
Abstract
The author, James C. Burroughs II, is Chief Equity and Inclusion Officer at Children's Minnesota, one of the largest freestanding pediatric health systems in the United States. This article presents the structure of a thriving Equity and Inclusion (E & I) Department as well as stories of their successes, culminating in practical suggestions for organizations wishing to develop their own E & I departments and/or initiatives.
As the Chief Equity and Inclusion Officer of a large metropolitan hospital, I'd like to invite you to participate in a thought experiment: Imagine you were starting a health-care organization to address the health needs of young people. Let's call it Children's Minnesota. The goals of the hospital are to provide equitable care for all its patients and families and deliver excellent tertiary and quaternary care that focuses on health equity and positive health outcomes for all. You wouldn't go without a Chief Operating Officer (COO), because you care about the efficient, effective, and cost-effective operations of your organization. You wouldn't go without a Chief Medical Officer (CMO), because you know that a medical staff needs someone at the executive level to understand and serve their specific needs in order to hold them accountable for delivering healthy outcomes. You wouldn't go without a Chief Human Resources Officer (CHRO), because you care about the experience and engagement of your employees, and you know that how your organization is staffed makes a key difference in how it performs. So the question becomes clear: Do you care enough about equity (making sure you're running an organization that is fair, impartial, and just) and inclusion (making sure you're running an organization where everyone feels they are valued and respected and their ideas are heard) to ensure that your organization performs well on those two metrics? Should your organization recognize equity and inclusion as metrics? Should you have a Chief Equity and Inclusion Officer? That role could be just as important as the COO, CMO, and CHRO are to the success of your health-care system.
In health care, we should put the needs and concerns of patients and families before anything else. The COO, CMO, and CHRO in your organization are all trying to improve certain metrics. What gets measured gets done. Leaders in all departments should have an eye toward improvement. These leaders will have better success with it when there is also someone—ideally a team that is formalized, focused, and funded— actively seeking to improve the experience of the entire workforce through equity and inclusion (Glover Blackwell et al., 2017).
At Children's Minnesota, one of the largest freestanding pediatric health systems in the United States, more than 50% of our patients and families are Black, LatinX, Asian, or Native American, but our patient-facing caregiver population is 93% white. We must intentionally put systems in place to recruit and retain a racially diverse group of employees and partners, so that our pool of qualified job applicants, our staff of caregivers, and the people who help build and maintain our infrastructure better reflect our patients and families.
The stated vision of Children's Minnesota is “to be every family's essential partner in raising healthier children” (Children's Minnesota, 2020). We will be living our vision when everyone feels they can bring their full selves and their full family to a system that delivers high-quality care—and where outcomes are not impacted by racism. We must eliminate policies and practices in which white supremacy and systemic racism are embedded.
We must intentionally put systems in place to recruit and retain a racially diverse group of employees and partners, so that our pool of qualified job applicants, our staff of caregivers, and the people who help build and maintain our infrastructure better reflect our patients and families.
Calling it what it Is
James Baldwin wrote, “Not everything that is faced can be changed, but nothing can be changed until it is faced” (Baldwin, 1962/2010, in Kenan, p. 42). At Children's we think it's important to use terms such as systemic racism and white supremacy because Baldwin is right: if we don't face such things without employing euphemisms, we cannot change them. Let's not word-smith it. Let's identify it, call it what it is, and change it.
The Aspen Institute defines structural racism as “a system in which public policies, institutional practices, cultural representations, and other norms work in various, often reinforcing ways to perpetuate racial group inequity” (Aspen Institute, 2016). Structural racism is embedded in our historical, political, cultural, social, and economic systems and institutions. It systematically disadvantages people of color and has a negative impact on all marginalized populations. According to Glover Blackwell et al. (2017), structural/institutional racism produces racial inequity and adverse outcomes for people of color (e.g., health, wealth, careers, education, infrastructure, and civic participation), as well as unfair and unjust practices (policies) that limit participation and prosperity of people of color.
It's not surprising, when starting a position like mine, to discover organizational policies and practices in place that result in inequitable care, either because they naively sought to be “color-blind”— purporting to promote equity without considering the reality of current race-based inequities (Kendi, 2019)— or because they failed entirely to take into account a diversity of races and cultures. These policies and practices are “white centered.” As we dismantle systemic racism and promote equity, we do that through making sure our patients and families are getting care that takes into account their race, ethnicity, religion, gender, gender identity, and any other signifiers of who they are as people. Healing is advanced through human connection, and connection is not established when those caring for patients and families fail to see, acknowledge, and accommodate the fullness of who they are. Equity is giving each patient, family, employee, vendor, and partner what they need to be successful and have an amazing experience as our “essential partner.”
I'm inspired by a quote by Dr. Martin Luther King Jr.: “[We] fear each other because [we] don't know each other, and [we] don't know each other because [we] don't communicate with each other …” (King, 1962). I would add the caveat that communication is never achieved by talking at someone; communication implies communion—a sense of being with the other person, being in something together. Data shows that Black patients do better with Black doctors and other Black caregivers (Corbie-Smith et al., 2002), so we're making efforts to have our employee population look more like our patient population. When you have caregivers who reflect the population you serve, the quality of care tends to become more comprehensive and holistic. Those clinicians understand the patients ‘cultural norms; they know how to communicate with patients and families—how to develop relationships; they know how to partner with families of color.
My 8-year-old daughter has sickle cell anemia and is a frequent visitor in the Hematology Department at Children's. It matters that our physician, Dr. Stephen Nelson, understands us. He is able to solicit input from me and engage me in a culturally relevant way. Although Dr. Nelson is white, he communicates with us and helps build the relationship, which builds trust, and that trust provides an essential foundation for quality care. [Editor's Note: Dr. Nelson is the author of “Race, Racism, and Health Disparities: What Can I Do about It?” in Creative Nursing Vol. 22 Issue 3,Caregiver Determinants of Health.] We also have a patient advocate who focuses on working with patients with sickle cell disease. She is African American. She has a son who has sickle cell disease. She gets us and understands us culturally. When culturally competent communication isn't happening—no matter what race the provider or family is—the connection doesn't happen, trust isn't built, and quality care is far less likely to happen. Cultural communication and understanding are keys to achieving racial equity.
Equity and Inclusion at Children's Minnesota
As Chief Equity and Inclusion Officer at Children's Minnesota, I lead a team whose goal is to identify and dismantle systemic racism and implement cultural change that actively promotes health equity. Those two pieces—dismantling systemic racism and actively promoting equity—are two halves of the whole of
Organizations will have better success with patient satisfaction metrics when there is a team that is formalized, focused, and funded, actively seeking to improve the experience of the entire workforce through equity and inclusion.
In my role, I report daily to the CMO and the Chief Advocacy Officer. I also frequently check in with the Chief Executive Officer. The Equity and Inclusion Department at Children's consists of six people. Besides myself, there are two diversity and inclusion consultants who help the HR Department with recruiting and retention, plan and conduct equity and inclusion trainings, and advise our internal employee resource groups which focus on the specific needs and concerns of LGBTQ+, Muslim, Black, Asian, and Latino employees and nurses of color. We also have two Health Equity Specialists who focus on improving outcomes related to patient health equity. They partner with our Quality Team in disparity analyses and to identify and reduce disparities. They also guide the work of the Health Equity Council, which comprises more than 30 employees from different areas of the system, to focus on how we drive health equity and eliminate health disparities and systemic racism in our work at Children's. There is also an Accountability and Metrics Subcommittee, a Community Subcommittee, a Policy Review Subcommittee, a Training and Awareness Subcommittee, and a Respect and Dignity Subcommittee. The Respect and Dignity Subcommittee acts on reports filed on any instances of emotional harm that occur in the organization. This subcommittee plays a prominent role in changing the culture at Children's. The Equity and Inclusion team also has a Project Coordinator who schedules events in the department and coordinates our work.
Equity and inclusion involve relationship building. To this end, the entire team works with community organizations to promote relationships with employees of Children's. We host “community bridging walks,” in which groups of employees walk through the neighborhoods to build relationships with neighbors, including local merchants. We have a very large physical footprint in the neighborhood, so it's important for us to see ourselves and conduct ourselves as one of the neighbors. We have established and nurtured relationships with the Minnesota Black Chamber of Commerce, the Lake Street Business Council, North Central Minority Supplier Development Council, the Metropolitan Economic Development Association, and other organizations in our community. We recently partnered with the Coalition of Asian American Leaders to bring in an exhibit and community members to speak about the Asian community in the Twin Cities and to talk with employees about what it means to be Asian in Minnesota. We have hosted the Green Card Voices Project at both our Minneapolis and St. Paul hospitals. The project, connecting immigrants and their communities through multimedia storytelling, showcases the amazing accomplishments of immigrant families and community leaders. We sponsor a biweekly video town hall, in partnership with the African American Leadership Forum, about COVID-19 and its impact on the Black community. Two African American women business owners have been contracted to teach healing yoga in our organization to provide an emotional and physical healing space. Another business of color, Common Sense Consulting, is working with our executive leaders to foster understanding of and actions to address racial equity, systemic racism, implicit bias, and inclusion.
To ensure a diverse workforce, my department partners with HR to recruit and retain employees of color in all roles and at all levels of responsibility. Our goals are a 34% rolling 3-year average hiring goal for employees of color, and decreasing attrition of employees of color by 3.4%. Our current attrition rate for employees of color exceeds that for white employees. Preventing unnecessary exits of employees of color from Children's is important for at least two reasons: (a) retaining our employees of color helps with diversity of the workforce and (b) high retention of employees of color is a critical indicator of how equitable and inclusive our culture is overall. It isn't just that we want employees of color to stay; we want to foster the kind of culture in which employees of color feel just as fully a part of creating that culture as everyone else in the workforce.
Our commitment to fostering such a culture also means we've got to hire and promote diverse employees in executive and director-level roles, and provide opportunities for people of color and Native American people in our organizations to seek additional education and training so that when opportunities for promotion occur, the pool of qualified applicants looks like our patient population. This also has implications for where and how we recruit candidates of color and Native American candidates. We recently partnered with the People of Color Career Fair-Minnesota and hired attendees, including some nurses of color. These accomplishments would not happen consistently without a dedicated group of people in our organization working solely on equity and inclusion.
Biggest Successes
I believe our biggest success so far is our equity internship program, which involved hiring young people of color as summer interns. We hired eight interns in partnership with the Dougherty Family College (part of St. Thomas University), which works in the interest of first-generation college students of color, and Achieve Minneapolis, which connects Minneapolis high school students with internships. At the end of their experience, the interns presented to our top 250 leaders their strategies for how to make Children's more inclusive. Some fantastic suggestions came from these young leaders. Our interns identified that the immodesty of our robing and the lack of availability of hijabs showed that we were not valuing the religious traditions of our Muslim patients and families. We are now contracting with a local Somali entrepreneur, Hilal Ibrahim, and her company Henna and Hijabs. The company creates hijabs and robes that serve the needs of both the hospital and our Muslim patients and families.
There is a fair amount of construction on our organization's buildings and grounds. We looked at how many of the subcontractors were minority owned and/or employed workers of color. Since our department began, the percentage of minority subcontractors and workers of color has increased from around 6% to nearly 25% minority subcontractors for many of our construction projects. Our newest policy requires that general contractors who win our bids employ 30% of subcontractors who are women and/or minority-owned businesses. Our intentional focus is on increasing minority-owned business participation. It's worth noting that metrics related to construction were outside the purview of the Equity and Inclusion Department, but when we brought them to the attention of the CEO and COO, action was quickly taken through changing policy and practice.
Fighting Racism at the System Level
When you're dismantling racism at the system level you're looking at policies, practices, and outcomes. You're asking, What kinds of policies have been shown to have a disproportionate or negative impact on patients of color? For example, our organization has a policy of “behavior contracts,” which are assigned to patients and families by our staff. These contracts require patients and families to agree to do certain things and adhere to or refrain from certain behaviors in order to stay in, or visit, our hospital. These behavior contracts originate when someone in our system tags a family as being disruptive or somehow behaviorally inappropriate—maybe they were too loud or cursing. When this policy and its outcomes were examined, we found a disproportionate number of reports and security calls that involved white employees and Black patients and families. We are intentionally reviewing the successes and failures of previous behavioral contracts and examining factors within the system itself that need to be addressed. There are biases and misunderstandings at work in how behavior contracts have been handled—biases and misunderstandings that continue to cause systemic racism and inequitable health outcomes for our Black patients and families.
As each of our organization's policies comes up for review every 3 years (or sooner, if an issue is discovered), the 8–10 members of the Health Equity Council's Policy Review Subcommittee look at each policy through an antiracist/equity lens. The process is a work in progress and is consistently being refined in order to address health equity. We plan to expand this process to be more inclusive of input from patients and families as well.
What Can you Do?
Lobby your organization to establish and fund an Equity and Inclusion Department. There are plenty of models to emulate and plenty of mentors and consultants available to guide you. If your organization is currently unable to invest in a full-scale Equity and Inclusion Department, there are still many things you can do. If there is some funding available, consider the possibility of hiring or promoting someone to a director-level Equity and Inclusion position, complete with a title, paid and/or protected time, an administrative budget, and a clearly articulated level of authority to begin doing some of the things described in this article so far, as well as the actions described in Figure 1, which lists things people can do to help make their organizations more equitable and inclusive.
Equity and inclusion work cannot be accomplished only through implicit bias training and good intentions alone, nor can it be accomplished by addressing one incident of race-based harm at a time. That's why a formalized, focused, funded, executive-level department is essential. Equity, diversity, and inclusion are components of a just and fair society. When done well, equity and inclusion initiatives consistently and systematically enhance community engagement, partnerships, and business.
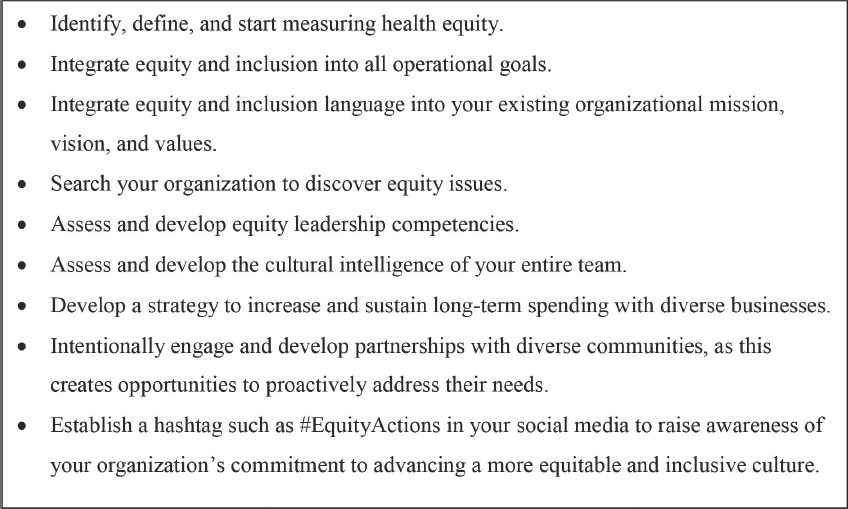
Actions to Make Organizations More Equitable and Inclusive.
There is not one person who will ever enter your organization, either as a patient or family member, as an employee, or as a visitor, who is any less deserving of a loving, compassionate, high-quality experience than anyone else is. If you believe this statement, you'll want to do everything you can as an individual to prove it every day of your professional life. If your organization says it believes that statement, it's time for them to put their money where their mouth is and demonstrate commitment through equity actions and not just words.
Footnotes
James Burroughs II, JD (he/his), is the Chief Equity and Inclusion Officer for Children's Minnesota. His key focus areas include patient quality initiatives, employee recruitment and retention strategies, and organizational culture. James has more than 25 years of experience in nonprofit management, equity, diversity, inclusion, and employment law.
Disclosure. The authors have no relevant financial interest or affiliations with any commercial interests related to the subjects discussed within this article.
Funding. The author(s) received no specific grant or financial support for the research, authorship, and/or publication of this article.