
Abstract
Transgender and non-binary patients are greatly impacted by political initiatives intended to diminish their rights, including the right to access to gender-affirming medical care. Nurses who provide Person-centered Care (PCC) are uniquely positioned to honor their patients’ rights and humanity. PCC is an important component of building trust with transgender and non-binary patients, but honoring their humanity fully and comprehensively requires an intersectional approach. To build trust, the authors suggest that a paradigm that interweaves PCC with intersectionality promotes social justice for transgender and non-binary patients.
During the last decade, as transgender individuals have gained more social recognition and visibility, their rights have been consistently questioned and at times attacked in legislation in the United States. In 2021, 147 pieces of anti-transgender legislation were introduced in the US; of these, there were 43 bills that could prevent transgender youth from receiving gender-affirming care (Human Rights Campaign, 2022). These health-care policies may create fear among transgender and non-binary individuals, directly impacting their trust in health-care services. In essence, anti-transgender legislation can lead to medical mistrust, which contributes to health disparities for transgender and non-binary patients.
Medical mistrust among transgender and non-binary patients is not a new phenomenon; data shows that mistrust has been a pervasive and well-documented issue (Grant et al., 2011). Medical mistrust is often exacerbated along lines of socio-economic standing, race, immigration status, and gender identity; “health outcomes for all categories of respondents show the appalling effects of social and economic marginalization” (Grant et al., p. 6). A study by Padrón and Salcedo (2013) found that transgender and non-binary patients who are immigrants and working-class experience even higher levels of mistrust, with 28% of participants reporting that accessing medical services where they were treated with integrity and respect was “very difficult” (Padrón & Salcedo, p. 4). The Report of the 2015 U.S. Transgender Survey (James et al., 2016) revealed that 33% of respondents who had seen a health-care provider in the past year reported at least one negative experience related to being trans-gender or non-binary, and 23% of respondents did not see a doctor when they needed to because of fear of being mistreated as a transgender or non-binary person.
To improve the health experiences of transgender and non-binary patients, institutionalized transphobia must be acknowledged and rectified. In this paper, the authors discuss how bodily autonomy for trans-gender and non-binary patients is highly dependent on social institutions, which may often promote trans-phobia and social injustice. Nurses who understand how social institutions fail to support the wellbeing and bodily autonomy of their transgender and non-binary patients can act as allies and build trust. This paper examines the use of intersectionality as a social justice framework in nursing to affirm the bodily autonomy of transgender and non-binary patients.
Nurses who are committed to the bodily autonomy of their transgender and non-binary patients may find themselves questioning, and at times challenging, domains of power, such as institutional practices in clinics and boardrooms, and the legislation that hinders patients’ self-actualization. Reversing the damage that transphobia has enacted on people's bodies, and specifically honoring bodily autonomy, requires that nurses listen attentively to their transgender and non-binary patients, recognizing how they communicate their bodily needs in relation to structural and institutional power.
Structural and institutional power creates and sustains heteronormative and cisnormative standards that protect and normalize Eurocentric notions of health and deservingness (Spade, 2015). As a result, white, straight, able-bodied, cisgender people tend to have a more stable and secure place in society and in health care than people who identify as Black, Indigenous, and People of Color (BIPOC) and/or queer, transgender, non-binary, disabled, and/or immigrant, and their life chances are greater than the life chances of their counterparts who are considered outside the norm. Historically, the dichotomy between those who are deemed normal and those who are not has supported denying transgender and non-binary people medical authority and bodily autonomy; this dichotomy is especially pronounced among those who are Black, Indigenous, and People of Color (BIPOC) (Snorton, 2017).
Person-Centered Care: Promises and Shortcomings
The World Professional Association for Transgender Health (WPATH) Standards of Care for the Health of Transsexual, Transgender, and Gender Nonconforming People recommends a flexible, client-centered approach when working with transgender and non-binary patients (WPATH, 2012). Based on the WPATH recommendation, scholars and professional organizations have found Person-Centered Care (PCC) a promising framework when working with transgender patients (Knutson & Koch, 2022). PCC is a model in which clinicians center the patient, view the patient as a unique human being, and partner with the patient to personalize care (Knutson & Koch, 2022); it is a rights-based approach that aligns with the promotion of human dignity for the patient. Therefore, PCC is appropriate to challenge the denial of medical authority and bodily autonomy that transgender and non-binary patients experience. However, PCC falls short for transgender and non-binary patients in at least two ways.
First, PCC's emphasis on the individual is insufficient to address transphobia and other forms of oppression that deeply impact transgender and non-binary persons’ health (Austin & Craig, 2015). For example, according to a survey of U.S. transgender adults, two-thirds of respondents reported discrimination in the employment sector (James et al., 2016). For many transgender and non-binary people, job discrimination results in the loss of employment-based health insurance and access to health care, which profoundly limits their bodily autonomy and results in a constant state of survival mode. PCC's focus on the individual patient as an entity separate from the larger social context (e.g. economic and political sectors) overlooks the power that institutions such as labor and medicine have over transgender and non-binary patients’ autonomy. A nurse who is treating a transgender or non-binary patient experiencing a medical issue must consider the “magnitude and effect of transphobic discrimination on the lives and experiences of transgender people” (Austin & Craig, 2015, p. 22).
Second, PCC assumes that the patient has a corrective influence in the health-care system (Hansson & Frödding, 2021; Meranius et al., 2020; Tomes et al., 2011), implying that patients have an equal footing with institutions in decision-making processes in health care. However, Knutson and Koch (2022) state that transgender and non-binary people sometimes hide certain aspects of their identities (e.g., gender expression, sexual practices, socioeconomic status, immigration status, self-management of medical care) when coping with discrimination and societal rejection. Because transgender and non-binary patients experience pervasive marginalization, it is difficult if not impossible for them to have a corrective influence in the health-care system. Understanding that trans-gender and non-binary patients are not just individuals with human rights, but are also people who belong to communities that are institutionally and systemically disenfranchised, provides an intersectional and social justice lens in nursing. Thinking like a nurse involves leveraging medical training and professional influence to advocate for transgender and non-binary patients as individuals and as members of institutionally oppressed groups whose rights are constantly violated. This expansive way of thinking is called intersectionality.
Structural and institutional power creates and sustains heteronormative and cisnormative standards that protect and normalize Eurocentric notions of health and deservingness.
Understanding that transgender and non-binary patients are not just individuals with human rights, but also belong to communities that are institutionally and systemically disenfranchised, provides an intersectional and social justice lens in nursing.
The Expansive Power of Intersectionality
Intersectionality is a paradigm that illustrates the relationship between individuals and the institutions that grant and deny life chances. It reveals how discriminatory practices within our society do not act independently of one another, but rather are interrelated and create compounded systems of oppression and discrimination (Collins, 2000; López & Gadsden, 2016). In the medical setting, transgender and non-binary patients may experience a series of health concerns not only because of their own bodily functions, but also (and most palpably) because of their social standing in a society that offers almost no moral, financial, or spiritual support, especially to those who are BIPOC. An example of this level of vulnerability is a legal minor transgender patient who has been kicked out of their home as result of their parents’ transphobia. This patient has lost medical care, housing, and a sense of belonging. If they go to a clinic for hormone provision or other care, they are denied access because of lack of health insurance. Their intersectional identity as an unhoused transgender youth shapes their access to health care, housing, and safety. In this example, PCC alone only addresses the health concerns and not the context in which they occur. Interweaving intersectionality with PCC helps nurses see the interlocking systems of oppression that are impacting this patient's health. Advocating for this patient entails having knowledge and insight into the ways in which transgender and non-binary people experience institutional oppression; this insight will enable nurses to apply interventions that affirm, promote, and validate their patient's identity, wellbeing, and human worth.
An Intersectionalized Pcc Framework: Implications for Practice
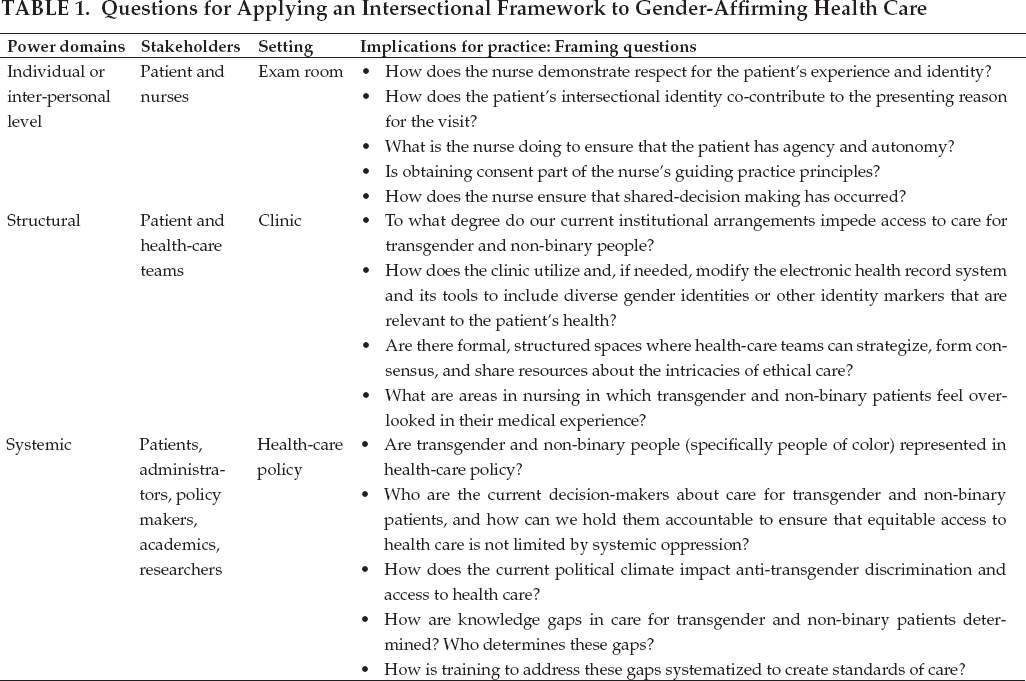
While traditional scholarship may conceptualize intersectionality as an abstract theory, intersectionality in reality has tremendous practical potential. In nursing, intersectionality is a concept that can be used to challenge various forms of oppression, including trans-phobia and racism. Table 1 illustrates how nurses can integrate PCC and intersectionality by asking critical questions that amplify the voice, visibility, and autonomy of their transgender and non-binary patients.
Questions for Applying an Intersectional Framework to Gender-Affirming Health Care
Conclusion
A social justice lens is desperately needed in a political climate in which transgender and non-binary people constantly experience threats to their health and bodily autonomy. During this politically volatile time, nurses play an important role in improving their transgender and non-binary patients’ experience. This paper examines how intersectionalizing Person-Centered Care for transgender and non-binary people constitutes a social justice model that seeks to counteract institutionalized transphobia and uphold the humanity of these individuals.
Footnotes
Acknowledgment
s. This article is dedicated to all the people who have suffered maltreatment and discrimination in a medical setting, and to those whose pain was ignored. As interdisciplinary scholars, we seek to create spaces where people of color, including those who are trans and gender diverse, can thrive.
Disclosure.
The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding.
The author(s) received no specific grant or financial support for the research, authorship, and/or publication of this article.
Karla M. Padrón, PhD, (she/her/hers/ella), is an Assistant Professor of Gender Studies in the Department of Communication and Center for the Study of Women, Gender, and Sexuality at Northern Illinois University in DeKalb, Illinois.
Coralie Pederson, CNP, (she/her/hers), is a Nurse Practitioner at Boynton Health at the University of Minnesota in Minneapolis, Minnesota.