
Abstract
Discussing racism is challenging for nurse educators and nursing students, because White privilege and racial inequities are deeply embedded and normalized in our societal structures. Avoiding the topic of racism in nursing education renders White supremacy invisible and serves to perpetuate racial discrimination and disparities in health care. Nursing education has the potential to train both faculty and students to recognize and dismantle oppressive attitudes, structures, and practices that have led to negative health outcomes for patients. Equipping nurse educators with the tools to understand and address White supremacy as well as to educate themselves and their students about antiracist language, self-care, and patient care is an important step toward promoting health and creating an antiracist society.
Race is one of the most significant determinants of success in life, not because of any genetic or biological factor, but because of racism. Oluo (2018) defines racism as prejudice against someone because of their race when that prejudice is reinforced by systems of power. In health-care education, race is often discussed as a factor that contributes to health inequities and chronic conditions. In June 2000, at the public announcement of the completion of the working draft of the Human Genome Project, lead scientists declared the construct of biological “race” invalid and unsupported by any genetic or scientific evidence (Mohsen, 2020). Race is a social construct that has been used historically to establish and perpetuate hierarchies of power and oppression. Centuries of racist policies, laws, and practices have created systemic, or institutionalized, racism that has contributed to poverty, mass incarceration, redlining and mortgage discrimination, the achievement gap in primary and secondary education, and disparities in health and health care.
Discussions of racism continue to be challenging because White supremacy continues to be a societal norm. By avoiding the topics of racism, white advantage, and White privilege, educators contribute, intentionally or unintentionally, to the maintenance of White supremacy. The immensity of institutional racism is often blamed for causing injustice and suffering, yet attributing injustice to an institution allows individuals to deny personal responsibility for accepting it and failing to confront it (Hobbs, 2018). Educators ‘ability to teach the values and positive interactions they want health-care workers to promote depends on their ability to overcome taboos and begin a dialogue about racism (Harvey, 2017). Integrating images of Black, Indigenous, and Persons of Color (BIPOCs) into lecture slides or using a mannequin with dark skin in a simulation does not in itself teach students to value diversity or practice antiracism. Nursing students should be taught about determinants/drivers of health through their entire nursing education. When social determinants of health are applied in multiple courses and woven through nursing curricula, students gain deeper understanding of the impact that social determinants have in health and illness. Education must include discussion of disparities and their impact on health outcomes. These can be difficult topics to teach, especially if talk about racism is considered unacceptable or is prohibited, and health-care educators often discuss disparities and inequities without directly addressing their roots in White supremacy. When nurse educators teach students about determinants of health, maternal mortality rates, and illnesses such as end stage renal disease and hypertension that have outcomes affecting patients differentially by race, they must address racism, White supremacy, and oppression rather than framing race as a contributing factor in inequitable treatment and outcomes. Educators must make a commitment to learning and teaching the truth that racism, oppression, and white privilege have as great an impact on health as biology and genetics.
Cultural (Un)Intelligence
Over the past few decades, health-care education has begun to place an emphasis on cultural intelligence (Hultsjo et al., 2019), defined as “an individual's ability to recognize the rules of an unknown social environment, and then to absorb them and apply them effectively in a new culturally diverse environment” (Barzykowski et al., 2019, p. 3). Both as a nursing student and as a nursing instructor, I strove to develop new ways to consider and present cultural ideas, practices, and beliefs about pain, diet, communication, and body language. Available tools were often highly stereotyped by ethnicity: some taught that African American patients did not feel pain as acutely as European American patients, and that Asian and Asian American patients, as well as Hispanic/Latinx patients, prefer to endure and suffer through pain without medication (Sabin, 2020). Cultural competency charts in nursing education have historically lumped together groups whose belief systems vary widely. Although indigenous people are not a monolithic group, generic lists of what they consider culturally sensitive have been presented to nurses for decades. True cultural sensitivity can only be achieved by learning, unlearning, and teaching about each culture from its own perspective, and nurses should be taught to treat each person as an individual by asking about their individual needs and personal preferences.
Colorblindness
Colorblindness refers to a strategy, historically practiced by White people, to regulate any appearance of prejudice or racism during social interactions by avoiding the subject of race entirely (Apfelbaum et al., 2008). Practicing colorblindness is harmful and unjust. As early as age 5, children recognize and understand that various groups possess different social statuses and are treated differently (Harvey, 2017). Noticing differences is part of healthy neurological development; racial colorblindness damages children's ability to embrace equity and distorts their engagement with and interpretation of reality (Harvey, 2017). Children who are trained to be colorblind may be unable to recognize or consider differential treatment by race because such training is incompatible with the brain's normal development and function. Colorblind racial attitudes (e.g., denying or minimizing racism in society) correlate with the inability to have racially just and equitable conversations (Johnson & Jackson Williams, 2015). Colorblindness upholds the racial status quo, inhibits efforts to promote health equity, and undermines efforts by health-care providers, healthcare educators, and leaders to develop strategies to dismantle racially colorblind practices and beliefs (Cunningham & Scarlato, 2018). Diversity education is inadequate if it does not address the unique issues faced by White people who struggle to overcome ingrained colorblindness as they embrace antiracist beliefs and behaviors.
White Advantage/Privilege
From the 1930s through the 1970s, W. E. B. Du Bois wrote about a psychological wage, which he labeled “White-skin privilege,” that enabled poor White people to feel superior to poor Black people (Du Bois, 1962). The concept of White privilege was further defined in 1988 by Mcintosh, who explained that being White did not so much confer privilege as that being non-White meant, in many cases, being without rights (Mcintosh, 1988, 2015). Hobbs (2018) describes White privilege as an unearned advantage affording White people benefits based on their skin color, and states that disadvantage caused by racism is often cloaked in invisibility, so it is difficult to recognize (Hobbs, 2018). White privilege perpetuates a lack of privilege for non-White individuals in social systems in which racist laws and policies are entrenched (Hobbs, 2018). Learning about privilege entails reflecting on how the advantages one has had in life have contributed to one's opinions and actions. Being intentional about recognizing advantages and disadvantages linked to White privilege, and teaching students to do the same, is crucial to undermining the strong societal tendency to regard Whiteness as “normal” and members of other racial groups as inferior, an example of the destructiveness of White supremacy (Harvey, 2017).
Tone Policing
Tone policing may be difficult to spot. It is a tactic that dismisses the ideas being communicated when they are perceived to be delivered in an angry, frustrated,
Educators must make a commitment to learning and teaching the truth that racism, oppression, and White privilege have as great an impact on health as biology and genetics.
Noticing differences is part of healthy neurological development; racial colorblindness damages children's ability to embrace equity and distorts their engagement with and interpretation of reality
Tone policing distracts from the speaker's intended messages by focusing on the tone of the delivery rather than the content of the message, thus allowing the distractor to establish their power in the conversation (Campbell, 2018). It is most often used by individuals holding privilege (e.g., able-bodied White heterosexual males) to prevent marginalized individuals or groups from exposing and sharing their experiences of oppression (Oluo, 2018). Such policing reinforces White supremacist norms that dictate how BIPOCs are supposed to act and, in so doing, keeps BIPOCs disempowered. BIPOCs often face unspoken judgment for not conforming to White norms, expressed through facial expressions or body language (Saad, 2020).
Tone policing in nursing education might take the form of a faculty member chastising a BIPOC student for “sounding angry” while discussing test results. It might be evident if White students roll their eyes when a BIPOC speaks loudly on a cellphone, or when a clinical instructor tells an African American student speaking African American Vernacular English (AAVE) to speak in standard English. Microagression is a statement, action, or incident regarded as an instance of indirect, subtle, or unintentional discrimination against members of a marginalized group (Microaggression, n.d.). Tone policing, implicit and explicit bias, and microaggressions are powerful, and often unintentional, forms of discrimination that constantly drain the psyches of BIPOCs (Saad, 2020; Wong et al., 2014). To avoid confronting tone policing or microagressions by people with White privilege, many BIPOCs subconsciously and preemptively tone police themselves.
Integrating Antiracism into Nursing Education
Nursing students are taught that communication is crucial and that words matter; however, these lessons generally focus on the nurse-patient relationship and the performance of caregiving tasks. Communication that uses appropriate and respectful words and terms is a valuable tool that allows nurses to provide optimal and holistic care. Constructive conversations should explicitly explore and address White supremacy and racism (Harvey, 2017).
White nurse educators should not rely on non-White educators to provide racial equity and antiracism education. BIPOCs may find it difficult to talk to White people about racism; they may fear that White listeners will become defensive, or may even feel obligated to comfort them or assuage their sense of guilt for prospering in a White-dominated society (Caporuscio, 2020). Antiracism is not a goal but a journey that must be taken by all together. The harmful assumptions and practices of racism have existed for centuries; identifying, acknowledging, and changing them will take time as well. Mistakes will be made, but with a concerted commitment to self-awareness and learning, and with curricula and teaching strategies focused on antiracism, nursing educators can counteract oppressive structures and beliefs to promote a more just, healthy, and equitable society.
Antiracism in Clinical Settings
The clinical component of nursing education should also incorporate consideration of racism, which requires clinical instructor training and accountability. Non-White nursing students may witness or experience tone policing or other forms of racism in clinical settings and/or while caring for patients. Students who have been taught about racism in the classroom have been offered the ability to recognize it and will have constructive tools for addressing it in the clinical setting.
Reflection on experiences and self-reflection are common learning tools in nursing education. It is critical that nursing faculty, clinical instructors, and students reflect on differential privileges they have experienced, and on how lack of such privileges affects the health and well-being of underprivileged populations. Mcintosh's “Unpacking the White Privilege Knapsack” is a reflective exercise that can be assigned in nursing foundations courses to help students see invisible privilege and oppression; its primary goals are to help health-care providers understand how clients ‘lives are influenced by societal disadvantages and advantages, encourage a new understanding of oneself, and increase empathy toward clients (Mcintosh, 2015).
Antiracism work in nursing academia.
Antiracist Language in Scholarly Writing
In addition to formats for citation and referencing, The Publication Manual of the American Psychological Association (APA), 7th edition (2020) contains guidelines on the use of bias-free language for researchers and writers. Attention to these guidelines is important, as the authors warn that “[l]ong-standing cultural practice can exert a powerful influence over even the most conscientious writer” (APA, 2020, p. 131). For example, the use of the term “Caucasian” as an alternative to “White” or “European” is discouraged because it originated as a way of classifying White people as a race to be favorably compared with other races (Turner, 2020). When referring to non-White racial and ethnic groups collectively, it is most appropriate to use terms such as “people of color” or “underrepresented groups” rather than “minorities” (Turner, 2020). Nurse educators should teach and utilize correct terminology in lectures, assignments, and papers (Turner, 2020).
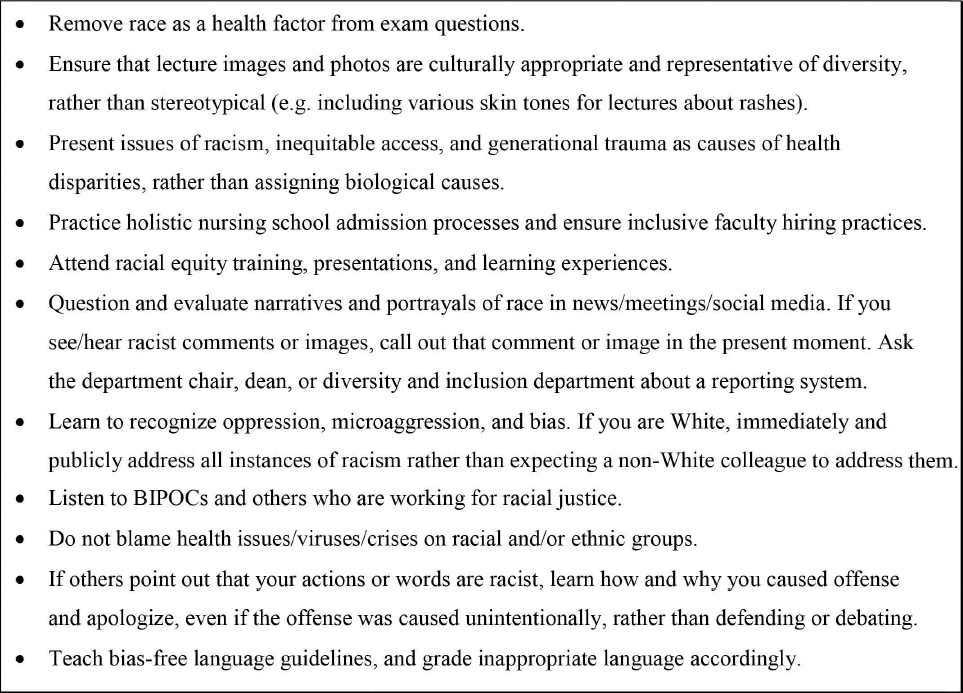
Actionable Antiracism in Nursing
Figure 1 is not an exhaustive list of antiracism work in nursing academia, but a starring point in rooting out White supremacy.
Conclusion
In a society built on White supremacy, in which racism has a profound negative impact on health and wellness, creating health equity forces us all to notice color. Education about social inequities, systemic racism, White supremacy, and social determinants/drivers of health is an essential component of nursing education. These topics must be discussed and reflected on if future nurses are to be equipped with tools to assess, diagnose, plan, and implement health care for people who have experienced the consequences of oppression and racism. As nurses and nurse educators, we need to invite conversation and reflection, even when (perhaps especially when) we feel we lack answers or do not know the right way to begin (Harvey, 2017). To improve health and wellness, and to provide holistic care, nurses must become adept at recognizing the presence and effect of racism and oppression. Educators and nurses are uniquely placed to develop policies and practices aimed at creating justice and dismantling systemic inequities.
Health-care professionals (and health-care systems) cannot embrace the values needed to reduce health disparities if they are governed by prohibitions against open and honest discourse. It is imperative that nursing educators (a) participate in programs that expose systemic racism and promote racial equity, (b) participate in self-reflection, (c) actively embrace learning opportunities, and (d) commit themselves to endorsing and advancing antiracist efforts. Healthcare education must take a firm and enthusiastic role in ending the silent and invisible attitudes and structures of racism that have plagued society for so long. It is time to actively and openly talk about racism.
Footnotes
Amie M. Koch, DNR FNP-C, RN, ACHPN (she/her), is an assistant professor at Duke University School of Nursing in Durham, North Caroline, where she teaches wellness, evidence-based practice, palliative care, and community health. Dr. Koch is a family nurse practitioner providing community-based palliative care. For over two decades she has been an activist practicing social justice work.
Disclosure. The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding. The author(s) received no specific grant or financial support for the research, authorship, and/or publication of this article.