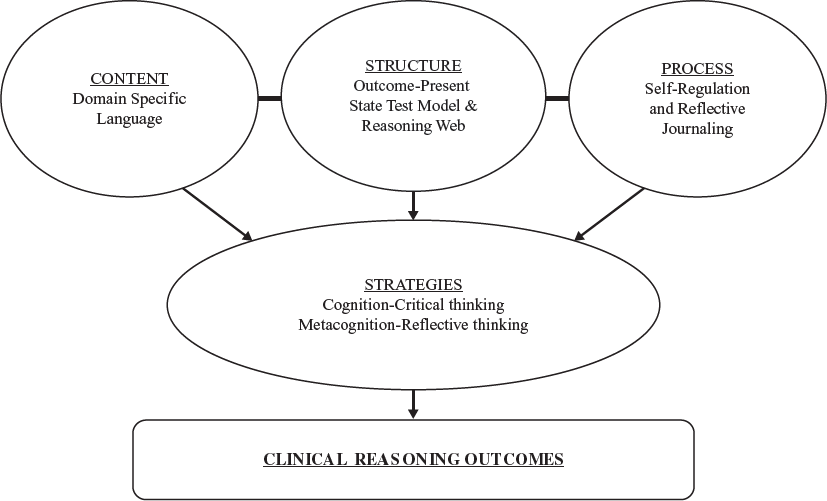
A Clinical Reasoning Framework, shown in Figure 1, was tested and implemented for eight years in an undergraduate nursing program that includes pedagogies that address the content, structure, and process inherent in successful clinical reasoning (Kuiper, Pesut, & Kautz, 2009). Novice students first master the content—the clinical vocabulary and knowledge represented by nursing language associated with patient health issues—so that situations and complex phenomena are framed, categorized, and organized into concepts for clinical reasoning (Benner, Tanner, & Chelsa, 1996; Decker, 2006; Groves et al., 2003; Hoben et al., 2007). These students also need structure in the form of a framework or scaffold for cognitive activities, to practice formulating health and illness scripts and schemas that can be used in future situations. Metacognitive processes of reflective thinking then pull experiences together to enhance competence in problem solving on the journey to developing expertise. When these skills are situated in authentic clinical experiences and/ or simulation scenarios, the appropriate choice of nursing interventions can be framed for each particular patient. Research has shown that the clinician considers the patient's particular clinical trajectory, concerns and preferences, particular comorbidities, and specific responses to past therapies to make decisions and form conclusions (Benner et al., 2008). The timing and processing of these experiences is important and drives the need to integrate supportive pedagogies throughout a curriculum. Students and new graduates have limited work experience, so promoting and supporting these pedagogies is important to prepare the beginning practitioner (Benner et al., 1996).
Content, Structure, Process Model.
Progressing from inductive reasoning, which moves from facts to hypotheses, to deductive reasoning (the style used for clinical reasoning), which moves from hypotheses to the gathering of confirmatory information, is a process that occurs over time (Hoben et al., 2007; Pottier et al, 2010). Novices need help with this process, and concept mapping with reflection is a strategy that can improve accuracy of outcomes. Concept mapping supports clinical reasoning and can assist with pattern recognition for accuracy and diagnostic success (Kautz, Kuiper, Pesut, & Williams, 2006; Pottier et al., 2010). In fact, the reasoning process is more important than the final outcome, so patient cases for student practice should be complex enough to encourage different reasoning pathways to provide opportunity for feedback and conceptualizing problems at deeper levels (Hoben et al., 2007; Kabanza et al., 2006; Müller-Staub, 2009). Self-regulation of cognition and metacognition during clinical reasoning through reflection, assessment, and monitoring has been shown to improve attention to thinking in nursing, occupational therapy, and speech and language therapy students (Kuiper, Murdock, & Grant, 2010; Liu et al., 2000; McAllister & Rose, 2000; Schunk, 2008; Unsworth, 2001).
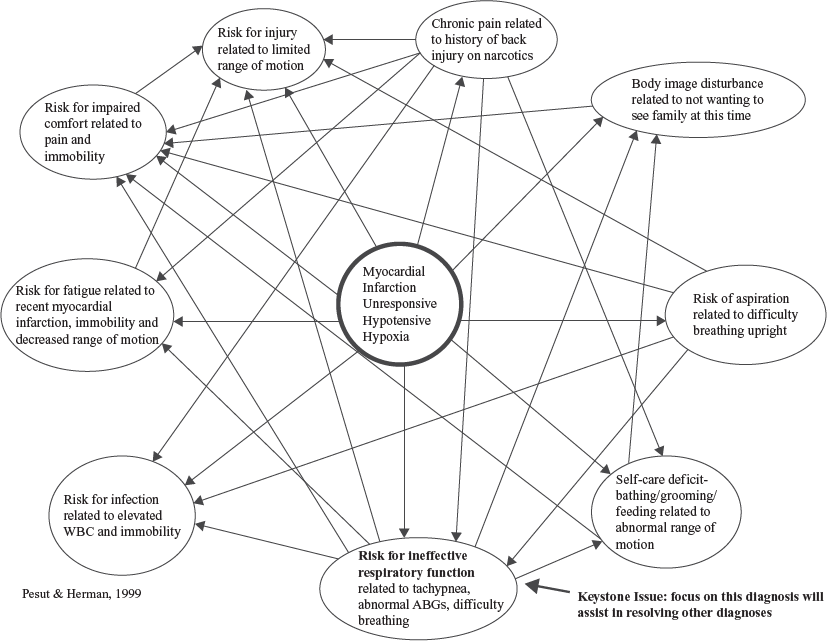
The clinical reasoning web shown in Figure 2 is a structure for concept mapping that prevents premature closure on considering all the data inherent in a patient scenario and avoids reliance on prototype features in a situation. As a scaffold, the clinical reasoning web encourages situated cognition by helping students consider all significant data and priorities to plan interventions and project outcomes. The client-in-context story is derived from multiple sources of patient/family assessment and history, and supports the selection of nursing diagnoses that accompany a particular health problem. Evidence-based nursing diagnoses are intimately related to the medical diagnosis and reflect the priority need of a particular patient within the frame identified by the practitioner during clinical reasoning. The clinical reasoning web aids students in discovering relationships between the chosen nursing diagnoses to determine the priority that achieves the greatest number of connections with the others and is at the center of the patient's problem. This type of concept mapping has been used with other disciples as a bridge between theory and practice as students apply knowledge and experience to new situations (Kabanza et al., 2006; Pottier et al., 2010; Rochmawati & Wiechula, 2010).
Clinical Reasoning Web.
Progressing from inductive reasoning, which moves from facts to hypotheses, to deductive reasoning (the style used for clinical reasoning), which moves from hypotheses to the gathering of confirmatory information, is a process that occurs over time. Novices need help with this process.
Creating scripts or schemas is also important to the clinical reasoning process because they explain how humans understand real-world events. Charlin, Boshuizen, Custers, and Feltovich (2007) associate script theory with clinical reasoning because scripts are created from repeated experiences that are organized and encapsulated into long-term memory. The process of increasing clinical expertise in medical students was shown to depend on integrating foundational knowledge into clinical concepts, which then became encapsulated into illness scripts (Boshui-zen & Schmidt, 2000; Groves et al., 2003). Scripts or schemas are goal-directed and adapted to situations so that chosen interventions are efficient and correspond to the domain they come from. As interventions increase in number, they are activated automatically in complex situations, become part of a repertoire, and are nonanalytic based on a pattern.
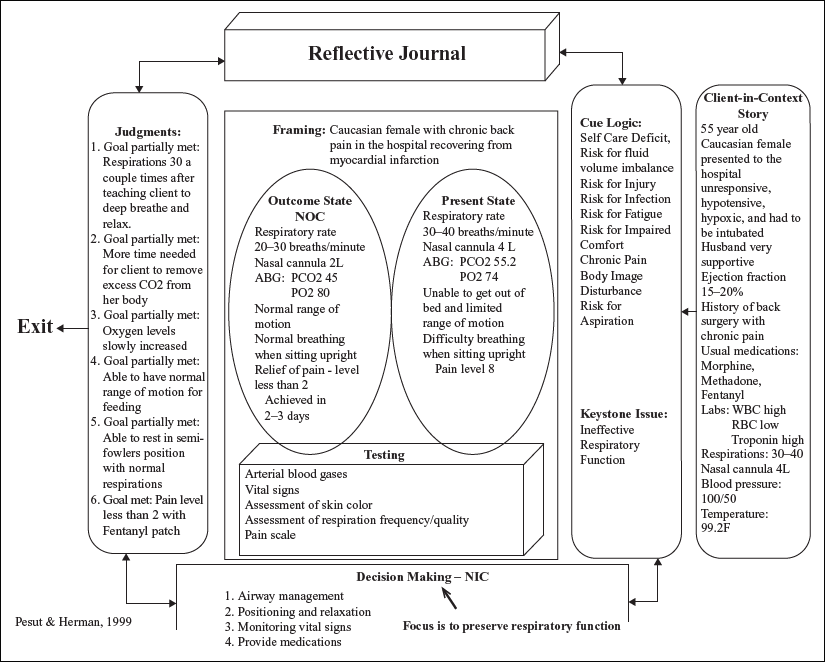
The Outcome-Present State Test (OPT) model of clinical reasoning, shown in Figure 3, helps the student create scripts or schemas with patient situations that are easily organized for storage in memory. The student determines the present state of the patient in time and states the major issues that justify the priority diagnosis. He or she then chooses outcomes that match the present state issues and determines which tests will show a change from present state to outcome state once interventions are applied. The frame includes the context, aesthetic state, and cognitive and psychomotor abilities of the patient that determine the choice of nursing interventions. As nursing outcomes and interventions are related to the priority nursing diagnosis, clinical concepts are formed into scripts or schemas that can be used in future clinical situations. Finally, through further reflection, the student judges whether interventions were successful, outcomes were achieved, and tests were appropriate to solve the patient's problems. This scaffolding helps students organize all the content that has to be dealt with to solve a problem, provide structure, provide language to label the data, and promote reflection on the experience, all of which are essential for clinical reasoning development.
OPT Model of Clinical Reasoning.
Investigations into guided clinical reasoning for nursing students show that accurate use of nursing classification is related to improvements in nursing/ patient sensitive outcomes that are then documented.
Curriculum Integration
The OPT model of clinical reasoning shows promise in deepening student thinking, refocuses attention on patient problems, and considers situated cognition. When we changed from the traditional care plan format to the OPT model worksheets, students expressed enthusiasm and viewed the assignments as more patient-focused and less as “busy work.”
The process of integrating the OPT model into the curriculum begins with describing the worksheets as a scaffolding measure to support thinking processes until they become habitual, help organize content knowledge into scripts or schemas, and improve confidence in clinical reasoning skills. The worksheets provide a visual representation of the thinking involved in clinical reasoning. While completing the worksheets, students are encouraged to use resources to build their knowledge of nursing classifications for diagnoses, interventions, and outcomes. Investigations into guided clinical reasoning for nursing students show that accurate use of nursing classification is related to improvements in nursing/patient sensitive outcomes that are then documented (Kautz et al., 2006; Müller-Staub, 2009). To evaluate outcomes, faculty use a rating tool to give students feedback on their use of the worksheets, and the students use the same rating tool as a guide for adhering to the specific sections of the model.
The undergraduate faculty at our school integrate the OPT model of clinical reasoning across the curriculum through the different specialties and advance through levels of acuity in assignments. The use of the OPT model worksheets varies by course, making evaluation of its use difficult; however, a consistent advantage of the worksheets is that students must plan care that is specific to each individual patient instead of copying prepublished plans from textbooks or articles.
Integration of the clinical reasoning web and the OPT model of clinical reasoning into our undergraduate curriculum (see Table 1) begins in the first semester junior level with a foundational course, Clinical Reasoning and Scientific Inquiry, in which the OPT model worksheets are introduced one section at a time and practiced in three classes. In a companion clinical nursing course, Adult Health I Nursing, seven OPT worksheets are completed, with the five best examples graded on a pass/fail basis. The goal is to achieve mastery in the use of the OPT worksheets in order to promote habitual clinical reasoning with nursing language and knowledge in clinical contexts. Reflection on five clinical experiences with course-specific prompts is also introduced in this first clinical course to promote metacognitive skills.
Integration Plan for Clinical Reasoning Strategies
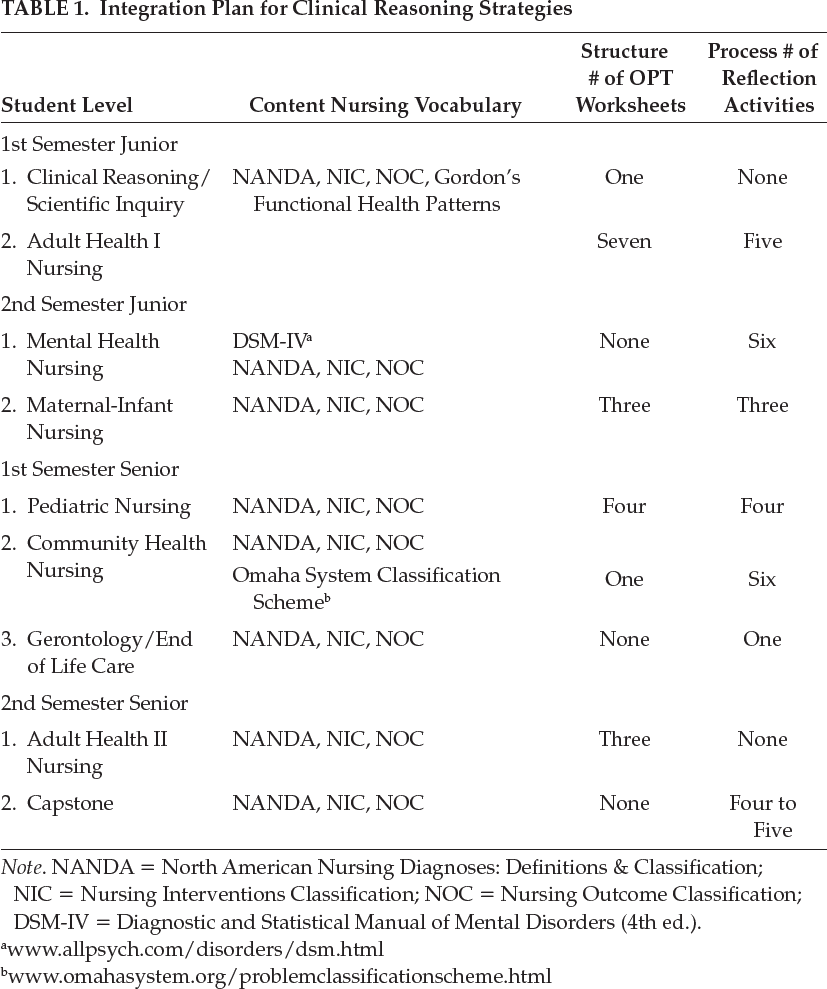
Note. NANDA = North American Nursing Diagnoses: Definitions & Classification; NIC = Nursing Interventions Classification; NOC = Nursing Outcome Classification; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders (4th ed.).
The second semester junior level course, Mental Health Nursing, does not use the OPT model worksheets but includes six reflective journals with course-developed prompts for specific in-patient and community experiences. Our faculty find that concurrent validity for clinical reasoning assessment is needed to capture thinking surrounding therapeutic communication, similar to another program that used the OPT model worksheets with 43 nursing students in a mental health course (Bartlett et al, 2008). The students in this level also complete three OPT worksheets in the corequisite Maternal-Infant Nursing course; one is completed as a group project with 8–10 students following simulated experiences, and two are individual assignments following acute care clinical experiences. Students receive detailed feedback on their OPT model worksheets and reflect on necessary changes.
In the first semester senior level, students complete a reflection activity at the end of the Gerontology/End of Life Care course on an applied learning experience evaluating long-term care patients and facilities. Whereas in the Pediatric Nursing course, students complete four different OPT model worksheets until there is a comprehensive example. The clinical reasoning activity in the Community Health course includes one comprehensive OPT model worksheet for a home care visit and six reflective journals during the semester.
In the final senior level semester, students enroll in the Adult Health II Nursing course, in which three OPT model worksheets are completed on patients with complex health problems and four to five reflective journals are written during the 125-hr capstone experience. At this point, students are very familiar with the OPT model worksheets and reflection, and need little guidance; feedback is often supportive rather than corrective.
Novices who have developed the habitual cognitive skills of deductive and inductive clinical reasoning to recall scripts and schemas for understanding the human response to illness beyond a simple cause-and-effect model are exemplars of successful clinical reasoning pedagogy.
The integration pattern is not the same in all courses and is reevaluated annually because individual faculty members choose pedagogies and assignments that best suit each clinical area. The use of the OPT model helps students achieve the overall learning outcomes for the program such as passing grades in clinical courses, favorable evaluations of performance from clinical facilities and employers, yearly licensure exam pass rates greater than 94%, successful accreditation reviews, and less than 5% attrition per student cohort. A comment from a recent graduate who took the licensure examination reflected on program assets that helped in passing the exam, including problem-solving practice with the OPT model worksheets for clinical experiences. There are annual reviews of the OPT model worksheets and reflection pedagogies for new and experienced full-time and part-time faculty. An Essentials of Clinical Reasoning presentation is available as an MP3 file to all interested faculty and nurse educator graduate students.
Implications for Practice, Education, and Research
Novices who have developed the habitual cognitive skills of deductive and inductive clinical reasoning to recall scripts and schemas for understanding the human response to illness beyond a simple cause-and-effect model are exemplars of successful clinical reasoning pedagogy. The comparisons and critical reflections used in completing the OPT model worksheets and narrative journals enable dialogue with patients about their perspectives and influence decisions about interventions and judgments of outcomes. As health care shifts to community settings with chronic illness management, new graduates’ competence in solving patient problems is extremely important, and can be facilitated with clinical reasoning practice using situated cognition and reflection strategies.
As health care shifts to community settings with chronic illness management, new graduates’ competence in solving patient problems can be facilitated with clinical reasoning practice using situated cognition and reflection strategies.
The implications of our experiences for teaching and learning pedagogy are that incorporating a curricular model promoting clinical reasoning prepares nursing students for the decision-making required for professional practice. Murphy (2004) suggests the following guidelines for a curricular model:
Practice clinical reasoning in all clinical courses.
Use scaffolding methods until students are able to show good habits of mind.
Promote reflection to enhance the metacognition surrounding clinical reasoning.
Give ample feedback to help students grow in clinical reasoning skills.
Practice with cognitive and metacognitive strategies to facilitate the transfer of these skills to new situations and practice arenas.
The implications for nurse educators are that the desired outcome of student competence in clinical reasoning is enhanced through mentoring and guidance. The clinical reasoning competence in practice will help students to
understand the patient's issues in the context of the world in which the patient lives;
use procedural and content knowledge to place concerns within the social and temporal situation;
propose how the patient's conditions can change and can be managed; and
consider the patient's participation at all stages of care (Liu et al., 2000).
Outcomes are optimized when students are made aware of cognitive biases as instructors promote cognitive and metacognitive strategies for growth in clinical reasoning (Kuiper & Pesut, 2004; Round, 1999; Unsworth, 2001). In using all the educational resources available in the clinical setting, clinical reasoning processes and domain-specific knowledge can be made explicit to the student to enable competent decision making (Murdach, 1995). Faculty guidance and expertise in the clinical reasoning process are essential to promoting growth in student clinical reasoning ability and competence in solving patient problems.
Because expert reasoning is complex and multidimensional, measuring it is a challenge, but is needed to help novices enter practice with skills that will enable competent care and promote professional development.
Implications for further research include the need for continued analysis of the OPT model worksheets, comparing cohorts to each other and over time. Research has shown that students master the OPT worksheets in 4–5 weeks in different clinical areas (Kuiper, Pesut & Kautz, 2009); however, more investigation is needed to measure clinical reasoning with concurrent measures. Transfer of reasoning skills to new domains and situations is promoted by using varied pedagogies, and is a vital area for future study. It is important to continue to test domain-specific clinical reasoning pedagogies because reasoning skills used in daily life may not transfer to new domains (Norman & Eva, 2010). Because expert reasoning is complex and multidimensional (Norman, 2005; Norman & Eva, 2010), measuring it is a challenge, but is needed to help novices enter practice with skills that will enable competent care and promote professional development.
Conclusion
Educators acknowledge that health care situations are complex, and best judgments by students can be encouraged and guided through the use of pedagogies like the OPT model of clinical reasoning, reflection on cognitive and metacognitive processes, and curriculum integration. The educational strategies described in this article are one example of how consistent and focused attention to clinical teaching and learning activities can result in positive outcomes for patients and their families.
Footnotes
Ruth Anne Kuiper, PhD, RN, CNE, ANEF, is a professor in the University of North Carolina School of Nursing in Wilmington, North Carolina.