
Abstract
This study aimed to describe the impact of mutuality, anxiety, and depression on quality of life (QoL) in patients with heart failure (HF) using cross-sectional, convenient, and consecutive sampling. A total of 97 patients were recruited. Sociodemographic and clinical variables and self-report measures of anxiety, depression, mutuality, and QoL were collected. The results highlighted the pivotal role of mutuality (specifically the domain of shared values between patients and their caregivers) in determining perceptions of physical health. Conversely, depression was a negative determinant of perceptions of both physical and mental health. Future research is needed to describe in-depth and longitudinally the associations between mutuality and QoL in patients with HF.
The description of the quality of life (QoL) and its determinants in patients with heart failure (HF) are strategic for developing tailored nursing care plans for supporting and educating patients and their care-givers (Wang et al., 2016). Patients ‘psychological burdens, such as anxiety and depression, are described as important determinants of QoL in HF populations (Celano et al., 2018). Recent evidence shows that the positive quality of relationships between patients with HF and their caregivers, defined as mutuality, is a positive strategic modulator of the patients ‘self-management behaviors (Vellone, Dellafore, et al., 2018). However, beyond the role of patients ‘psychological burdens – particularly anxiety and depression – no studies have investigated the predictive performance of mutuality on QoL in patients with HF (Dellafore et al., 2019). This gap undermines the possibility of framing comprehensive knowledge of the role of each determinant in modulating QoL. This study provides the first evidence of the specific contribution of mutuality, anxiety, and depression in determining QoL in patients with HF.
Background
HF, a chronic condition affecting more than 26 million people worldwide (Savarese & Lund, 2017), is a clinical syndrome that leads to typical symptoms (e.g. breathlessness, ankle swelling, and fatigue) and/or signs (e.g., elevated jugular venous pressure, pulmonary crackles, and peripheral edema) as the result of structural and/or functional cardiac abnormality, resulting in reduced cardiac output and/or elevated intracardiac pressures at rest or during stress (Ponikowski et al., 2016). Prevalence of HF ranges from 1.2% to 6.6% in people aged 66–85 years (Danielsen et al., 2017). Overall, the ageing population and improved survival rates among patients with myocardial infarction are the main causes of the increased prevalence of HF (Ponikowski et al., 2016). Although significant improvements have been achieved in medical treatments of HF over the last 10 years, these patients still present with a wide range of psychological burdens, such as anxiety and depression (Celano et al., 2018).
Both anxiety and depression negatively affect daily living activities, as well as the physical symptoms of HF (Dellafore et al., 2019a). Anxiety is a sense of doubt and vulnerability about the future, and depression is a sense of sadness, with a loss of interest in daily living activities (Celano et al., 2018). Anxiety and depression have been described as prevalent in patients with HF, associated with the development and progression of the disease (Celano et al., 2018). A meta-analysis of eight studies found that depression led to a two-fold increased risk of negative outcomes, such as death or cardiac events (Rutledge et al., 2006). Associations between anxiety and negative outcomes are less clear (e.g. no available meta-analysis); however, several studies highlight an association between the longitudinal trajectory of anxiety in patients with HF and negative outcomes (Friedmann et al., 2006; Pelle et al., 2010).
Currently, the challenge of clinical management of patients with HF is not only to improve survival rates and medical treatments but also to improve patients ‘QoL (Moradi et al., 2019). QoL is a complex, subjective, multidimensional concept that includes physical, emotional, and social well-being as well as functional ability (Post, 2014). Patients ‘QoL is influenced by several factors, such as self-care, socio-economic status, family or social support, and health literacy (Audi et al., 2017). Assessment of QoL is pivotal in designing care plans for patients with HF and for their caregivers (Garin et al., 2014). Recent research highlights that the caregiver contribution to supporting patients with HF (particularly mutuality) is theoretically an important factor influencing patients ‘QoL, that needs to be empirically explored (Dellafore et al., 2019a). Evidence suggests that the dyadic relationship between patients with HF and their caregivers is highly important for disease self-management in achieving the best clinical outcomes (Vellone, Chung, et al., 2018).
Mutuality is defined as the positive quality of the relationship between patients and their informal care-givers, encompassing four dimensions that explain the nature of their relationship: love and affection (e.g., attachment felt toward the patient/caregiver), shared pleasurable activities (e.g., enjoying time spent together), shared values (e.g., agreeing on views and perspectives), and reciprocity (e.g., comforting each other) (Vellone, Chung, et al., 2018). Research on mutuality shows interesting effects in modulating behaviors and QoL: Higher mutuality decreases aggressiveness in patients with dementia (Ball et al., 2010), and improves QoL in stroke survivors (Ostwald et al., 2009). Overall, higher mutuality improves the recovery process (Park & Schumacher, 2014). Recent evidence in different cohorts of patients with HF suggests that mutuality has an influence on patients ‘self-management behaviors, anxiety, and depression (Dellafore et al., 2019; Vellone, Dellafore, et al., 2018). However, the specific contribution of mutuality, anxiety, and depression on modulating QoL is largely under-investigated in patients with HF (Vellone, Dellafore, et al., 2018). This implies that clinicians ‘and researchers ‘understanding of the specific role of anxiety, depression, and mutuality in determining QoL in patients with HF is still weak, undermining the development of evidence-grounded educational and supportive interventions. This study aimed to describe the impact of mutuality, anxiety, and depression on QoL in patients with HF.
QoL is a complex, subjective, multidimensional concept that includes physical, emotional, and social well-being as well as functional ability.
Materials and Methods
Design, Setting, and Sample
This is a cross-sectional, single-centre study using a real-world, convenience, and consecutive sampling. The study was performed in an outpatient HF clinic in the north of Italy. Inclusion criteria were: Diagnosis of stable chronic HF, recent cardiac assessment (maximum 1 week before enrolment), and able to read and speak Italian. Exclusion criteria were: Diagnosis of cognitive decline, age under 18, and inability to read and speak Italian. Although this study used real-world sampling, the exclusion criteria were necessary to ensure that participants were able to complete the self-report questionnaires for data collection. The clinical cardiac assessment had to be performed in accordance with current European guidelines (Ponikowski et al., 2016)
Measurements
Clinical and socio-demographic characteristics were collected from medical records in accordance with previous research aimed at determining self-report outcomes in patients with HF (Vellone, Chung, et al., 2018). Clinical characteristics were: ejection fraction (EF), months from diagnosis of HF, New York Heart Association (NYHA) classification, etiology, and comorbidities. Socio-demographics included sex, marital status, occupation, and education.
Mutuality was measured using the Italian version of the Mutuality Scale (MS) (Dellafore, Buck, et al., 2018), a 15-item instrument measuring the quality of the patient/caregiver relationship in four dimensions: Love and affection, shared pleasurable activities, shared values, and reciprocity. Each item of the MS uses a 5-point Likert scale for responses, ranging from “not at all” (0) to “a great deal” (4). Scores range between 0 and 4 in each domain; higher scores indicate higher mutuality.
QoL was assessed using the Italian version of the Short Form-12 (SF-12) (Kodraliu et al., 2001). SF-12 is a shorter version of Short Form-36 (SF-36), showing good validity in measuring the physical and mental components of health (PCS and MCS, respectively). Both PCS and MCS are scored between 0 and 100, where higher scores indicate stronger perception of health.
Anxiety and depression in patients and caregivers were assessed using the Italian version of the Hospital Anxiety and Depression Scale (HADS) (Costantini et al., 1999). The HADS, commonly used by researchers to determine levels of anxiety and depression in different settings, consists of 14 items in two subscales: the HADS-A to measure anxiety and the HADS-D to measure depression. Each item of the HADS uses a Likert scale ranging from 0 to 3; each score for the two subscales can range from 0 to 21.
Ethical Considerations
The Institutional Review Boards of the involved centre approved the study protocol. The protocol was designed to be consistent with the ethical standards indicated by the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) and Good Clinical Practice (GCP). Patients received information about the study before they signed the written informed consent.
Statistical Analysis
The sample characteristics were synthetized using descriptive statistics. Missing data were managed using a pairwise deletion, eliminating information when the particular data point needed to perform a specific test was missing. Multiple linear regression (MLR) for the multivariable analysis was used to assess determinants of QoL. Independent variables of the MLR models were identified considering both previous descriptions of QoL determinants in patients with HF and bivariate analysis (Bursac et al., 2008; Vellone, Dellafore, et al., 2018). Independent variables were included in regression models if they were associated with the outcome (MCS12 or PCS12) at p ≤ .20 (Bursac et al., 2008). Independent variables were assessed for possible collinearity using a preliminary evaluation through correlation analysis (Dormann et al., 2013). The regression coefficients were standardized. The independent variables were entered into the models simultaneously (i.e., block inclusion). Signifcance was set at α = 5%, where null hypotheses were two-tailed. Statistics were performed through Statistical Package for the Social Sciences (SPSS) version 22 (IBM Corporation).
Results
Sample
A sample of 97 patients with HF was enrolled (see Table 1).
Socio-Demographic and Clinical Characteristics of the Sample (N = 97)
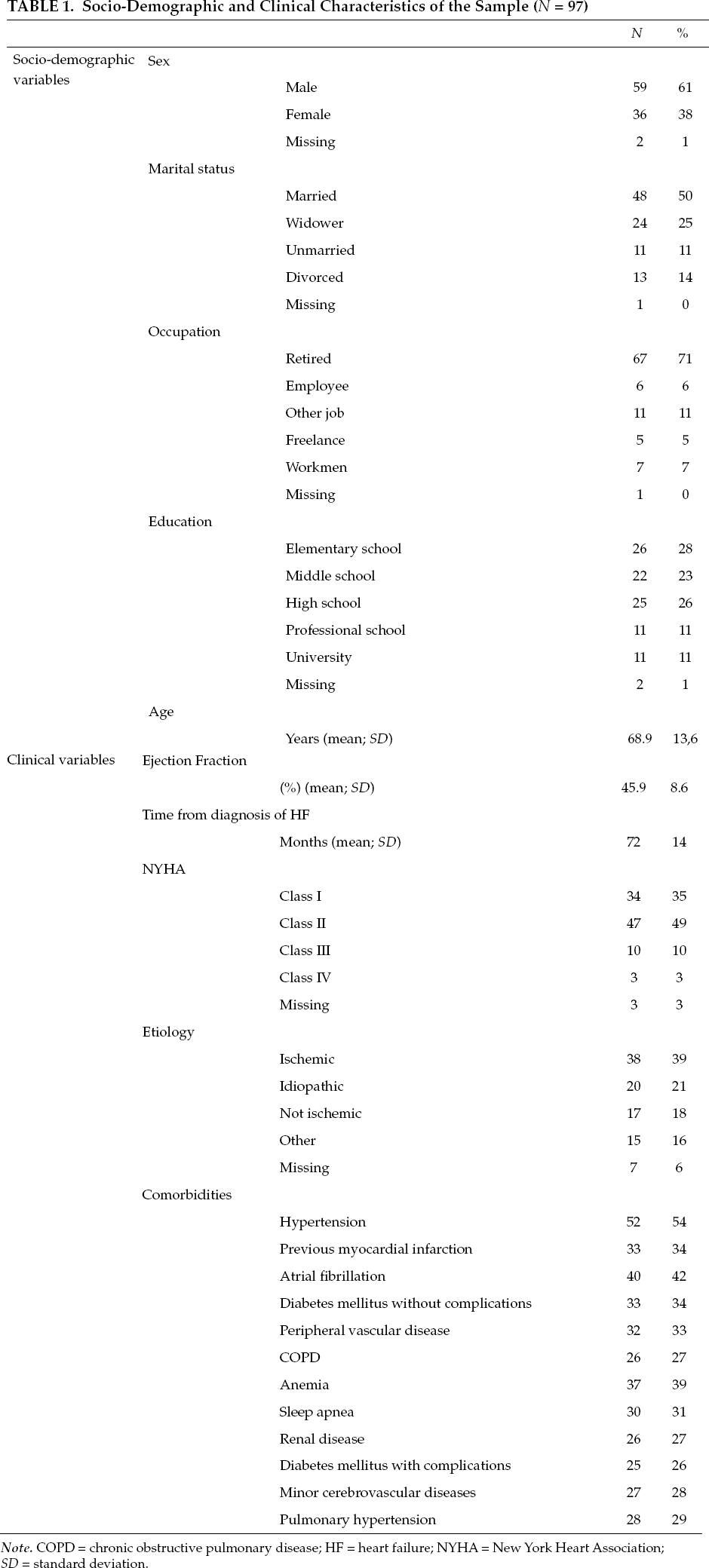
Note. COPD = chronic obstructive pulmonary disease; HF = heart failure; NYHA = New York Heart Association; SD = standard deviation.
Mutuality, Qol, Anxiety, and Depression
Table 2 reports the scores for the four dimensions of mutuality from the MS. For anxiety and depression from the Hospital Anxiety and Depression Scale, and perceived physical health (PCS12) and mental health (MCS12) from the Short Form-12.
Descriptive Statistics of Self-Report Measurements
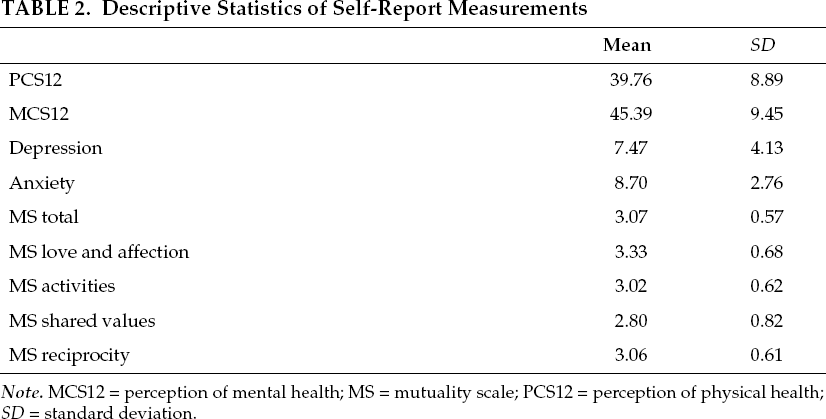
Note. MCS12 = perception of mental health; MS = mutuality scale; PCS12 = perception of physical health; SD = standard deviation.
Table 3 shows determinants of the levels of perceived physical and mental health as reported on the SF-12.
Determinants of Perceived Physical and Mental Health
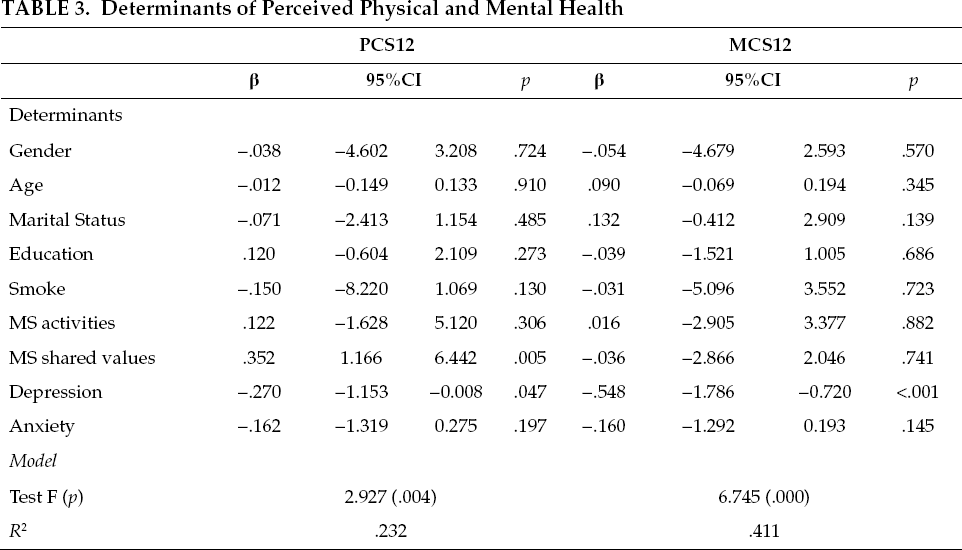
Bivariate analysis between PCS12 and depression and anxiety showed significant negative correlations (i.e., respectively: r = -.297; p = .003; r = -.243; p = .017). The remaining variables, including those in Table 1 did not show significant correlations with PCS12.
Bivariate analysis between MCS12 and sociodemographics and clinical variables showed correlations similar to the PCS12. Depression and anxiety scores significantly decreased when patients reported higher MCS12; MS “shared values” was significantly positively associated with MCS12. The remaining variables, including those in Table 1, did not show significant correlations with MCS12.
Determinants of Pcs12 and Mcs12
As Table 3 shows, the model describing the determinants of PCS12 was adequate to explain the proportion of variation in the response data. MS “shared values” and depression were significant determinants of PCS12; “shared values” made a higher contribution to the positive variance of PCS12 than the negative contribution given by depression. The model describing the determinants of MCS12 was adequate as well. The only negative determinant involved in explaining the variance of MCS12 was depression. No positive determinants were found.
Although significant improvements have been achieved in medical treatment of HF, these patients still present with a wide range of psychological burdens, such as anxiety and depression.
Discussion
To the best of our knowledge, this study was the first description of the specific contributions of mutuality, anxiety, and depression to modulating perception of physical health and perception of mental health as major components of QoL. This research is useful considering that the goal of treating patients with HF is not only to increase survival rates but also to improve QoL (Polikandrioti et al., 2019). Beyond recent significant improvements in medical treatments, patients with HF experience a wide range of physical and psychological symptoms with an impact on their QoL (Dellafore, Arrigoni, et al., 2018; Dellafore et al., 2019; Rutledge et al., 2006). The comprehension of specific contributions of each determinant of QoL helps to frame updated knowledge to address educational and supportive care, in accordance with previous evidence about diverse cardiac diseases (Flocco et al., 2018, 2019).
The main novelty arising from this study was the association between “shared values,” which is a domain of mutuality, and perception of physical health: Patients having a high propensity to share values with their caregivers show a more positive perception of physical health. The domain of “shared values” measures whether patients and their informal caregivers are aligned regarding the meanings of aspects of their life. Accordingly, the domain of “shared values” seemed to act as a proxy indicator for the quality of the patient/caregiver relationship by positively influencing QoL. Further, the positive contribution of “shared values” in determining the perception of physical health was stronger than the negative contribution of depression in explaining the variance of PCS12. This result suggests several implications for designing patient care plans in which enhancing mutuality could have important effects on perceptions of physical health, rather than focusing exclusively on treating depression.
The efficacy of educational interventions for improving mutuality and specifically shared values should be empirically tested since previous research was aimed at describing the relationship between QoL and clinical outcomes such as mortality and rehospitalization (Erceg et al., 2019), perception of pain, depression, and anxiety (Celano et al., 2018), with very little about the contribution of mutuality to QoL (Vellone, Dellafore, et al., 2018).
Clinical Scenario
A 76-year-old man came to the clinic with ankle swelling, chest pain, weight gain, and shortness of breath, accompanied by his son, who was his caregiver. The patient's anamnesis was well-known to the clinic: reduced left ventricular systolic function with an ejection fraction = 46% (ultrasound performed two months ago), treated with angiotensin-converting enzyme inhibitors and diuretics in the last 12 months. The clinical presentation (from NYHA II to NYHA III and signs of fluid retention) and the lab values (B-type natriuretic peptide = 501 pg/mL; N-terminal pro-B-type natriuretic peptide = 3798 pg/mL) suggested an exacerbation of HF. After two days of hospitalization to adjust therapy (adding diuretics and beta-adrenergic receptor blockers), symptoms were relieved, and the patient appeared ready for discharge. The clinical nurse specialist assessed his anxiety and depression using the HADS, his QoL using the SF-12, and mutuality of the patient and his caregiver using the MS, to design an education plan. Anxiety and depression scores were 9 and 8; PCS12 and MCS12 were 38 and 46, MS total = 3, MS love and affection = 4, MS shared values = 2; MS reciprocity = 3. Considering the current scenario, the clinical nurse specialist interviewed the patient and caregiver to explore which aspects showed misalignment of views. The nurse found that the caregiver had not focused on the need to support adherence to diuretics regularly and that he and the patient often discussed their different perspectives about the necessity of the therapy. Therefore, the nurse prioritized educational interventions for aligning the views between patient and caregiver to improve the shared values of mutuality before planning specific interventions for depression and anxiety.
The dyadic relationship between patients with HF and their caregivers is highly important for disease self-management in achieving the best clinical outcomes.
Limitations
This study has some limitations. The design was cross-sectional, without reference to the trajectory of QoL and its determinants over time. Other behavioral variables, such as health literacy and engagement, might have an influence on both QoL and mutuality. The participants were a convenience sample of Italians, so caution is required in interpreting the inferential results. The main strengths of this study were the consecutive sampling, minimizing selection bias, and the use of valid, reliable, and theoretically-grounded tools to measure self-reported variables.
Conclusion
Understanding the determinants of QoL has the potential to identify the most susceptible modifiable aspects that can improve QoL as well as other outcomes. This study highlighted the pivotal role of mutuality in determining higher scores of perception of physical health, especially the role of shared values between patients and their caregivers. This aspect could be susceptible of improvements through specific education programs aimed to enhance mutuality. For this reason, clinicians should take into account the quality of the patient/caregiver relationship, and researchers should empirically demonstrate through longitudinal data collection and cross-national studies that structured education can enhance mutuality, as a positive influence on QoL.
Footnotes
Acknowledgments
We wish to thank all the study participants.
Disclosure. The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding. The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the IRCCS Policlinico San Donato no specific award grant.
Federica Dellafore, PhD, RN, (she/her), is a researcher at IRCCS Policlinico San Donato (Italy). She holds a PhD in Nursing Science and Public Health from the University of Rome Tor Vergata.
Cristina Arrigoni, RN, MSc, (she/her), is a professor of Nursing Science at University of Pavia. Her research focus is mainly public health.
Francesca Palpella, RN, MSc, (she/her), has a strong clinical background in cardiovascular care. She holds a Master of Science degree in nursing. She is currently a tutor in the undergraduate nursing education of University of Milan.
Alberto Diazzi, RN, BSN, (he/him), is a clinical nurse at at IRCCS Policlinico San Donato.
Marilena Orrico, RN, BSN, (she/her), is a clinical nurse at IRCCS Policlinico San Donato.
Arianna Magon, RN, MSN, PhD, (she/her), received her doctorate in Nursing Science and Public Health at the University of Rome Tor Vergata. She is currently a research nurse at IRCCS Policlinico San Donato.
Francesco Pittella, MSN, MBA, (he/him), is the director of undergraduate nursing education at IRCCS Policlinico San Donato.
Rosario Caruso, PhD, (he/him), is the director of Health Professions Research and Development Unit at IRCCS Policlinico San Donato. He holds a PhD in Nursing Science and Public Health from the University of Rome Tor Vergata.