
Abstract
Introduction/Background: A study involving 48 obstetric nurses explored the relationship between self-efficacy scores and demographic variables, and family-focused care during obstetrical emergencies. Methods: Obstetric Nursing Self-Efficacy Scale scores and demographic data were collected, and the Van Gelderen Family Care Rubric (VGFCR) was administered following simulation of obstetrical emergencies. Results: Two variables were found to influence the VGFCR scores. Nursing specialty certification and previous education in family-focused care. Conclusion: Improvements in the delivery of family-focused care can be achieved with simulation education and nursing specialty certification achievement.
Each year in the United States more than three million births occur, each with unique maternal experiences. These experiences may be perceived as negative, and those perceptions may last a lifetime. Women's negative perceptions of childbirth are influenced by fear of losing control (Dunning et al., 2016; Hollander et al., 2017), concerns for the infant (Dunning et al., 2016), birth complications (Dunning et al., 2016), pain and discomfort (Dunning et al., 2016; Zhang et al., 2020), lack of family support (Zhang et al., 2020), and lack of communication and explanation by the health-care team (Dunning et al., 2016; Hollander et al., 2017; Reed et al., 2017; Zhang et al., 2020). The World Health Organization's (WHO) (2019) Intrapartum Care for a Positive Childbirth Experience prioritizes childbearing women's access to an environment that is safe and allows the family to have a sense of control with decision making.
Family-Focused Care
Historically, nurses have been taught to care for the patient, “view[ing] the family as the background of care” (Denham, 2003, p. 150). Some nurses may have lacked the knowledge necessary to provide care to the patient and family, as their education may have solely focused on the patient (Sanchez Exposito et al., 2017). Family-focused care (FFC) is when “nurses assume a mind-set that continually thinks family as they care for individuals and their families as a unit of care” (Hoehn Anderson & Denham, 2016, p. 196). Nurses’ lack of knowledge about FFC may be attributed to minimal instruction, and/or faculty members’ lack of comfort and skill in including the family, as they may have been unprepared in this skill (Eggenberger et al., 2015). When the patient is the sole focus of the nurse's care, the family's needs may not be included in care planning; this oversight may lead to increased family stress, thus negatively impacting patient and family health outcomes (Alavi et al., 2017).
Nurses are essential in identifying the needs of family during health events, helping them understand and navigate health-care interactions. Inadequate FFC can hinder positive patient experiences and care outcomes (Van Gelderen et al., 2019). FFC is essential during health events, as this approach is grounded in partnership among interdisciplinary health-care teams, patients, and families that can lead to positive family outcomes (Denham, 2003; Van Gelderen et al., 2019). FFC involves integrating the family into the patient care experience, addressing concerns, easing anxieties, supporting inquires, advocating for connectedness, and influencing health outcomes (Banergee et al., 2018; Reed et al., 2017; Swan & Eggenberger, 2021).
Historically, nurses have been taught to care for the patient, viewing the family as the “background of care.”
Simulation
Skill development via simulation has become a widely accepted and effective teaching modality to improve nursing knowledge, skills, and communication, and has been linked to improvement in FFC (Van Gel-deren et al., 2016). Simulated learning environments can improve clinical performance (Christian & Krumwiede, 2013; Nelissen et al., 2017) and ability to intervene during life-threatening concerns (Christian & Krumwiede, 2013; Nelissen et al., 2017), and enhance self-efficacy (Ehmke et al., 2021; Egenberg et al., 2017; Irby et al., 2017). Simulation that includes FFC increases proficiency and comfort with carrying out difficult conversations with families (Irby et al., 2017; Sanchez Exposito et al., 2017). The purpose of this study was to explore the relationship between nurses’ self-efficacy scores and demographic variables, and their demonstration of FFC during simulated obstetrical emergencies.
Methods
Study Design
This study employed a quasi-experimental design to measure obstetric (OB) nurses’ FFC of patients with OB emergencies as measured using the Van Gelderen Family Care Rubric (VGFCR) (Van Gelderen et al., 2019), and to determine whether nurses’ demographic data and self-efficacy as measured by the Obstetric Nursing Self-Efficacy Scale (ONSE) (Guimond & Simonelli, 2012) are predictors of VGFCR scores. Self-efficacy is the belief in oneself regarding what they can do with the knowledge they possess within the care areas where they work (Bandura, 1998).
Sample and Setting
The research was conducted at a large university in the upper Midwest, with a provisionally accredited simulation center. The university partners with health-care organizations to provide educational opportunities to their employees. A convenience sample of 48 OB nurses who worked in the regional medical center's birth center was recruited by email communication. Inclusion criteria was nurses who worked in OB at the medical center. Exclusion criteria were nurses who did not work in OB, medical providers, and advanced practice nurses.
Tools
Demographics.
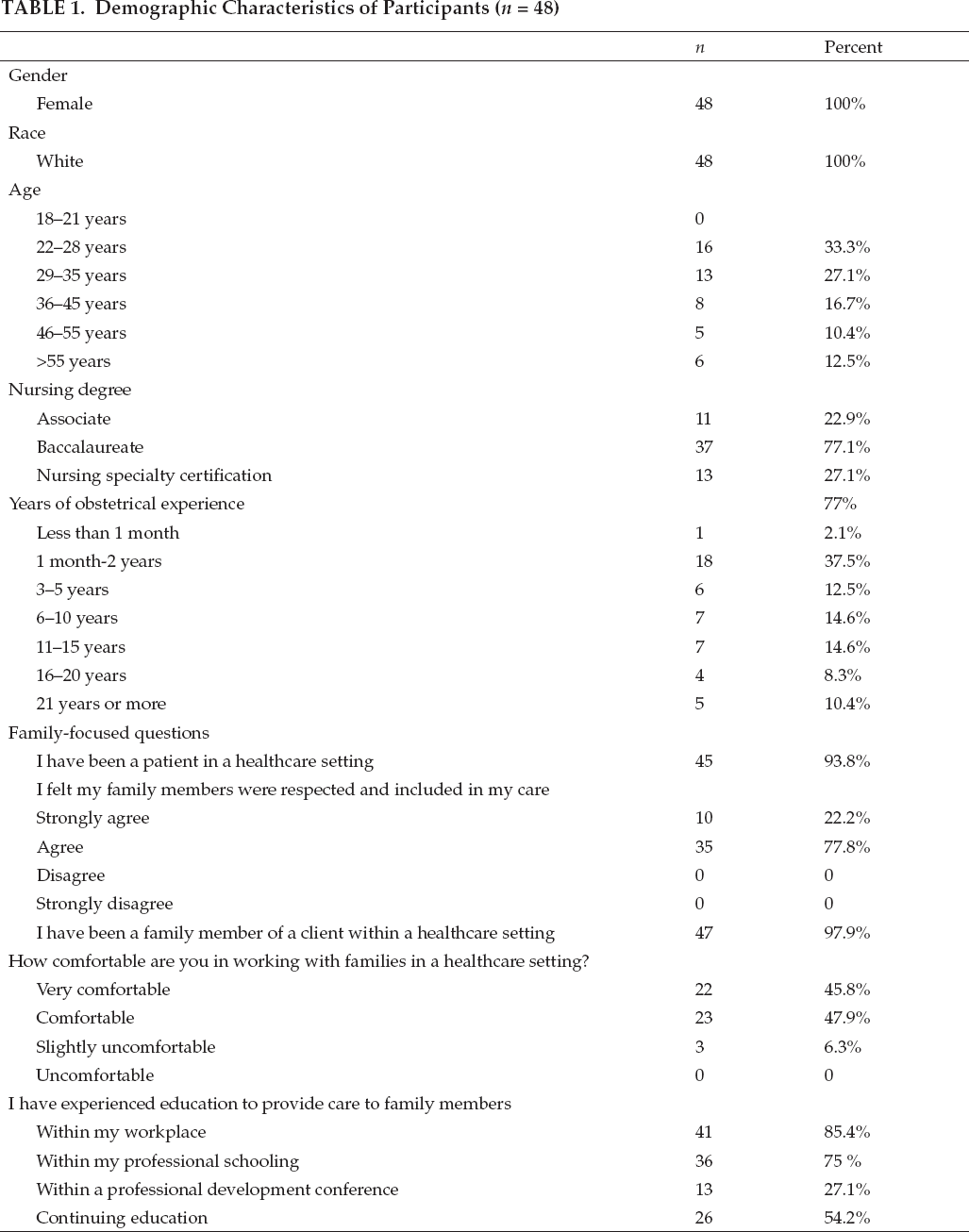
Demographic data collected included gender, race, age, nursing degree, years of OB experience, years as an RN, and FFC questions, as shown in Table 1. The variable “years as an RN” was a continuous variable, with the remaining demographic variables being categorical.
Demographic Characteristics of Participants (n = 48)
The Obstetric Nursing Self-Efficacy Scale.
The Obstetric Nursing Self-Efficacy Scale (ONSE) is an 18-question self-report tool measuring perceived self-efficacy of nursing students related to OB patient care scenarios (Guimond & Simonelli, 2012). Participants rate their self-efficacy level as completely sure (4), very sure (3), moderately sure (2), slightly sure (1), and not at all sure (0), for a possible total of 72 points. Reliability of the ONSE scale for nurses has a Cronbach's alpha of .98 (Ehmke et al., 2021).
Van Gelderen Family Care Rubric.
The VGFCR is a rubric consisting of 12 family-care constructs with three score categories; Met (3), Needs Improvement (2), and Not Met Characteristics (1), for a possible total of 36 points (Van Gelderen et al., 2019). The constructs are communication style, use of terminology, positioning, eye contact, delivery of compassionate care, summary and validation, family history collection, family health routines assessed, addressing family needs, addressing improvement, partnering with family, and addressing needs and follow up care (Van Gelderen et al., 2019). Cronbach's alpha for this tool was .845 (Van Gelderen et al., 2019).
Data Collection
After Institutional Review Board (IRB) approval, 80 OB staff nurses from the medical center who met the eligibility criteria were sent an email invitation to participate in the study; 48 nurses responded and were emailed the study consent and details of the simulation event 1 week prior to the scheduled dates, which occurred over a series of 5 days, with eight sessions to choose from. On the designated day, participants arrived at the simulation center and were provided with an iPad preprogrammed with the consent form, demographic survey, and ONSE scale. Next, participants cared for simulated OB patients while being video recorded. After the simulation was complete, three researchers viewed the recordings, evaluating the participants’ engagement in the 12 constructs of the VGFCR. All results were de-identified through the Qualtrics software. The ONSE scale and demographic data were matched to the VGFCR results by unique participant identifier numbers. Inter-rater reliability was maintained by utilizing the same three researchers to rate the practice simulation videos.
Data Analysis
Once data collection was completed, data was transferred to Statistical Package for the Social Sciences (SPSS), version 27, for further analysis. Data was coded for analysis of variance (ANOVA) and linear regression. Gender and ethnicity were found to be homogenous data and were removed from the analysis. For this study, the independent variable was the self-rated levels of self-efficacy regarding OB emergencies interventions, measured by the ONSE scale.
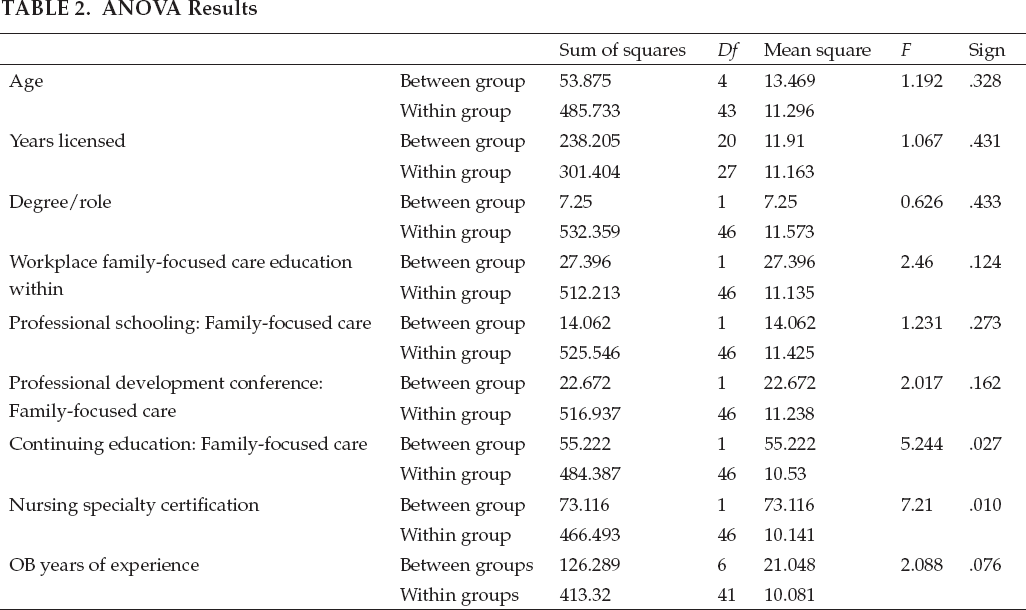
ANOVA Results
Regression Model
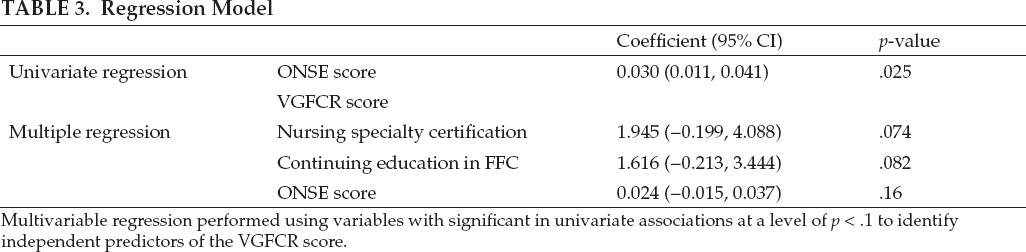
Multivariable regression performed using variables with significant in univariate associations at a level of p < .1 to identify independent predictors of the VGFCR score.
Predicting VGFCR Scores

Predictors: (Constant), nursing specialty certification, I have experienced education to provide care to family members: Within a continuing education, ONSE score.
Demographic descriptive statistics were determined for continuous variables, and percentages for categorical variables. Normality of all variables was determined by examining the Q-Q plots. An ANOVA determined the relationship between VGFCR scores, and categorical variables and simple linear regression examined the continuous variable relationships to VGFCR scores (ONSE scores, OB years of experience, and continuing education). Variables with a p value less than .05 were further analyzed via multiple regression to determine their relationships to the VGFCR.
Results
A total of 48 nursing participants (a response rate of 60%) signed consents, completed the ONSE survey, and participated in the simulation; all were able to be observed demonstrating simulated FFC.
Demographics
All participants were female and identified as white. Most (37) had a baccalaureate degree; 13 held a nursing specialty certification (e.g., Inpatient Obstetrics, Maternal Newborn Nursing, Lactation Counselor); and 26 had received continuing education in FFC. See Table 1.
Influencing VGFCR Scores
The results of ANOVA analyses indicate there were two variables that influenced the VGFCR scores: Nursing specialty certification and continuing education. The simple regression analysis using ONSE and VGFCR scores revealed a statistically significant relationship with higher ONSE scores predicting high VGFCR scores.
Multiple Regressions
Following the significant results from the ANOVAs and simple regression, three variables were entered into a multiple regressions model: Nursing specialty certification, continuing education in FFC, and ONSE scores. The results of the multiple regression model using nursing specialty certification, continuing education with FFC, and ONSE scores revealed no statistically significant predictors of VGFCR scores.
Regression Analysis
Using the enter method, ONSE score, nursing specialty certification, and continuing education were found to explain a significant amount of the variance in VGFCR scores. The 19.4% variance in the VGFCR scores was attributed to nursing specialty certification, continuing education in FFC, and ONSE. This finding highlights the important role professional development plays, through continuing education and nursing specialty certification, to develop and extend nurses’ FFC knowledge.
Discussion
The nurses’ self-efficacy in providing safe OB nursing care predicted an increase in FFC. To advance FFC nursing practice, the family must be viewed as a client and placed at the “center of the nursing perspective” (Van Gelderen et al., 2016, p. 168). FFC implemented in daily nursing practice may improve outcomes for patients and their families (Banerjee et al., 2018; Yu et al., 2017). All study participants either agreed or strongly agreed that they respected and included family in their care, and a high percentage (93.7%) self-identified as being comfortable or very comfortable in working with families. In addition, 75% reported receiving education in FFC as part of their nursing education program, and 54.2% reported engaging in continuing education about FFC. Similarly, 85.4% identified that FFC education occurred within the workplace, suggesting that family care is integrated into usual practice. Taken together, the findings support the role of FFC education in knowledge translation at the bedside (Duhamel, 2017; Swan & Eggenberger, 2021).
A birthing experience that includes an unexpected complication may have a negative impact on maternal well-being (Cook et al., 2018). An unexpected complication may be perceived as a traumatic event by the patient and family. The use of FFC simulation scenarios that center on preventing and/or intervening during an emergent OB event can support the development of a nurse's self-efficacy and FFC skill in the management of OB emergency situations (Ehmke et al., 2021; Sanchez Expósito et al., 2017; Van Gelderen et al., 2019). Increased self-efficacy may be reflected in improved care provided to birthing women and families. Reducing or mitigating traumatic experiences associated with OB emergencies may positively influ-ence care outcomes.
Implications for Practice
Health-care organizations seeking to improve patient and family outcomes may want to consider adding FFC knowledge to OB continuing education to enhance the self-efficacy of OB nurses. The study findings support that increasing OB nurses’ self-efficacy strengthens an increase in FFC. Educational opportunities, particularly simulation scenarios that incorporate family concerns, provide the ability to develop knowledge and thinking, which in turn may positively influence patient outcomes (Ehmke et al., 2021). A challenge to this perspective is that during OB emergencies, nurses may shift their focus to the emerging physiologic needs of the birthing woman, inhibiting FFC.
Health-care organizations seeking to improve patient outcomes must provide nurses with educational opportunities that advance their knowledge of family-focused care and create practice environments that give nurses time to provide it.
The study found that ONSE scores, when analyzed alone, were strong predictors of VGFCR scores; nursing specialty certification and FFC education had a relevant effect on VGFCR scores. Further research into other factors predictive of VGFCR scores could aid in developing education that builds FFC skills and self-efficacy.
The study findings support the need for ongoing education on FFC. Pre-licensure education programs and professional development via continuing education can be guided by the five competencies in the International Family Nursing Association (IFNA) Position Statement on Generalist Competencies for Family Nursing Practice: 1) Enhance and promote family health; 2) Focus nursing practice on families’ strengths; 3) Demonstrate leadership and systems thinking skills; 4) Commit to self-reflective practice; and 5) Practice using an evidenced-based approach (IFNA, 2015). Swan and Eggenberger (2021) found that early career nurses graduating from a program with a FFC curriculum incorporated family care in the usual care provided at the bedside. The findings from this study support that nurses’ gain knowledge from FFC professional development, including continuing education, nursing specialty certification, and simulation. Integrating FFC competencies and care into educational opportunities prepares nurses to manage family concerns within complex clinical situations (Swan & Eggenberger, 2021) and is associated with improved health-care outcomes (Chesla, 2010; Christian, 2018). Health-care organizations seeking to improve OB patient outcomes must provide nurses with educational opportunities that advance their knowledge of FFC and create practice environments that give nurses time to provide it (Chesla, 2010; Swan & Eggenberger, 2021). More research is needed to understand the impact on health-care organizations that emphasize FFC.
Simulation is an effective pedagogy for teaching nurses to manage OB emergencies while providing FFC. Simulation scenarios concentrated on FFC during OB emergencies enable learners to balance the patient's need for care during physical declination with the family's need for support during a crisis (Ehmke et al., 2021). When developing simulation scenarios about complex, emergent events, educators need to make sure that families are incorporated into the care, and not overlooked as nurses manage the patient's physiologic needs. Including families in these scenarios will prompt nurses to continually assess the needs of the family unit and enhance confidence and FFC skills in a safe learning environment where mistakes can be corrected (Van Gelderen et al., 2016). Effective management of emergent clinical situations while supporting the family may play a role in mitigating traumatic experiences.
Simulation scenarios concentrated on family-focused care during OB emergencies enable learners to balance the patient's need for care during physical declination with the family's need for support during a crisis.
Nurses need to appraise their personal beliefs and “develop self-reflective practices with families,” so they can navigate complex relationships and needs (Swan & Eggenberger, 2021, p. 29). Traumatic birth experiences are often associated with lack of communication and support from nurses (Hollander et al., 2017). Patient satisfaction surveys may not specifically refer to FFC, but nurses need to develop self-reflective practices with a FFC lens. FFC could be incorporated into documentation systems, enabling nurses to acknowledge the approaches they take to implement FFC. More research is needed to understand how nursing care focused on families may reduce traumatic experiences.
Limitations of Study
Despite efforts to model a familiar work environment, the simulation scenarios, involving a mannequin instead of an interpersonal experience, may have created a barrier to FFC. Utilization of a live, standardized patient may provide a more realistic care approach. The study was conducted at a single regional medical center, limiting generalizability. The convenience sample comprised subjects who were willing to complete the research, introducing selection bias. The ONSE scores may have been influenced by participants’ existing FFC knowledge and skills acquired in their nursing education.
Conclusion
FFC simulations of complex physiologic conditions enable nurses to practice skills and family interventions in a safe environment. Higher levels of FFC can contribute to improved patient experiences and to the overall health of OB patients and their families. FFC education is needed for all nurses so they can develop and apply FFC practices, to enhance positive patient outcomes and mitigate childbirth trauma and its impact on family health.
Footnotes
Disclosure
The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding
The author(s) received no specific grant or financial support for the research, authorship, and/or publication of this article.
Sabrina Ehmke, DNP, RNC-OB, NPD-BC, PHN, (she/her/hers), is an Assistant Professor in the School of Nursing at Minnesota State University, Mankato, in Mankato, Minnesota.
Stacey Van Gelderen, DNP, MS, RNC-MNN, PHN, (she/her/hers), is a Professor in the School of Nursing at Minnesota State University, Mankato, in Mankato, Minnesota.
Marilyn Swan, PhD, RN, (she/her/hers), is an Associate Professor in the School of Nursing at Minnesota State University, Mankato, in Mankato, Minnesota.
Laura Bourdeanu, PhD, NP, (she/her/hers), is a member of the online faculty at American Sentinel College of Nursing in Waterbury, Connecticut.