
Abstract
Cancer somehow lends itself to military analogies, perhaps because of its status as a threat to life itself. We've declared war on cancer over several decades, viewing cancer as a cell going rogue, dividing uncontrollably, and ultimately breaking through local boundaries to spread. Less well known, but critically relevant to the health care impact of questioning authority, is the war within the breast cancer management community, among those studying molecular and cellular targets in breast cancer biology and those managing the human targets that represent cancer's toll. This article outlines current concepts and controversies about breast cancer, presenting a bio/sociological basis and a mental toolkit for thinking about and coping with this conflict.
Keywords
Cancer, with a capital C, has long been recognized in human experience. The ancients noted that affected tissue could be cut out, but disease often returned (Hajdu, 2011). Cancer somehow lends itself to military analogies, perhaps because of its status as a threat to life itself. We've declared war on cancer over several decades, viewing cancer as a cell going rogue, dividing uncontrollably, and ultimately breaking through local boundaries to spread. An early United States incarnation of the War on Cancer, the 1971 National Cancer Act, saw the conquest of cancer as practically within our reach in real time (National Cancer Institute, 1971). A historical viewpoint has characterized cancer as a pathway of cellular malfeasance best countered by outright physical removal and/or general weapons against inappropriate cell growth. More recently, deployment of specific molecularly-targeted growth inhibitors comprises a cornerstone of therapeutic management (e.g., Herceptin in Her2+ breast cancer).
A loss of innocence now shapes our view of cancer. We've learned it's not a monolithic condition but reflects contributions from genetics, external and local tissue environments, and even a roll of life's dice. The Cancer Moonshot initiative passed by Congress as the 21st Century Cures Act in December 2016 reprises on the current battleground the intentions and infrastructure of five decades ago, albeit in the context of this new realism (National Cancer Institute, 2016). We now recognize (to varying degrees) that the capital C designation can be fluid at best— that a multitude of processes involving a multitude of players influences the onset and course of a highly diverse condition. Amid this understanding, squabbling in the ranks has given rise to clashing armies, brandishing pennants and trumpeting position statements as to just what is cancer and what is not, and what should be done about this conundrum. A review of our most basic biologic understanding of cancer is shown in Figure 1.
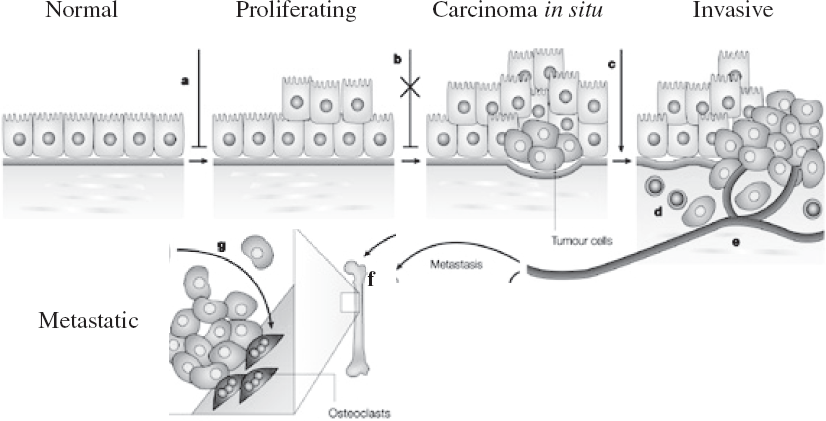
Schematic model of progressive steps in malignant transformation of breast and other cells to culminate in invasive and metastatic cancer. (Adapted from Siegel and Masssague [2003]. Used with permission via Rightslink by Copyright Clearance Center).
Critically relevant to the health care impact of questioning authority is the war within the breast cancer management community, among those studying molecular and cellular targets in breast cancer biology and those managing the human targets that represent cancer's toll.
A YELLOW BRICK ROAD GUIDES TREATMENT
According to this model, a defined progression occurs from initial inappropriate cell proliferation and changes in cellular character (Figure 1b and 1c), to initial invasion into nearby tissue (Figure 1d and 1e), and ultimately metastasis to distant sites (Figure 1f and 1g). This model has worked well in describing colon cancer's molecular underpinnings and sequence of cellular behaviors and in translating this knowledge to therapeutic intervention. Our first step in questioning authority is to ask, How well does this model apply to breast cancer, whose current incidence is one woman in eight (12.5%; National Cancer Institute, 2017)?
Figure 2 shows the female breast structures of primary concern for breast cancer. The lobules bear cells designed to produce milk, whereas ducts transport the milk product onward. Blood vessels (Figure 1d and 1e) and lymph nodes (see Figure 2) can become involved upon entrance of local cancer cells into nearby connective tissue, with lymphovascular invasion and involvement of sentinel underarm nodes. These loci of invasion have traditionally been considered the chief sites from which metastasis to distant regions takes place.
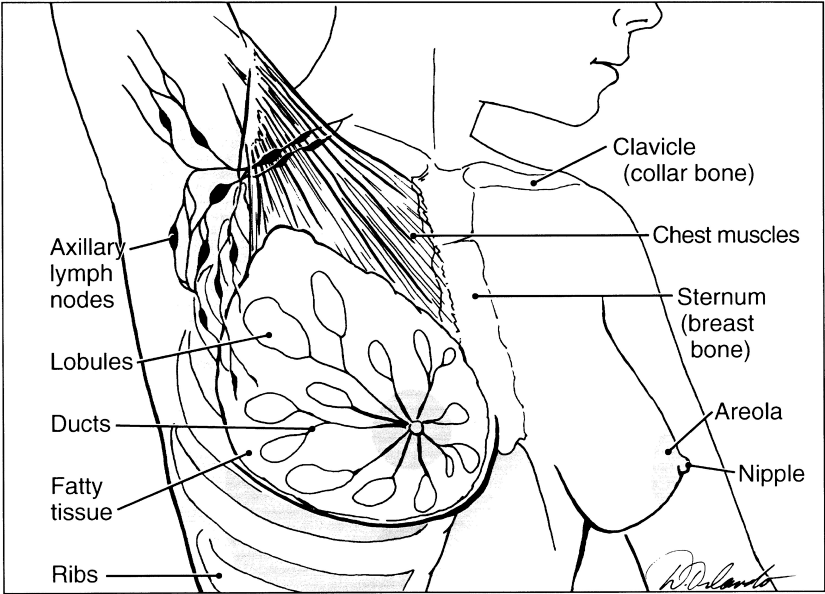
Schematic of breast showing key structures where cancer begins and progresses. (Used with permission from the Allina Health System).
Several key concepts drive the most common formula for breast cancer management based on the model in Figure 1:
Once begun, progression though the steps shown is deemed inevitable with time.
Halting the process, the earlier the stage of discernment the better, is best accomplished by physical removal of the offending locus of activity.
The best means of earliest discernment is mammography, despite prominent caveats about this technology, such as poor efficacy in evaluating dense breast tissue.
Once discerned, strategies augmenting physical removal, such as radiation and chemotherapy, continue largely to target inappropriate growth of the most readily identifiable breast cancer cell population.
We've learned that cancer is not a monolithic condition but reflects contributions from genetics, external and local tissue environments, and even a roll of life's dice.
It is clear that in some circumstances, such as frank invasive breast cancer and high-risk familial mutations, the applicability of this model and the reasonableness of therapies based on it are not open to serious question at this time. However, hidden amid the apparently straightforward schematic in Figure 1 is a veritable alphabet soup of acronyms describing additional cast members good and bad. Unlike the apparent relative homogeneity of colon cancer, breast cancer takes the form of four currently recognized subtypes depending on malignant cell behaviors and molecular profiles: luminal A and B, Her2+, and triple negative (Komen.org, 2017). It is not clear how the Figure 1 scheme can adequately account for this diversity of cancer phenotypes, let alone better inform approaches to therapy. Moreover, a blanket application of this model has sown the seeds of dissension within the community of breast cancer care providers and their patients. A substantial impact of questioning authority has arisen because the questioners are themselves scientists who are leaders in this field.
The prevailing view of LCIS has evolved to become regarded as not cancer itself but an indication of elevated risk for invasive cancer; yet in many quarters, LCIS is subject to a strikingly aggressive posture for treatment.
The Yellow Brick Road Leads to Gray Areas
In the graphics of Figure 1b and 1c, the concepts of “proliferation” and “carcinoma in situ” lie at the heart of the breast cancer wars. This term designates inappropriate breast cell proliferation without the malignant process having yet broken downward through a basement membrane barrier into the surrounding tissue environment. At the level of the lobules, “lobular carcinoma in situ” or LCIS constitutes a numerically small territory in the gray area, accounting for approximately 2% of cases (Cutuli et al., 2015). This condition provides little hint of its presence per se and is often an incidental finding on a breast biopsy undertaken for other indications. It tends to occur as nests of noninvasive cells located throughout both breasts. The prevailing view of LCIS has evolved over decades to become regarded as not cancer itself but an indication of elevated risk for invasive cancer; yet in many quarters, LCIS is subject to a strikingly aggressive posture for treatment ranging all the way to bilateral mastectomy (Anderson, Calhoun, & Rosen, 2006).
The majority of the gray area most prominently identified with breast cancer battles involves the ducts, in “ductal carcinoma in situ” or DCIS. This condition is currently viewed in many quarters as outright breast cancer, designated as “Stage 0” and perceived as firmly on the path to disseminated disease; for an excellent lay public- oriented review about Stage 0, see Hobson (2009). Malignant cells invading the tissues surrounding breast ducts constitute invasive ductal breast cancer, accounting for 55% of all breast cancers (Makki, 2015), as the putative next stage if the model in Figure 1 is, in fact, correct. This perspective underlies how DCIS has historically been treated aggressively based on this model, via mastectomy/lumpectomy and radiation.
Not everyone agrees. Dr. Laura Esserman (Esserman, Shieh, & Thompson, 2009) and a cohort of colleagues in the breast cancer field (Lundberg, 2013; Partridge, Elmore, Saslow, McCaskill-Stevens, & Schnitt, 2012; Topol & Esserman, 2016) argue that the view of DCIS as an obligatory and inevitably progressing stage in invasive breast cancer is neither accurate nor helpful. The model in Figure 1 provides an ideological basis for breast cancer screening via mammography, but this technology has also drawn criticism for the ever-widening net that it has cast. Such screening has enhanced pickup of much smaller tumors than previously, including many that might never have progressed at all, and has substantially expanded the incidence of DCIS diagnosis (Fallowfield & Francis, 2016; Margenthaler & Vaughan, 2015; Sagara et al., 2015). Consequently, many women becoming denizens of the gray area, without real knowledge of its implications or the existence of disagreeing camps, are subjected to treatments that may or may not provide real biological benefit.
The gray area is not the province solely of women's breasts but includes cervical tissue and male prostate tissue as well. These reproductive hormone-dependent secretory tissues spawn intraepithelial proliferation, of unknown cause and bewildering implications, discerned by screening techniques. Some of these cell types give rise to a highly malignant process calling for aggressive countermeasures, and others never do (Castellino, 2017; Wilt et al., 2017). The National Institutes of Health has pointed out that we have no idea which cells have lethal potential and which do not, calling for applications for funding research to figure this out (National Institutes of Health, 2016). New information gained from this requested program would clearly benefit the breast cancer field also.
Many women whose diagnoses are in the gray area of carcinoma in situ are subjected to treatments that may or may not provide real biological benefit.
What is the Impact of Questioning Authority in Breast Cancer?
Nevertheless, the earth moves … Galileo
In the breast cancer arena, questioning authority has an impact on three health care domains and their interactions with one another.
Impact on the Field: Emerging Strategies and the Status Quo
Questioning authority is inherent in the very nature of science … and of scientists. This questioning of current conventional wisdom is what drives scientific progress. Questioning authority reflects such motivations as scientists ‘natural interests and restless curiosity about mechanisms, even to the point of adverse consequences for the thinkers.
Altruism among scientists also drives the search for alternatives, at both basic and applied levels—for better ways of discerning, treating, and possibly preventing breast cancer. At the cutting edge of this field are several new developments aimed at improved detection and management. For example, novel imaging technologies of photoacoustic tomography and photoacoustic microscopy developed by Dr. Lihong Wang and colleagues (Wang & Yao, 2016; Wong et al., 2017) offer rapid analysis of tumor biopsy tissue in images of literally photographic detail. This strategy is already being extended to intact animal studies. Although clinical application in humans may be some ways off, historic TV images of Star Trek physician Dr. Beverly Crusher waving a diagnostic device in the air over Captain Picard may be more farsighted than farfetched.
Analysis of known risk gene panels encompassing breast cancer mutations is now well-established as a standard of care (Easton et al., 2015). However, various DNA profiles of tumors themselves, intended to optimize chemotherapy, have yielded discordant recommendations (Kuderer et al., 2016). Moreover, cellular and genetic makeup of tumors can be heterogeneous at diagnosis and can evolve further with time and tumor progression. This issue hampers not only current disease management but also proposed blood testing to track circulating tumor cell DNA or very rare circulating tumor cells (CTCs).
Defining the spectrum of tumor-associated genes in terms of their protein products is an emerging avenue in identifying molecular targets for drug therapy. Proof-of-concept study investigator Dr. Reid Townsend (as cited in Huang et al., 2017) says, “Requirements for quantities of tumor material and time for analysis presently limit applicability of protein profiling” (personal communication, May 11, 2017). However, such studies break ground for improving breast cancer patients ‘outlook in the future.
Recent advances shake once-solid convictions about behavior of breast cell populations schematized in the Figure 1 model. A confluence of scientists ‘curiosity about why breast cancer metastasizes to bone in 70% of cases (Hussein & Komarova, 2011) and a clinical initiative collecting patient bone marrow has led investigators toward another acronymic disease culprit: disseminated tumor cells (DTCs). The actions of DTCs are suggested in Figure 1d, 1e, 1f, and 1g (upper right and lower left), where cancer cells appear initially as an invading army disrupting the protective basement membrane and claiming local territory. Traditionally, the Figure 1 model includes the notion that sufficient size of the territorial invasion is what ultimately prompts cancer cells to head off into wandering as a cloud of cells or as individuals throughout the circulatory system. This concept underlies the push to catch breast cancer early via widespread screening. DTCs may ultimately settle in the bone marrow cavity right up against the inner bone surface (Figure 1g), there to remain dormant for years, for decades, or for a patient's lifetime. Drs. Katherine Weilbaecher, Rebecca Aft, and others are pursuing the molecular profiling and behavioral characterization of these cells (Aft et al., 2010; Siddappa et al., 2013; Watson et al., 2007). A key area of current investigation is what awakens these cells from dormancy to grow and to prompt nearby osteoclasts to break down bone, decades after the original breast cancer was thought cured. Weilbaecher says, “Keeping these cells dormant and their niche quiet, or alternatively flushing them out and then destroying them by chemotherapy, may help deal with the onset or consequences of breast cancer metastasis” (personal communication, September 23, 2016).
The gray area is not the province solely of women's breasts but includes cervical tissue and male prostate tissue as well; some proliferating cells in these reproductive secretory tissues give rise to a lethal malignant process, and others never do.
An additional recent puzzlement outlines a possible new frontier in countering behavior of breast cells on the putative cancer path. A substantial percentage of DCIS cases have revealed DTCs residing in the bone marrow (Sänger et al., 2011). This suggests that the cells observed in DCIS may not necessarily invade nearby tissue by breaking down the protective basement membrane surrounding lobules and ducts as in Figure 1d and 1e but could potentially traverse the basement membrane that is still intact in Figure 1c, ultimately to enter the circulation and end up in bone marrow. A precedent for such cellular travel between tissue compartments across intact basement membrane occurs in hemopoiesis, the generation of all blood cell types in the bone marrow from a single or “pluripotent” stem cell precursor. This blood cell precursor gravitates from the circulation into its bone marrow niche and back out again through the action of molecular homing signals such as the protein thrombospondin (TSP; Pedemonte et al., 2007). For a broad overview of TSP, see https://en.wikipedia.org/wiki/Thrombospondin. DTCs appear to share with these blood precursor cells not only a propensity for wandering but also a similar homing property effected by TSP. The mutual properties of wandering and common homing signals suggest that both blood stem cells and DTCs may be drawn to or even compete for a common bone marrow niche. Interaction with TSP also serves to keep the DTCs dormant in the bone marrow niche (Ghajar et al., 2013). In questioning the concept of local invasion as a prerequisite for disseminated disease, this new picture may have implications for many aspects of breast health management.
A darker side to the impact of questioning authority on the breast cancer field as a whole is pushback from professional power structures and from financial considerations behind diagnostic and therapeutic conventional wisdom. The authority, in fact, being questioned has over time accrued to thought leaders who designated a standard of care based on the model in Figure 1. Medical centers ‘enormous financial investments in imaging technology and medical care infrastructure generate the expectation of a commensurate throughput supporting cost recovery as well as ongoing growth of the enterprise. Surely the physicians involved have the best interests of patients at heart. However, health care is often the largest financial enterprise in many cities (Allhealthcare, 2017), accounting for 13% of American jobs and serving as a generator of broad financial pressures throughout all arenas of medical practice.
Impact on Care Providers: “What's this about Shared Decision Making?”
Questioning authority forces breast health care providers to take a stand and to defend their position on the medicine they practice. The gray area of DCIS is right in the middle of this battle scene, subject to admonition that surgeons should or should not yet give up their scalpels (Esserman et al., 2009; Margenthaler & Vaughan, 2015; Topol & Esserman, 2016). Also in the middle of the battle are LCIS and its acronymic cousins and sometime biopsy companions, atypical lobular hyperplasia (ALH) and atypical ductal hyperplasia (ADH). In the past two decades, LCIS clinical presentation has prompted recommendations that are all over the map, from outright dismissiveness of concern by breast biology specialists to a current menu of options beginning with chemoprevention via selective estrogen receptor modulators (Maximov, Lee, & Jordan, 2013). A more aggressive approach uses intensive annual monitoring via not only mammography but breast MRI; the latter uses gadolinium contrast media, some of which may be deposited in the brain (McDonald et al., 2015). This observation has generated recent controversy (Olchowy et al., 2017) and at least gives pause about the wisdom of breast MRI as an annual screening tool in high-risk individuals with no current disease. Even the extreme of bilateral prophylactic mastectomy is a recommendation advanced with some frequency to both LCIS and DCIS patients (Anderson et al., 2006; Mulcahy, 2017; Tuttle et al., 2009). Thus care providers are likely to encounter patients in the gray areas who range from compliant to confused to cantankerous. The most significant adverse impact of care provider controversy here lies in its potential distraction of attention and energy from what should be the top priority: learning more about disease biology to know which gray area conditions really do call for more aggressive or less aggressive treatment.
Questioning authority may also impact breast health care providers by shaking the very foundations of their relationship to their chosen life's work. Many factors can promote in care providers a sense of necessity to stake out a position of “directiveness” instead of shared decision making with a patient, especially in breast health gray areas such as DCIS. David Abelson, MD, poignantly describing how physicians come to feel not only responsible but also exalted, attributes the development of these attitudes to the climate of residency training (Abelson, 2017). Self-selection for attitudes of dominant/directive status in health care professionals ‘career choices may also enter into the equation of relationship-based care in a manner fostering an adversarial footing rather than cooperative shared patient-care provider decision making.
A darker side to the impact of questioning authority on the breast cancer field as a whole is pushback from professional power structures and from financial considerations behind diagnostic and therapeutic conventional wisdom.
Financial pressures exerted on care providers by their organizations can extend beyond imposing a rushed pace on care interactions. Liability issues are a vast space of institutional concerns interfacing with questioning of health care provider authority by patients (Manthey, 2017). In academic health centers where skyrocketing malpractice premiums long ago created incentives for self-insurance, medical practice tends to be highly defensive, “reflexive” rather than “reflective” (LaRocco, 2017). A related agenda is the legal position of care providers vis-à-vis competent, knowledgeable patients who refuse designated standards of care (Carrese, 2006). These latter folks may be viewed as a threat, likely to change their minds and sue. Although Dr. Esserman's viewpoint of “let the woman decide” clearly has its adherents, sadly, the impact of questioning authority on breast health management in the gray areas may well be a hampering of the relationship between the community of care providers and the patient, rooted in mistrust of one another.
Questioning authority forces breast health care providers to take a stand and to defend their position on the medicine they practice.
Impact on Patients in the Gray Area: “Who's in Charge Here?”
Patients being urged to accede to a given care plan may come to question the authority of a breast health establishment whose positions may not make sense when viewed critically. A gray area patient with an initial LCIS diagnosis tends to incur repeated biopsies in a context primarily geared to looking for the presence of DCIS, as a putative next step in a malignant process, to be countered with radiation (Hobson, 2009). The patient may question this part of the plan: Radiation is a known mutagen; would superimposing it on an already abnormal ongoing LCIS breast-wide cellular process stop further progression or would it, in fact, kick carcinoma in situ status up to the next level of malignancy? Where and how good is the data on this, and how likely is such data to be available to any given questioner of authority?
An LCIS patient (name withheld) describes her ordeal of multiple surgical biopsies over decades as “drive-through mastectomy on the installment plan” (personal communication, August 1, 2017). Her health care providers have urged extensive surgery to survey more tissue in a search for DCIS that can then be irradiated. Such gray area management in breast health as a quest for an elusive goal, prompting ever more intensive maneuvers, is based on the model in Figure 1 and the perception that LCIS may represent a stage progressing toward DCIS; this view is yet another point of controversy in this area (Simpson, Gale, Fulford, Reis-Filho, & Lakhani, 2003). Clearly, what this patient needs is a reliable noninvasive means of detecting invasive breast cancer while further research sorts out the implications of acronymic gray areas such as LCIS, DCIS, and DTCs.
A significant impact befalling a patient who questions authority is living with the certainty of uncertainty. Disquietude that comes with understanding how incomplete our knowledge is about the biology of breast cancer and what really is the best approach to this condition may be inevitable, particularly if one has ended up in the gray area. Questioning authority based on a patient's own knowledge base, or critical reading and thinking, or temperament, unquestionably leads to a great deal of extra work. A patient has the right to seek breast health care based on reflective rather than reflexive (LaRocco, 2017) medical practice, but finding the right health care providers for one's own circumstances is time consuming and anxiety provoking; care providers may react negatively to being questioned, refuse up front to care for, or subsequently fire the patient. Dr. Esserman attests to a flood of e-mails received from women who are authority-questioning gray area patients (Topol & Esserman, 2016). Such patients would do well to acquire information about care providers under consideration and their staff people who manage their time, and never go unprepared, presenting a complicated agenda, into a busy clinical service with clockworklike time constraints. Instead, they should first explore with candidate breast health care providers the optimal means to establish a relationship in which their care concerns can be politely communicated and discussed.
In the end, the impact on the patient of questioning authority is best told in a true story. Dr. X, an academic physician, developed a most serious form of cancer, about which his institution's physicians offered a grim prognosis. A wine aficionado determined to live his remaining life to the fullest, he headed to his favorite wine shop and confided his circumstances to its owner, a friend who related how his own parent had had the exact same cancer successfully treated by a different physician in the same department that had suggested Dr. X should primarily put his affairs in order. This other physician was not only willing to treat Dr. X but welcomed his knowledgeable input. After an admittedly harrowing treatment course, Dr. X is alive, disease-free, and headed for the beach, having questioned authority and had his life saved by his sommelier's mother.
Patients have the right to seek breast health care based on reflective rather than reflexive practice; they should explore with candidate care providers the optimal means to establish a relationship in which their care concerns can be politely communicated and discussed.
Footnotes
Nancy L. Baenziger, PhD, is an associate professor of neurobiology (Ret.) at Washington University School of Medicine in St. Louis, Missouri. Her original discovery of thrombospondin (TSP) laid the foundation for what has grown into a broad research area of human biology. TSP is now known, among other actions, as a molecular homing signal that has implications for understanding and confronting the actions of disseminated tumor cells (DTCs) in breast cancer.