
Abstract
In this exploratory project, efforts were made to strengthen a relationship-centered, caring milieu to improve communication among nursing staff and to help nurses identify and constructively resolve conflicts. Eighteen interactive workshops addressed communication patterns and helped participants identify causes of conflict, facilitate dialogue, improve collaboration, and resolve workplace conflict. The experiential workshops were analyzed with pre- and post-surveys. Participants perceived as individual and team members that it was less important to like one's colleagues and more important to be committed to the same purpose/goals. Individuals noted the value of respect for each other, regardless of title or position. They reported feeling more hopeful regarding work and that practicing tactics to address conflicts made it easier to confront others when the team goal was clear and shared. They indicated a desire to continue to build on conflict resolution, mediation, stress management, and mindfulness skills.
Collegial aggression and bullying have long afflicted nurses in hospital settings (American Nurses Association, 2006). This article reports the results of a pilot project aimed at increasing relationship-based care at one hospital in the United States.
Review of Literature
Literature from the last decade indicates a strong association between the 30%–60% of newly registered nurses who left their positions and collegial aggression and bullying in the workplace (Beecroft, Kunzman, & Krozek, 2001; Griffin, 2004; MacKusick & Minick, 2010; McKenna, Smith, Poole, & Coverdale, 2003; Winter-Collins & McDaniel, 2000). Connections between nurses who work together can become tenuous, resulting in complaints made about one another (Dellasega, 2009; Farrell, 2001; Longo, 2010). Such poor professional relationships can jeopardize retention (Moore, Leahy, Sublett, & Lanig, 2013). Ineffective communication among peers can also lead to physical and emotional exhaustion and burnout (Dayton & Henriksen, 2007; Scott, Hofmeister, Rogness, & Rogers, 2010). The pervasive fatigue from overwhelming workloads, long hours, and erratic schedules are compounded by nonconstructive feedback by colleagues and/or administrators, and intensify workplace problems (Spence Laschinger, Leiter, Day, & Gilin, 2009) and the potential for making errors (Barker & Nussbaum, 2011). Additional stressors may include inconsistent support and insufficient resources (Buchan & Aiken, 2008), lack of recognition, impeded advancement opportunities (Dickerson, 2013; Toh, Ang, & Devi, 2012), and ever-increasing expectations of technological competency (Trossman, 2014).
Risks in the workplace further exacerbate stress (Gaffney, DeMarco, Hofmeyer, Vessey, & Budin, 2012) and compromise nurses ‘well-being. These risks can range from physical hazards such as exposure to toxic pathogens to emotional victimization (Heath, Johanson, & Blake, 2004; Longo, 2010). Yet, despite these destructive challenges, nurses are expected to provide professional care (Barrere, 2013). Nurses need to be skilled in emotional intelligence (Codier, Kooker, & Shoultz, 2008; Goleman, 1995), self-regulation (Evans, Bartol, & Courts, 2014), and self-care (McElligott, 2013) to provide safe, quality care for others.
Workplace norms need to be adopted and actualized to encourage nurses to practice self-care (Dossey & Keegan, 2013). Research shows that even short breaks taken at work can improve work functioning and decrease fatigue (Rogers, Hwang, & Scott, 2004). Tactics such as relaxation techniques, meditation, imagery, and mindful and contemplative practices are cost-effective (Anselmo, 2013; Anselmo, 2016; Larkin & Anselmo, 2014), can reduce symptoms of burnout and increase well-being and productivity (Landa & López-Zafra, 2010), and can generate a greater capacity to care for others (Watson, 2004, 2006).
Ongoing efforts to improve professional nursing practice (Broom & Tilbury, 2007) are aligned with the goals of Magnet designation. Hospitals with this prestigious status are known to attract and retain excellent nurses who continuously perform at higher levels of competency in healthy work environments. Nursing leaders in Magnet hospitals need to be visible and model open communication and mutual respect (Kramer & Schmalenberg, 2008; Kramer et al., 2008; Laschinger, Almost, & Tuer-Hodes, 2003). In addition, there must be evidence of shared governance and shared decision making, collaborative practice, adequate nursing staff ratios, and a milieu that values nurses ‘contributions (Heath et al., 2004).
Study Design
Aims of the Study
This article describes a pilot project in an urban/suburban 292-bed hospital preparing for Magnet application. Two study questions were explored:
How does participation in a series of relationship-based care workshops change participants ‘perceptions of nursing practice?
How does participation in a series of relationship-based care workshops change participants ‘perceptions of self and team behaviors and attitudes?
Ethical Considerations
The hospital and the researchers ‘college gave institutional review board (IRB) approval. A verbal explanation was given to the participants that completion of the anonymous surveys indicated consent.
Participants
Attendees (n = 129) worked on different floors, specialties, and shifts throughout the hospital. All were staff nurses or nurse managers; their professional experience ranged from novice to near retirement. Additional demographic information was not collected to preserve confidentiality.
Procedure
As part of a larger initiative to transform a hospital into a high-performing one, the researchers were invited to develop and provide 18 conflict resolution and relationship-building workshops to improve intra- and interprofessional communication. Recent strategic and administrative changes had been put into place to flatten the hospital's organizational structure and strengthen shared governance. The nursing administration used the book Relationship-Based Care: A Model for Transforming Practice (Koloroutis, 2004) as a resource for nurses. Relationship-based care is comprised of three relationships: with patient and family, with co-workers, and with self. The researchers incorporated elements of this book into their design of the workshop sessions to facilitate reflection and to help participants explore strategies to improve their nursing practice.
At the beginning of the workshops, norms were established for confidentiality and mutual respect. A contemplative and progressive relaxation meditation was provided, and the values of relationship-based care (Watson, in Koloroutis, 2014, p. viii-ix) were integrated into the induction process. The format of the workshops included lecture on tenets of building positive communities. The facilitators described ways of building constructive relationships and strengthening emotional intelligence. Additional instructional materials developed and compiled by the workshop facilitators emphasized the dialogue process (Bohm, 1992) among participants and guided them via dialogue and hands-on activities to develop and strengthen constructive, therapeutic communication strategies (Larkin, 2014) and skills in mindfulness, shifting perspectives, empathy building, and self-regulation. Based on participants ‘lived experiences regarding workplace conflicts, scenarios developed by the facilitators focused on using role play and simulation exercises to build therapeutic communication skills. The participants practiced conflict resolution and peer mediation techniques to resolve their described workplace conflicts and to improve their professional relationships.
A series of three workshops (Workshops I, II, and III) took place in a medium-sized urban/suburban hospital. Depending on their availability, participants completed one, two, or three of the workshops. Workshop I was a full-day session. Workshop II, a half-day session, was offered 2, 3, 4, or 5 months later. Workshop III, a half-day session, was given 12 months after the second workshop to allow for integration and practice of content. The size of Workshops I and II ranged from 15 to 22 participants. Approximately 50 participants attended the final workshops. Pre-and post-training surveys were conducted after the initial and final workshops. Participating nurses received continuing education credits for their participation and were compensated for their time.
Stressors experienced by nurses include inconsistent support and insufficient resources, lack of recognition, impeded advancement opportunities, and ever-increasing expectations of technological competency.
Data Collection
Pre- and post-training surveys from the Commitment to My Co-Worker Healthy Team Survey (Koloroutis, 2004, pp. 257–258) were administered at the beginning and end of the workshop series. Permission to use this survey was given by the publisher. Reliability and validity of this tool were not reported. The 15-item survey included statements referring to perceptions of self and team relationships (Koloroutis, 2004). Respondents were asked to rate themselves and their team on each question on a 7-point Likert scale (with 1 being the least positive and 7 being the most positive). In consultation with the nursing administrators at the hospital, the authors/researchers added the following two open-ended questions:
Tactics such as relaxation techniques, meditation, imagery, and mindful and contemplative practices are cost-effective, can reduce symptoms of burnout and increase well-being and productivity, and can generate a greater capacity to care for others.
How do you feel at the end of the day?
How do you feel at the beginning of the day?
Data Analysis
Surveys were hand coded into Excel tables. The ordinal data were analyzed in R (R Development Core Team, 2008). A comparison was made between the pre- and post-questions. Because of anonymization, researchers did not identify individual responses.
The analysis consisted of two parts. First, a comparison was made between the pretest and posttest Likert survey answers. Second, a word frequency analysis was performed for the open response sections of the pretest and posttest groups. Survey answers were pooled into pretest I (n = 129) and posttest groups (n = 69). Because data were ordinal, standard statistical measures (means, standard deviations, and t tests) were not appropriate analyses. Instead, medians and quartiles were used to summarize the data, and the authors compared median responses per question between groups with a nonparametric Mann-Whitney rank test. Pre and posttest questions were directly compared against each other rather than combined into a single, composite measure.
Results
Seven of the 30 questions indicated statistically significant positive changes between pretest and posttest at the p = .10 significance level. Three of these items were statistically significant at the p = .05 level (see Table 1), which are suggestive of beneficial effects of the workshops.
Mann-Whitney Rank Test: Comparison of Pre- and Post-Surveys
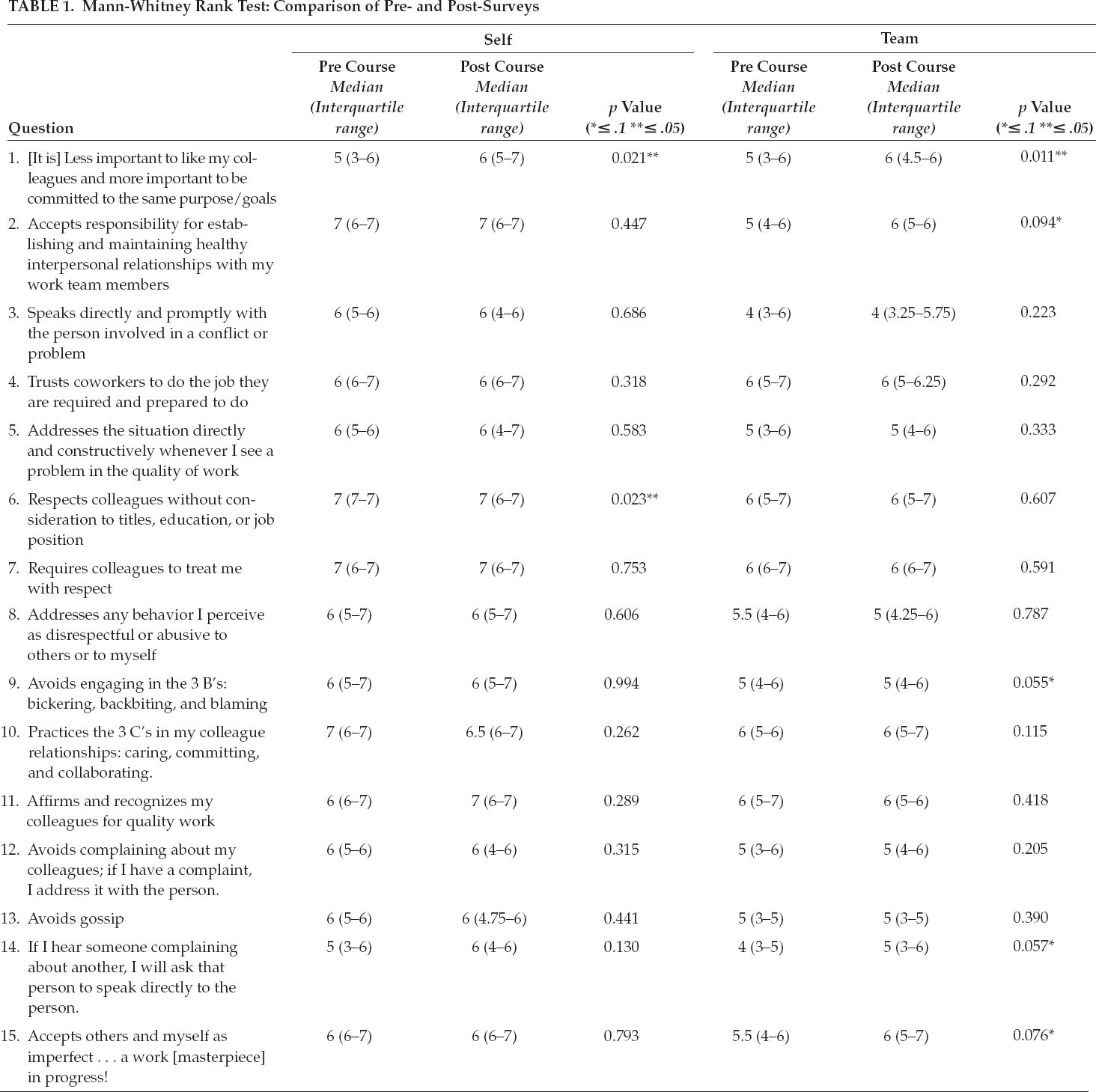
The largest and most statistically significant changes across pre- and post-tests were for Question 1: “[I agree that it is] less important to like my colleagues and more important to be committed to the same purpose/goals” and “[My team agrees that it is] less important to like my colleagues and more important to be committed to the same purpose/goals.”
For the word frequency analysis in both pretest and posttest responses to “How do you feel after work?” the most common responses related to “fatigue” were words such as “tired” and “exhausted.” The second most common sentiments were variations on the word “good.” For the question, “How do you feel before work?” the most common words written on the pretest and posttest surveys were “ready” and “hopeful.” The sentiment most common in the pretest that was absent in the posttest was “anxious.” These are all important findings in facilitating an evolving culture of civility and respect.
Further observations throughout the workshops revealed emerging themes, which were shared with administrators while preserving confidentiality of participants. Participants reported that practicing tactics in real and simulated conflictual situations made it easier to confront others when the team goal was clear and shared. By focusing on common goal attainment, participants acknowledged a priority of effective team practice and a growing culture of relationship-based care. Participants also indicated the value of practicing relaxation techniques and mindful exercises during the workshops and on their own to augment their own stress management. They reported having growing confidence in their ability to be proactive and use constructive communication and conflict resolution skills. Many comments in the posttest evaluations indicated participants ‘desire to build on conflict resolution and mediation skills.
Of the 30 Likert survey items, 15 separate statements pertained to “self” (for me or I), and 15 statements referred to perspectives about their “team” (for my team). The following statements indicated a statistically significant positive change between pretest and posttest distributions on the Mann-Whitney test:
Less important [for me] to like my colleagues and more important to be committed to the same purpose/goals
Less important [for my team] to like my colleagues and more important to be committed to the same purpose/goals
[My team] accepts responsibility for establishing and maintaining healthy interpersonal relationships.
[I] respect colleagues without consideration to titles, education, or job position.
Avoids engaging in the 3 B's: bickering, backbiting, and blaming [for my team]
If I hear someone complaining about another, [my team] will ask that person to speak directly to the person.
[My team] accepts others and myself as imperfect … a work [masterpiece] in progress!
The largest and most statistically significant changes across pre- and posttests were for the questions, I agree, and my team agrees that it is less important to like my colleagues and more important to be committed to the same purpose and goals.
Discussion
A key factor in a healthy work milieu is supporting constructive relationships among colleagues, as emphasized in the Code of Ethics for Nurses with Interpretive Statements (American Nurses Association [ANA], 2015a). The American Association of Critical-Care Nurses (AACN; 2005, 2008, 2016) and the International Council of Nurses (ICN; 2012) have issued standards and policies that address the necessity to create a culture of civility, kindness, professionalism, and ethical conduct (AACN, 2005, 2008, 2016; ANA, 2015a, 2015b; Barrere, 2013; Cronenwett et al., 2007; ICN, 2012). Health and safety standards include appropriate dispositions and attitude (ANA, 2010).
Skilled communication was the first of six standards outlined by the AACN (2005) to promote healthy work environments that are key to the satisfaction and retention of nurses. The Joint Commission (2008) and Kurtzman and Fauteux (2014) emphasize the importance of educating all team members in appropriate professional behaviors and developing a norm of zero tolerance for intimidating and/ or disruptive behaviors. They highlight the need to provide skills-based training in relationship-building and collaborative practice, including giving appropriate, timely feedback and resolving conflict constructively.
Because professional nurses must work well with others in intensive and unpredictable environments, they should be confident in expressing their individual needs while constructively responding to the needs of a group. Nurses need to have constructive and collaborative relationships among colleagues and patients (College of Nurses of Ontario, 2009). Strong interpersonal communication skills promote effective, efficient teamwork. Relying on others is rewarding when the team is working collaboratively toward common goals.
When colleagues communicate poorly with each other, situations can become toxic. Dayton and Henriksen (2007) reported that communication failures contributed to nonconstructive and ineffective health care outcomes. Conflictual issues may arise within this team environment that “rock the boat,” such as unexpressed and repetitive irritants (e.g., leaving a mug in a sink—again; not cleaning up the IV drip—again; coming late for rounds—again). When these seemingly small irritants occur, unhealthy negative behaviors can spiral. Other, more significant irritants may include repeatedly coming late to work and/or to meetings. When these offenses reoccur, patterns of incivility can potentially escalate and lead to volatile behaviors. In preliminary workshops, participants described these examples and patterns of nonconstructive behaviors as typical:
The person does not wish to confront the other(s) because although the situation is frustrating and irritating, the overall working group relationships are acceptable. This is commonly viewed as using the defense mechanism of suppression (i.e., suppression).
The person may not address the issue but instead communicate with another in a passive aggressive way (i.e., passive aggressiveness).
The person chooses to discuss the issue with other colleagues rather than addressing it directly with the individual(s) involved (i.e., gossiping).
The person does not feel comfortable confronting another(s) and instead goes home and displaces anger on family/others (i.e., displacement).
The person rationalizes the irritating behavior as a minor event and internalizes it. Often, such repressed feelings emerge in other nonhealthful ways (i.e., rationalization, repression, and displacement).
The person confronts another with such hostility and accelerated volatility that new problems develop (i.e., road rage behavior).
With such an abundance of conflictual issues, there is a paucity of solution-focused interventions that are geared toward sustainable resolution. Multifaceted interventions that facilitate the building of trust, shared decision making, and skilled communication in working relationships are still sorely needed.
Participants reported that practicing tactics in real and simulated conflictual situations made it easier to confront others when the team goal was clear and shared.
Recommendations
To augment a culture of relationship-based care, multidimensional educational programs should emphasize self-care strategies, including mindfulness and progressive relaxation, to ameliorate the deleterious effects of fatigue and stress. In addition, programs should include education on strengthening constructive conflict resolution, peer mediation, and emotional self-regulation for all hospital community members. Nursing schools should also include this type of multifaceted content within their curricula to support the preparation of future registered nurses (Trossman, 2014) in a relationship-based, caring community. Additional research should be performed with a larger sample size at other hospitals to generalize to other populations and settings. Longitudinal research is indicated to explore additional interventions that can cultivate more constructive relationships within caring, collaborative milieus.
Limitations
Because of scheduling, not all participants attended the three workshops, thus challenging the makeup and dynamics of the group process. A more rigorous analysis would have strengthened the findings if participants had attended all sessions. Commitment by the highest level of administration is essential to this type of education so that individuals can be scheduled to attend all trainings. Improved attendance and additional techniques for collecting identifiable but anonymized test results with normed reliable and valid surveys would allow for better program evaluation.
By focusing on common goal attainment, participants acknowledged a priority of effective team practice and a growing culture of relationship-based care.
Implications
The results of this study imply that multithemed, experiential workshops geared toward building relationship-based care can yield greater commitment to shared goals at work. Constructive communication with others can improve professional relationships and support a healthier work environment. These interpersonal skills can continue to grow and positively influence all relationships.
Footnotes
Ruth Zealand, PhD, is a professor and chair of the Education Department in the School of Arts and Sciences at The College of New Rochelle in New Rochelle, New York.
Dorothy Larkin, PhD, RN, is a professor and coordinator of the Clinical Nurse Specialist Master's Program in Holistic Nursing in the School of Nursing at The College of New Rochelle in New Rochelle, New York.
Max Shron, BA, is a consultant at Data Strategy in Brooklyn, New York.