
Abstract
The novel coronavirus disease (COVID-19) pandemic as a public health emergency poses dramatic challenges for healthcare systems. The experiences of health-care workers are important in planning for future outbreaks of infectious diseases. This study explored the lived experiences of 14 nurses in Tehran, Iran caring for coronavirus patients using an interpretative phenomenological approach as described by Van Manen. In-depth interviews were audio-recorded between March 10 and May 5, 2020. The essence of the nurses ‘experiences caring for patients with COVID-19 was categorized as three themes and eight subthemes: (a) Strong pressure because of coronavirus: initial fear, loneliness, communication challenges, exhaustion. (b) Turn threats into opportunities: improvement of nursing image, professional development. (c) Nurses ‘expectations: expectations of people, expectations of government. The findings of this study showed that identifying the challenges and needs of health-care providers is necessary to create a safe health-care system and to prepare nurses and expand their knowledge and attitudes to care for patients in new crises in the future.
The novel coronavirus (COVID-19) was first reported as a global concern in Wuhan, China, and then spread rapidly around the world, becoming a public health emergency (Novel, 2020). Currently, as of June 10, 2020, more than 200 countries around the world have people infected with the coronavirus (World Health Organization [WHO], 2020). According to the latest statistics, as of 27 August 2020, above 20 million people wordwide have been diagnosis with coronavirus and almost 736,000 have died (WHO, 2020). In Iran, with a population of approximately 84 million people, as of 27 August 2020, 367,896 have been infected and 21,137 have died (Iranian Ministry of Health and Medical Education, 2020). The high rate of pathogenicity and infectivity of coronavirus has led to fear and anxiety in affected countries, not only among the general population but also among healthcare professionals, especially nurses who are in close contact with coronavirus patients (Duan & Zhu, 2020). Patients infected with coronavirus need holistic nursing care for a variety of physical and mental needs (Wu et al., 2020). Nurses, as the largest workforce in health care, play an important role in providing information and physical and psychological support to patients in critical situations. Nurses actively promote care of patients and family members care due to their pivotal role in the health-care team. They are also the coordinators of care and predictors of needed services (Kim & Choi, 2016).
Due to the high rate of infectivity and pathogenicity of this virus, nursing care for patients with COVID-19 is very demanding and requires high standards. Working in high-risk conditions in direct contact with confirmed patients, isolation, lack of adequate personal protective equipment (PPE), and lack of sufficient and clear information are among common nursing stressors (Kang et al., 2020). In addition, nurses are under ethical pressure to care for patients who may be a risk to their own health and safety (Kim & Choi, 2016). Reviews of studies on nurses ‘experiences with new infectious diseases such as severe acute respiratory syndrome (SARS), influenza A virus subtype H1N1 (H1N1), and Middle East respiratory syndrome (MERS) showed that lack of accurate information about the disease and inadequate PPE has caused nurses to experience high levels of stress (Lancee et al., 2008; Tam et al., 2004). A study of the long-term effect of caring for patients with SARS reported that health professionals experienced high levels of posttraumatic stress syndrome (PTSD) 13–26 months after the incident (Maunder et al., 2006). A study in Wuhan, China, on the psychological impact of the coronavirus on health-care workers found that frontline health workers, especially nurses, reported a high psychological burden (Lin et al., 2020). However, the experiences of nurses in different countries vary according to culture, religion, health-care system, and nursing resources (Kim, 2018). Therefore, it is necessary that the experiences of nurses caring for patients with coronavirus in each country be explored according to the local sensitivities of that country. Awareness of nurses ‘experiences, as the largest group in the treatment team, will help prepare the health-care system for future crises. Where there is a necessity to understand the specific phenomena accurately, qualitative research is beneficial. The study of phenomenology is used to accurately understand the essence and meaning of human experiences in a particular context (Beck, 2020). The current study aimed to explain the lived experiences of nurses in the care of patients with coronavirus in order to create a comprehensive description of this care and to understand the intrinsic structure of this phenomenon.
Methods
Study Design
This qualitative study used Van Manen's (2016) phenomenological method to explore the following research question: “What was the meaning of nurses ‘lived experiences of caring for coronavirus patients?” Van Manen's approach is based on the hermeneutic phenomenological tradition, the study of a person's lived experience (the person's reality, as it is immediately experienced in the world). The findings of phenomenological research reveal an understanding of the moment, so that persons who have had or could have had that experience can recognize it (Van Manen et al., 2016).
Participants
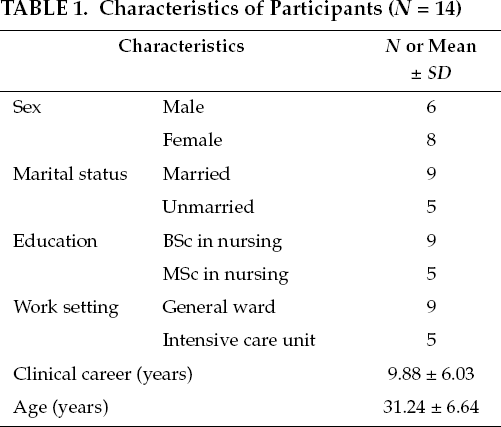
Participants were 14 nurses from five general hospitals in Tehran, Iran, selected based on purposive sampling with maximum variation according to the inclusion criteria (care for a patient with coronavirus, and willingness to participate in the study). See Table 1 for demographics. Participants were added until theoretical saturation was reached, and no new essential meaning could be derived from participants ‘statements.
Characteristics of Participants (N = 14)
Ethical Consideration
The study was approved by the Research Ethics Committee of Tehran University of Medical Sciences (No.IR.TUMS.VCR.REC.1399.020). Informed consent for participation was obtained from all participants. All responses were kept confidential and only used for the study purpose. Participants had the right to withdraw from the study voluntarily.
Data Collection
One-to-one in-depth recorded interviews of 30–60 minutes were conducted from March 10 to May 5, 2020. First, the researcher explained the purpose of the study, then asked the main question, “What kind of experience did you have while caring for Coronavirus patients?” Later, following questions such as “Can you explain more”? Or “Can you give an example?” were asked. The interviews were transcribed, along with description of nonverbal movements such as laughter, crying, silence, and sighs.
Data Analysis
Van Manen's approach was used for data analysis (2016). Since this approach makes the tradition of
The findings of phenomenological research reveal an understanding of the moment, so that persons who have had or could have had that experience can recognize it.
Paying attention to the nature of lived experience.
Obtaining descriptions about the lived experience through investigating the phenomenon as it is lived, not as it is conceptualized.
Engaging in thematic analysis through reflecting on the essential themes which characterize the phenomenon.
Engaging in phenomenological writing to describe the phenomenon via the art of writing and rewriting.
Establishing and maintaining a strong and oriented relation to the phenomenon.
Creating coherence and balancing the context by considering the parts and the whole (Van Manen, 2016).
Thematic statements were isolated using first the holistic reading approach (considering each interview as a whole and describing its essential meaning or main concept in several sentences), then the detailed reading approach (reading the transcript several times, selecting sentences or expressions related to the aim of the study). Thematic statements for each interview transcript were isolated, reworded, and labeled in order to develop primary themes, and the developed themes grouped into primary categories. The primary themes were frequently revised, overlapping or common themes were combined, unrelated themes were deleted, and essential themes were identified. In other words, expressions, sentences, and paragraphs of each interview were independently classified into themes and sub-themes based on their commonalities. A total of 354 primary themes were identified. After combining or deleting similar or overlapping themes, primary themes were categorized into three themes and eight subthemes.
Trustworthiness
Guba and Lincoln's (1989) criteria of credibility, transferability, dependability, and conformability were used to establish the trustworthiness of this study (Guba & Lincoln, 1989). Credibility was confirmed by having the participants review the descriptions of their respective interviews to ensure that the transcripts conveyed the correct message. Transferability was reached by providing rich in-depth descriptions of the lived experience. Dependability was verified by another researcher who followed the process of the study and the findings without contradiction. For conformability, all of the original research data, including verbatim drafts and data analysis records, were stored safely for future verification and reference.
Results
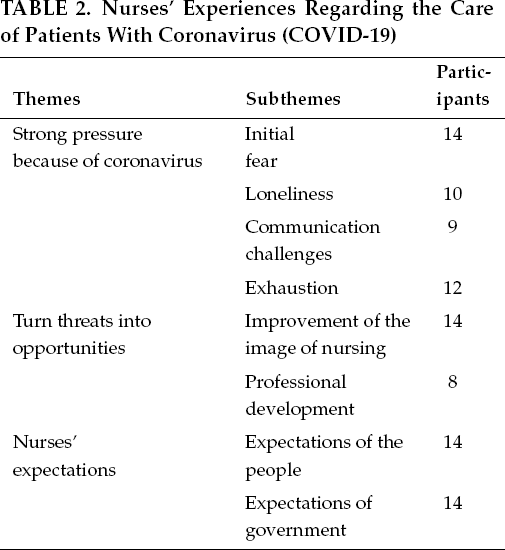
The themes that emerged from the study data are all about nurses ‘experiences of caring for patients with coronavirus and are based on the purpose of the study, which is to deeply understand and describe nurses ‘experiences in this field. Eventually, with the integration of the themes, three main themes and eight sub-themes emerged (Table 2).
Nurses ‘Experiences Regarding the Care of Patients With Coronavirus (COVID-19)
Strong Pressure Because of Coronavirus
This theme is one of the main themes of the coronavirus patient care phenomenon, and shows that nurses were under a lot of physical and mental pressure in caring for patients with coronavirus for various reasons. Its subthemes include initial fear, loneliness, communication challenges, and exhaustion.
“We wear white so that you do not have to wear black.” This sentence widely circulated in social media, and can be very effective in society and a positive sign for the future of nursing.
When the coronavirus entered Iran, there was a public fear throughout the country. When I got to the hospital, I was totally scared. It was as if I was done with life, and I felt like I was going to get sick and die.
On the first day of work, when I found out that my patient had coronavirus, after going back home, I cried all my off day, lest I get sick and transfer the virus to my family. Because I really didn't know much about it, and I thought I would get infected if I came to direct contact with the patient.
When I saw Chinese nurses on TV who were quarantined, I had no idea that it would happen to me. But now, I haven't seen my 6-year-old daughter for 35 days. My wife and daughter have gone to my mother-in-law's house, and I can't see them for now because of working with coronavirus patients.
It's really hard to communicate with these patients because I wear goggles, and I can't have good eye contact with them. The mask and shield don't allow the patient to see our face, and they only identify us by the name tag. Sometimes they don't even know if a nurse is a male or female.
Because patients have coronavirus, I can't stay with them long. Talking with a mask also makes me short of breath and, I can't communicate verbally with them as I do with other non-coronavirus patients, and that upsets me a lot.
This white coverall with a head cover and goggles, an N95 mask, and gloves are really hard to bear. I feel choked and sweat so much that I'm completely dehydrated after each shift.
A nurse with work experience in the intensive care unit, who had cared for coronavirus patient for 45 days, said,
When patients are transferred to the intensive care unit, it means their respiratory condition worsens. Seeing patients in these conditions and seeing the deaths of our compatriots has really had a negative effect on my mood. The emotional burden of this problem may be more severe than the disease itself, and it made the treatment team really tired.
When the crisis peaks and death strikes, a lot of people escape, but the nurses stay face-to-face with death and dance with it.
Turn Threats into Opportunities
Another major theme of the study was turning the threat into opportunities. Participants stated that although the coronavirus caused negative effects such as fear, pathogenicity, and mortality, the threat has served as an opportunity to change society's view of the nursing profession, improve nursing roles in various fields, and learn new scientific subjects. Sub-themes include improvement of the image of nursing and professional development.
During the night shift, when I was preparing the medicine, one of the patients told me that we were the bravest people of the time. This made me proud of myself as a nurse. Also, one of our nurse colleagues wrote on the back of her white coverall and posted on Instagram: “We wear white so that you do not have to wear black.” This sentence widely circulated in social media and can be very effective in society and be a positive sign for the future of nursing.
During this time, I received many messages from people. The family of one of the recovered coronavirus patients had sent a letter of appreciation to the nurses in the ward, writing that when the crisis peaks out and death strikes, a lot of people escape, but the nurses stay face to face with death and dance with it. This sentence made me feel that nurses are appreciated and are visible in society.
I've always worked in quite stable conditions, and almost no crises like this has occurred. We had several crisis management meetings at the hospital, and I'm sure that after this experience, my managerial vision will become broader.
Other comments included:
All members of the treatment team, the doctor, the nurse, the radiologist, and the lab are all working together to beat coronavirus and I have never really seen such an inter-professional collaboration in the health system.
It was a new experience in my life. The patients I work with, each have their own care, medications, and treatments that I haven't faced before. I've learned many things, and it can be useful for me in the future.
Coronavirus patients are among the most oppressed patients who don't have a companion or someone to visit them. They're all very scared. Even when they die, their families can't say goodbye to their deceased. They can't have a funeral for them. I feel they are more vulnerable than other patients, and I try to support them in every way I can.
Nurses ‘Expectations
In addition to their round-the-clock efforts in the hospital, the participants had a number of expectations of people, and of government.
Working conditions are very difficult, and it'll be harder if people don't cooperate. We expect people, by staying at home, and observing personal health and social distancing, to help us and not let the treatment staff's effort be in vain.
I expect the authorities to support us in this situation. Well, it can be financial or promotion in the work system.
The government must stand by the treatment system so that they don't feel alone. It should also provide us with enough equipment. And fully enforce quarantine conditions by enacting laws.
Discussion
This study was conducted to gain a deep and comprehensive understanding of the meaning of caring for coronavirus patients with a phenomenological approach. The results of an analysis of interviews conducted on nurses ‘experiences in caring for patients with COVID-19 showed positive and negative experiences in the care process led to their growth as nurses.
The theme that emerged first was strong pressure because of coronavirus. Coronavirus was a novel infectious disease that spread rapidly in Iran and caused public fear in the community and the health system. Participants found the care of these patients risky and challenging. The fear and stress experienced by nurses are similar to that of nurses who cared for patients with SARS (Maunder et al., 2006), or MERS in Saudi Arabia (Khalid et al., 2016) or South Korea (Kim, 2017). In the current study, nurses who were in direct contact with confirmed cases were upset by the distance from family and social isolation, as people considered them coronavirus carriers. A study on the care for patients with SARS found that poor social support from family, friends, and officials caused significant burnout among nurses (Kim & Choi, 2016; Lee et al., 2010). A study by Kim similarly showed that nurses felt frustrated due to isolation and distance from family (Kim, 2018). In addition, participants suffered from physical and mental fatigue due to long working hours, wearing PPE, and witnessing the critical condition of patients. The results of studies showing nurses ‘experiences with patients with H1N1, SARS, and Ebola were consistent with the current study in terms of emotional and physical fatigue (Lam & Hung, 2013; Smith et al., 2017; Tiwari et al., 2003).
As time passed and fear and anxiety subsided, participants described the coronavirus as a threat that provided an opportunity to grow and improve the image of nurses in society by providing high-quality services and fulfilling their responsibilities in this national crisis. With the coronavirus crisis and a global focus on nursing capabilities, it was an appropriate time to improve the status and visibility of nurses. In a study that measured the experience of South Korean nurses during the MERS outbreak, nurses had a variety of conflicting emotions, including fear, stigma, and embarrassment, and ultimately feelings of pride for performing their tasks successfully (Kim, 2018). The final emerged theme was the nurses ‘expectations of people and of government. In this regard, a study conducted in Saudi Arabia on the concerns of health professionals about MERS patient care reported that in addition to being provided with PPE, they need training, psychological support, and encouragement to enhance their morale (Abolfotouh et al., 2017). Similarly, a study in China that examined the psychological needs of the nurses caring for COVID-19 patients showed that nurses needed existence, relatedness, and growth (Yin & Zeng, 2020).
Emerging pandemics are always a possibility. Therefore, it is important to train and support nurses to deal with new and unknown health challenges and to create practical programs based on the valuable experiences of health-care providers. To this end, focus on identified problems based on nurses ‘experiences is needed to improve mental health interventions, coping strategies, and the health-care system.
It is necessary to specifically understand the problems and demands of health-care providers in order to establish a safe health-care system that can respond effectively in case of future disasters.
Conclusion
The current study was conducted to identify the experiences of the nurses caring for coronavirus patients. It is necessary to specifically understand the problems and demands of health-care providers in order to establish a safe health-care system that can respond effectively in case of future disasters. Support programs and practical and operational training are an appropriate way to create the necessary preparedness to deal with the crisis.
Footnotes
Fatemeh Bahramnezhad, PhD, is an assistant professor in the Nursing and Midwifery Care Research Center, Spiritual Health Group, Research Center of Quran, Hadith and Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Parvaneh Asgari, PhD Candidate, is a PhD candidate in nursing education in the School of Nursing and Midwifery at Tehran University of Medical Sciences, Tehran, Iran.
Disclosure. The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding. The study was approved by the nursing and midwifery care research center of Tehran university (No.99-1-100-47238).