
Abstract
Primary care settings have many opportunities to support patients who have anxiety and/or depression, but resources are often scarce. Our faculty team developed an education tool to support mental health awareness and provide suggested wellness activities. Health-care professionals from various disciplines and settings have demonstrated eagerness to use this tool with patients and with health-care students to improve resilience and mental wellness.
Mental health care in America has primarily focused on individuals with serious mental illness. Although an estimated 4% of Americans have a serious mental illness, nearly one in five (18.9%) have some form of mental illness, with depression and anxiety being the most common (National Institute of Mental Health [NIMH], 2019). Kansas, a predominately rural state, reports an even higher rate, with 20.9% of the population diagnosed with depression (Kansas Department of Health and Environment [KDHE], 2017). Mental health care is particularly complicated in rural areas due to provider shortages and lack of resources. In rural and underserved settings, first line health-care providers often work in primary care clinics. Although primary care providers (PCPs) may wish to address mental health issues, they may be unable to offer effective support or education to patients because of limited time and resources.
Background
Faculty at the University of Kansas School of Nursing (KU SON), located in a largely rural midwestern state, have been developing educational approaches for advanced practice registered nurse (APRN) students that focus on assessment and management of health-care needs in primary care settings, particularly in rural and underserved communities. The faculty team was awarded an Advanced Nursing Education Workforce (ANEW) grant from the Health Resources and Services Administration to advance this work by providing APRN students with opportunities to experience the distinctiveness of rural primary care. In developing these educational experiences for students, the faculty team included a focus on mental health and wellness, to complement the development of primary care skills for APRN providers in rural and underserved areas. Although the project initially focused on the APRN student group, the scope later expanded to include resources that would help a range of individuals, including PCPs, educators, and community members. Ultimately, the ANEW faculty team developed a tool for self-assessment of mental wellness (see Figure 1), and a tool for planning self-care activities to promote mental wellness (see Figure 2).
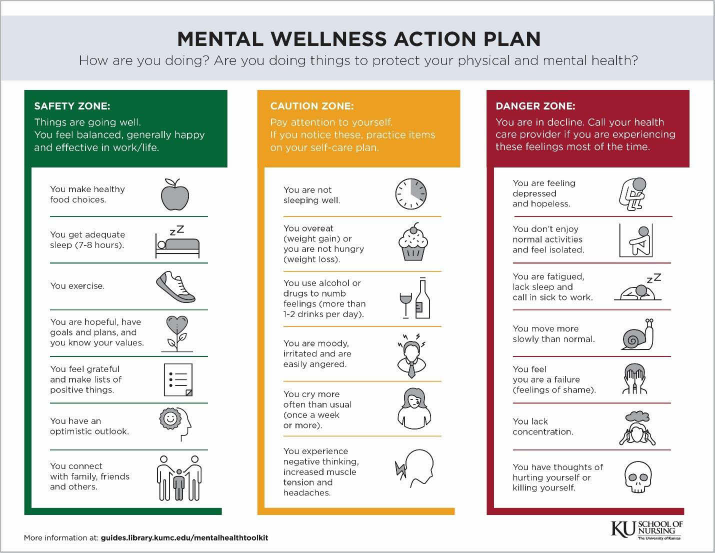
Mental Wellness Action Plan used for self-assessment. Available for download at https://guides.library.kumc.edu/ld.php?content_id=48265547.
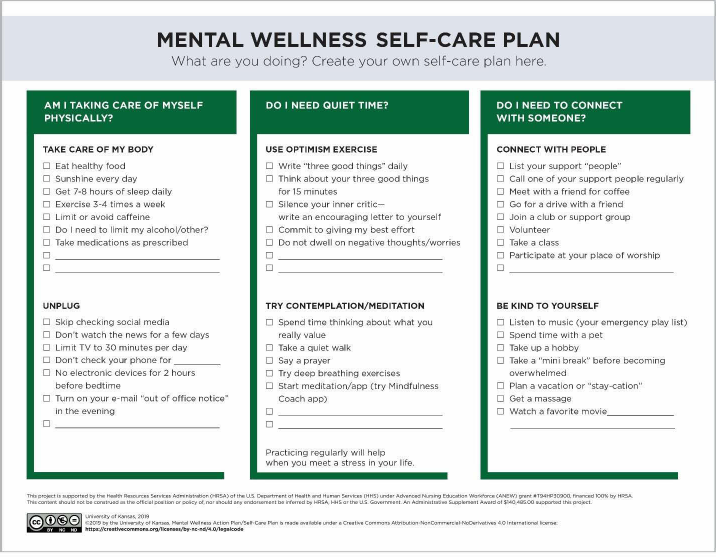
Mental Wellness Self-Care Plan to be used as inspiration to add self-care activities to daily habits. Available for download at https://guides.library.kumc.edu/ld.php?content_id=48265547.
Self-care plans are not only for chronically ill persons; anyone can benefit from taking intentional steps toward wellness.
Key Aspects of Self-Care
The need for a mental wellness toolkit was informed by the extensive practice experiences of our faculty team. The team focused on several aspects of self-care: self-care as a universal need, prevalence of chronic stress, health literacy, access to care, and fostering emotional intelligence (EI) and resilience, all self-care ideas that are supported in the literature.
Self-Care as a Universal Need
Most adults appreciate the importance of caring for self, both mentally and physically. According to Levich (2007), patients dealing with chronic illness “all self-manage, some more effectively than others” (p. 12). Levich explains that preparation for self-management is essential for patients to recognize and solve the care problems that arise over time. Any chronic disease self-management plan will recommend healthy lifestyle choices (e.g., diet, exercise, sleep, optimism, social support) as an essential part of the plan. Self-care plans are not only for chronically ill persons. Anyone can benefit from taking intentional steps toward wellness (Anekwe & Rahkovsky 2018).
Effects of Depression, Anxiety, and Chronic Stress
Globally, depression is a leading cause of disability, impacting individuals and their families, with problems commonly experienced at home, at work, or in social situations (World Health Organization, 2020). Using data collected in the United States from 2013 to 2016, Brody et al. (2018) stated that 8.1% of adults reported experiencing depression during any 2-week period. Anxiety has a similarly concerning prevalence in the United States. In a 2-year time period, 19.1% of U.S. adults reported an anxiety disorder (NIMH, 2019). Depression and anxiety are highly co-morbid disorders, with women more affected than men (Kalin, 2020). Depression also commonly co-occurs with chronic illnesses like diabetes and heart disease. For example, depression is associated with suboprimal control of disease and increased rates of end-organ complications; when patients with heart failure or diabetes develop depression, the cost for treatment is higher, and the patient often has poorer clinical outcomes (Sunha et al., 2014).
Chronic stress and sustained negative emotions, especially anger, depression, and anxiety, can prompt the onset and progression of several health issues, including heart problems; hypertension; diabetes; increased susceptibility to infections and cancerous growths; delayed healing; and exacerbation of chronic inflammatory conditions such as arthritis, atherosclerosis, and periodontal disease (Ersig & Starkweather, 2017; Salovey et al., 2000). Given the serious health consequences of prolonged, unresolved, or mismanaged stress, learning to regulate emotions supports a quicker recovery from a stress-induced reaction and is considered an important resilience factor in diminishing the overall burden of stress on the body (Salovey et al., 2000; Stough et al., 2009).
Health Literacy and Patient Education
Many Americans have difficulty comprehending or acting on health information because of basic or below-basic health literacy (Kim & Lee, 2016). Literacy deficits exist across the lifespan and in varied settings (Hahn et al., 2015; MacLeod et al., 2017; Sheridan et al., 2011). To be most useful across patient groups and to promote greater understanding, health-care education materials should be easy to read. Techniques effective for persons with lower health literacy include demonstration, and use of teaching tools with simple words and icons (Centers for Disease Control and Prevention [CDC], 2014). Teaching tools with pictures and diagrams can reinforce written or spoken health teaching.
The goal of supporting patient learning is central in developing self-care management, and helping patients recognize the importance of self-care and self-efficacy is critical to that aim. Empowering patients who have a chronic condition to improve their own self-care can benefit both patients and providers (Levich, 2007). However, as in other rural regions, most Kansans rely on primary care to manage acute and chronic physical and mental health conditions across the life span. The complexity of providing health-care information tailored to each patient is a strain for PCPs in rural and underserved areas (Bergh et al., 2015). Providers need patient education resources that can be used to promote self-care among patients with chronic conditions.
Access to Care
Most rural and underserved areas have shortages of primary health-care and mental health providers that compound the challenges of health-care access (CDC, 2017; Rural Health Information Hub, 2018). People living in rural and underserved areas often have longer distances to travel for health care and social services (CDC, 2017), compared to their urban counterparts. Unavailability of transportation, lack of insurance, and competing responsibilities are additional issues that may impede care for those with limited resources, no matter where they live.
Many rural and underserved communities rely on PCPs and clinics to deliver mental health services. However, primary care practices often are not well equipped to handle the complex psychosocial and behavioral needs of their patients, due to time and resource limitations. Self-care may be even more imperative in provider-scarce areas such as rural Kansas. Harwood and L'Abate (2010) note that patients living in rural areas, where there typically are few mental health professionals, may particularly benefit from self-help resources. Overall, PCPs in rural clinics need more tools to support mental health care.
Supporting Emotional Intelligence and Resilience
EI is defined as the ability to understand and control one's own feelings, and to understand the feelings of others and react to them in a suitable manner (Por et al., 2011; Raghubir, 2018). People with high EI and the ability to manage their feelings tend to rebound more quickly from stressful situations and events (Bennett et al. 2018; Salovey et al., 2000). Patients with high EI skills tend to follow their self-care plans and to cope more effectively during illness (Zysberg, 2018). Another benefit of EI is improved insight and judgment, which may reduce high-risk behaviors such as smoking, drinking, drug use, and gambling (Dev et al., 2018; Stough et al., 2009).
Self-awareness is an important attribute in mental wellness, success in work and family life, and following a healthy lifestyle. People who are self-aware can usually identify emotions as they happen, are sure of their own boundaries, have a positive outlook on life, and demonstrate good psychological health (Arnott et al., 2018; Salovey et al., 2000). These attributes contribute to resilience, that is, moving through emotions and moods more quickly. Resilience enables people to thrive when facing adversity, and can be a target for maintaining or improving mental health (Davydov et al., 2010).
Mental Wellness Tools
Development of Tools
With these key self-care issues in mind, our team created a mental wellness action plan handout as part of a mental health toolkit. The structure of our handout was based on an asthma action plan developed by the American Lung Association (2019), with colored zones to assist in gauging wellness. In the asthma plan, a green zone means “doing well,” a yellow zone means “caution,” and a red zone means “get help now.” Patients typically welcome the straightforward approach of an asthma action plan, which is easy to understand and supports self-care questions.
The ANEW team adapted the asthma action plan template structure to mental health. In the mental health adaptation (Figure 1), the green column is labeled a “safety zone,” representing a healthy, well-balanced, and positive lifestyle. The yellow column is labeled a “caution zone,” with stress-related symptoms evident. The red column is labeled a “danger zone,” and includes indicators of personal distress and dysfunction. The symptoms outlined in the red zone are consistent with questions related to symptoms of depression as measured by the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001), that is, lack of interest in activities, feeling down, difficulty sleeping, decreased feelings of self-worth, and negative thoughts. Formal screening for depression should be done in a health-care setting with a valid, reliable screening tool such as the PHQ-9. After appropriate screening has been completed, the mental wellness action plan is meant to be used as a tool for teaching and self-evaluation in primary care settings. The use of green, yellow, and red columns provides a color spectrum structure that is familiar to patients and providers.
Given the serious health consequences of prolonged, unresolved, or mismanaged stress, learning to regulate emotions supports a quicker recovery from a stress-induced reaction and is considered an important resilience factor in diminishing the overall burden of stress on the body.
The reverse side of the mental wellness action plan document provides recommendations for mental wellness self-care that can be used to build a self-care plan (Figure 2). For example, the first (and probably most important) aspect of the self-care plan focuses on a healthy lifestyle. This section includes exercise, sleep, exposure to sunshine, and healthy food choices. The second column offers additional recommendations for achieving personal quiet time, defining values, using positive thinking, and expressing gratitude. The last column includes suggestions for social interactions and self-care strategies that may improve connectedness and empathy. The aim of the mental wellness self-care plan is to encourage individuals to consider personal goals, while implementing behaviors and developing habits to improve overall health and wellness.
Dissemination of the Mental Wellness Action and Self-Care Plans
The mental wellness action plan and self-care documents are available through the University of Kansas academic medical center's open access library resource listing (Icenogle et al., 2019). In this online location, a brief message accompanies the action and self-care plans, and outlines possible uses of the tools in primary care. The mental wellness action and self-care plans can be used as an interactive tool and teaching aid to increase patients ‘awareness of their present emotional state; as a “prescription” for a self-care activity; or for personal goal setting. Ideally, a teach-back process with the patient would be used to help solidify understanding and commitment to participating in an activity identified as a short-term goal. These teaching tools can be shared by a provider, nurse, social worker, occupational therapist, health educator, chaplain, or other interprofessional team members.
As the mental wellness action plan and mental wellness self-care plan were distributed to APRN students and faculty through training sessions, there was interest and enthusiasm for using the handout with other groups and in other settings. For example, the plan is being used with undergraduate nursing students to build awareness of self-care; in the medical center's campus counseling office; with personal coaching by a licensed clinical social worker; and in home care settings. Multiple primary care and specialty care clinics at the academic medical center are using this tool with persons living with chronic illness. Additionally, staff and providers in a skilled care nursing facility and behavioral health nurses have found the document a helpful tool to use with adults and older adults. Several school nurses have requested the mental wellness plan to use with students. The tool is used in telehealth visits by a psychiatric/mental health nurse practitioner, and could be incorporated into tele-health primary care visits and placed on a patient portal. Health-care professionals have shared that the tool is well received by users.
Discussion
In this era of pandemic, PCPs must be mindful of the increased anxiety and fear associated with the coronavirus, and the impact on individuals ‘baseline ability to cope. Even though the mental wellness action and self-care plans were developed prior to COVID-19, they may prove to be helpful resources during this unprecedented time, when needs are especially great while access to resources is limited. The plans may be useful in meeting providers ‘needs for easily accessible resources. The action and self-care plans were developed with a focus on the needs of residents in rural Kansas communities; they may not translate to patients in other regions or with more diverse racial or cultural backgrounds. As these documents are shared more widely, plans for improvement include a Spanish language version and a formal assessment of readability (Coleman et al., 2017).
Because of space limitations of a single-page document that can be readily shared with patients, students, and providers, the wellness plan does not include all possible assessment or self-care options. Future modifications to the Mental Wellness Action Plan and Mental Wellness Self-Care Plans can address a broader audience, with attention to language, cultural sensitivity, and determinants of health such as systemic racism (Kwate & Goodman, 2015). Another potential modification of the Mental Wellness Self Care Plan is adding space for the user to write their personal goals. The act of writing a goal demonstrates intention, while making progress toward goals usually increases feelings of competence.
With the rapid expansion of telehealth during COVID-19, clinicians need educational resources that work well in a virtual platform. Education delivered via videoconferencing to patients with chronic diseases is an effective alternative to standard, clinic-based approaches (Kearns et al., 2012; Rush et al., 2018;
Patients dealing with chronic illness all self-manage, some more effectively than others.
Conclusion
Achieving and maintaining mental health and wellness is a challenge for many individuals. Health promotion and prevention of both mental and physical illness and disability are key responsibilities for PCPs. In rural and underserved areas, the limited time and resources available to many PCPs provide challenges that can be difficult to overcome. Fostering a patient self-care approach can support primary care efforts to promote health and wellness. Self-care is an approach that supports health-seeking behaviors and a mindset that includes optimism, meaningful connections, and resilience. Having resources such as the Mental Wellness Action Plan and Mental Wellness Self-Care Plan can facilitate the work of PCPs in encouraging patients to develop healthy lifestyle habits including mental and physical wellness self-care, reflection, and social interaction, which can lead to improved health outcomes and more meaningful and productive lives. The process our faculty team used to create and share these tools demonstrates an efficient means of adapting an effective self-assessment mechanism from one area (an asthma action plan) to a new area (mental wellness). These new products are intended to be helpful resources for PCPs, particularly in rural and under-served communities.
Footnotes
Acknowledgment
s. A special thanks to Edward Hunter, PhD, ABPP, Division of Psychology, for his support and insights and to Carla Deckert, Project ECHO Director, who also encouraged this work.
Mary Icenogle, RN, BSN, (she/her) is the Advanced Nursing Education Workforce Grant Project Manager at the University of Kansas School of Nursing (KU SON). Mary previously worked as the Nurse Manager at the KU SON faculty practice in Kansas City, Kansas.
Cara A. Busenhart, PhD, APRN, CNM, FACNM, (she/her) is a Clinical Assistant Professor and the Program Director for Advanced Practice & Midwifery Education Programs at the University of Kansas School of Nursing. She provides care to underserved patients in Kansas City, Kansas as a Certified Nurse-Midwife.
Carol Buller, DNP, APRN, FNP-BC, GNP-BC, (she/her) is a Clinical Assistant Professor and the Program Coordinator for the Adult-Gerontology Primary Care Nurse Practitioner program at the University of Kansas School of Nursing. She provided care to underserved adult and older adult patients in the faculty practice clinic.
JoAnn M. Peterson, DNP, APRN, FNP-C, WHNP-BC, (she/her), is a Clinical Assistant Professor and the Program Coordinator for the Family Nurse Practitioner program at the University of Kansas School of Nursing. She provides care to underserved patients in a safety net clinic.
Lori Schwartz, DNP, APRN, FNP-BC, (she/her), is a Clinical Assistant Professor in the Family Nurse Practitioner program at the University of Kansas School of Nursing. She provides clinical services in an urgent care setting.
Lucinda Whitney, DNP, APRN, PMHNP-BC, (she/her), is a Clinical Assistant Professor and the Program Coordinator for the Psychiatric-Mental Health Nurse Practitioner program at the University of Kansas School of Nursing. She provides residential treatment to underserved youth and telemental health services to rural and underserved patients in Southeast Kansas.
Cynthia Teel, PhD, RN, FAAN, (she/her) is a Tenured Professor, Associate Dean for Academic Affairs, and Project Director for the Advanced Nursing Education Workforce Grant, awarded by Health Resource and Services Administration, all at the University of Kansas School of Nursing.
Disclosure. The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding. This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number T94HP30900 Advancing Nursing Education Workforce for $1,243,677. The information or content and conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the U.S. Government.