
Abstract
Objective:
Little is known about relations between religious involvement and suicidal behaviors in mainland China. This study aims to examine the association between religious involvement and suicidal ideation, planning, and attempts within a general community population controlling for socio-demographic, physical, and mental health factors.
Method:
Data were examined from a population-based sample of 2,769 community-dwelling adults in the province of Ningxia China, where nearly 40% are Muslim, 11% other religious affiliations, and 49% no religion. Four separate logistic regression models examined correlations between religious involvement and self-reported suicidal thoughts, plans, and attempts. Analyses were also stratified by Muslim affiliation (n = 1103) and no religion (n = 1,366).
Results:
Bivariate analyses in the overall sample demonstrated that higher personal religiosity scores (χ2 = 6.8, p < 0.01) and total religiosity scores (χ2 = 5.1, p < 0.05) were positively correlated with developing a suicidal plan, which disappeared after controlling for demographic characteristics. Otherwise, no significant correlations were found between any religious characteristic and suicidal ideation, plan, or attempt in either Muslims or those with no religion.
Conclusions:
In contrast to most previous studies, religious involvement plays less of a role in suicidal behaviors in at least one province of mainland China.
Introduction
Suicide is a major public health problem worldwide and in China. Between 1995 and 1999, the annual suicide rate in China was estimated to be 23 per 100,000 [1]. For comparison, the suicide rate in the United States during this period (1996-1999) was 10.7-11.6 per 100,000 [2, 3]. Despite the surprising decreased national suicide rate in recent years [4], China still is the largest contributor to the absolute number of annual suicides in the world because of the size of its population [5, 6].
An understanding of suicide risk and protective factors is imperative for effective prevention. Suicidal ideation and suicide planning have been identified as pre-conditions for suicide [7–9]. Suicide attempts in China, even when they do not prove lethal, can result in serious and long lasting physical disability [10].
The relationship between religiosity and mental disorders and suicidal behaviors is now receiving increased attention in the empirical literature [11]. Many gaps in the literature remain. First, most studies have focused almost exclusively on Christian populations, and have typically been conducted in countries that are generally religious and well-developed economically. Little research has been done in non-Christian cultures like the one that exists in China. Second, most studies have found an inverse association between religious involvement and suicidal ideation. Strong arguments exist for the protective effects of religiosity on completed suicide, although the research is less consistent on findings between religious involvement and suicidal ideation and attempts. For example, the Collaborative Psychiatric Epidemiological Survey (CPES) study reported that religious attendance was protective against suicidal ideation, but not for suicide attempts [12]. Similarly, the Canadian Community Health Survey (CCHS) study found that frequent religious attendance reduced the risk of suicide attempts, but not suicidal ideation [13, 14]. Finally, a systematic review found that most studies examining religion and suicidal behavior failed to take into account relevant sociodemographic factors such as age and gender which may help to explain many of the observed relationships [15].
Religiosity and Non-Lethal Suicidal Behaviors in Muslims
Muslims represent the second largest religion in the world. Research on the relationship between religiosity and suicidal ideation and attempts has likewise been neglected in this religious group [16]. Several studies have reported a relationship between religiosity and mental health in Muslim adolescents, including positive correlations with happiness, life satisfaction and overall better mental and physical health [17]. Likewise, negative correlations have been found between religiousness and depression in Saudi college students [18]. Nevertheless, few studies have been conducted on religiosity and suicidal behaviors among Muslims in the general adult community population.
Religion in China
China is known to be less religious than many Western countries, due largely to the political control of and legal restrictions on religious activities [19]. For years, government regulations of religious practice in China prevented the free expression of religion and the willingness to admit to religious involvement [20]. Despite this, China has a diverse religious population that consists of Buddhists, Daoists, and a variety of other Chinese religions, Muslims, Jews, and Christians [21]. As a result of increased desire of the Chinese people for religious freedom, and current social and economic changes that are occurring in China, there is a rapidly increasing percentage of the population who claim some type of religious practice (from 7.0% in 2001 to 23.9% in 2007) [22].
Muslims make up only about 2% of the population of China, and most Chinese Muslims live in western border areas, including Inner Mongolia, Tibet, Gansu, and Ningxia [23]. The largest ethnic group in China is the Han, who make up 91.5% of the population. Because Muslims make up only a small percentage of the population, they exert little if any political influence and control few resources in any of the states and provinces in China [24]. The present study takes place in the Ningxia province of China, where over one-third of the population is Muslim.
To our knowledge, this is the first study to examine the relationships between religious involvement and non-lethal suicidal behaviors in a large, representative sample of community-dwelling adults in China. The objectives of this study are to: (1) examine the association between religious involvement and suicidal ideation, planning, and attempts; (2) examine these relationships within a general community population controlling for sociodemographic, physical, and mental health factors; and (3) explore the connections between religiosity and suicidal behaviors in Chinese Muslims compared to those with no religious affiliation.
Methods
Participants
Participants were from a population-based Epidemiological Study of Mental Disorders in the province of NingXia (ESMD-NX), China. A three-stage sampling method was used to select a representative sample of 6,476 persons aged 18 years or older, who had lived for at least 6 months here. In summary, 62 primary sample units (PSU) were selected from 2,209 villages and 393 neighborhood communities using a probability proportionate to size (PPS) method in the first stage. In the second stage, 60 to 210 households were identified from each PSU using a systematic sampling method resulting in a total of 6,890 households being selected. In the final stage, 85 trained interviewers from Ningxia Medical University visited each household and used a Kish selection table [25] to randomly select one eligible participant from each household. Interviewers were unable to reach the household member selected in 414 cases, resulting in a total sample of 6,476 participants who were approached to conduct a face-to-face interview from July 2011 to January 2013. Of those, 5,810 participants (89.7%) completed the interview. The present study consisted of 2,769 participants who completed the Part II interviews described below. The ESMD-NX study was approved by the institutional review board of the Ningxia Medical University.
Measurement
The computer assisted personal interview (CAPI) [26] version of the WHO composite international diagnostic interview (WHO-CIDI) was used to diagnose mental disorders and to document suicidal thoughts and behaviors. The interview schedule was divided into two parts. Part I, which was administered to all respondents, included the core WHO-CIDI diagnostic interview for mental disorders and questions about suicidal ideation, plans, and attempts. Respondents were asked three “yes” or “no” questions about whether they had ever seriously thought about killing themselves and, if so, whether they had these thoughts in the past 12 months. Respondents who reported suicidal ideation were then asked whether they had ever made a plan to commit suicide and, if so, whether they made such a plan within the past 12 months. Those reporting suicidal ideation were also asked whether they ever attempted suicide in the past.
Part II included assessments of religious involvement and other correlates of the core mental disorders and suicide behaviors [27]. Three groups were selected to complete Part II assessments. First, all the respondents who (1) met lifetime criteria for at least one mental disorder assessed in Part I, (2) met subthreshold lifetime criteria for a mental disorder and sought treatment for it at some time in their life, or (3) either ever made a plan to commit suicide or attempted suicide, were selected to complete Part II of the evaluation. Second, a probability sample was selected of 59% of respondents who did not meet criteria for membership in the first group, but gave responses in Part I indicating that they either (1) ever met subthreshold criteria for Part I disorders, (2) ever sought treatment for any emotional or substance abuse problem, (3) ever had suicidal ideation, or (4) used psychotropic medications in the past 12 months to treat emotional problems. Third, a 25% random sample of respondents without mental disorders or emotional problems was selected to receive the Part II evaluation [28]. Selection of subjects to complete Part II was controlled by the CAPI program.
Religious involvement was assessed based on seven Likert scale type questions: (1) “How closely do you identify with other people who are of the same religious group as yourself—very closely, somewhat, not very, or not at all?”; (2) “If you could choose, how much time would you like to spend with other people who are of your same religious group—a lot of the time, some, a little, or none of the time?”; (3) “How important do you think it is for people who share your religion to marry other people who are also from this group—very important, somewhat, not very, or not at all important?”; (4) “How often do you usually attend religious activities—more than once a week, about once a week, one to three times a month, less than once a month, or never?”; (5) “In general, how important are religious or spiritual beliefs in your daily life—very important, somewhat, not very, or not at all important?”; (6) “When you have problems or difficulties in your family, work, or personal life, how often do you seek comfort through religious or spiritual means, such as praying, meditating, attending a religious or spiritual service, or talking to a religious or spiritual advisor—often, sometimes, rarely, or never?”; and (7) “When you have decisions to make in your daily life, how often do you think about what your religious or spiritual beliefs suggest you should do—often, sometimes, rarely, or never?” [27].
Four variables were created based on responses to the above questions: social religiosity, personal religiosity, overall religiosity, and high (vs. low) religiosity. Social religiosity consisted of questions 1,2,3, and 4, whereas personal religiosity was composed of questions 5, 6, and 7. This division into social and personal religiosity was based on the content of the items; those items where religiosity was expressed in terms of participation with others or related to family matters were categorized as social religiosity, whereas those items that had to do with personal, more private forms of religious expression were categorized as personal religiosity. Overall religiosity was the sum of the personal and social religiosity scales. High religiosity was determined by the combination of responses “very closely” on question 1, “a lot of time” on question 2, “somewhat or very important” on question 3, “at least 2-3 times per month” on question 4, “very important” on question 5, “sometimes or very often” on question 6, and “sometimes or often” on question 7.
Sociodemographic information was collected using the demographic section of the CIDI. Physical health variables included overall self-reported physical health, self-reported chronic body pain, type II diabetes, and hypertension. Mental health variables include overall self-reported mental health, any ICD-10 mental disorders, any affective disorders, and any anxiety disorders.
Statistical Analyses
Statistical analyses were performed using SAS 8.2 software. Bivariate associations between participant characteristics and suicidal ideation, plan, and attempt were examined using one-way-analysis of variance for continuous variables and chi-square statistic for categorical variables. Four separate logistic regression models were constructed to identify the independent effects of religious involvement on suicidal thoughts and behaviors. Analyses were then stratified by religious affiliation (Muslim vs. no affiliation). Unstandardized beta and standard errors were calculated for the models. Given the exploratory nature of these analyses, statistical significance level was set at a p value of 0.05, without corrections for multiple comparisons.
Results
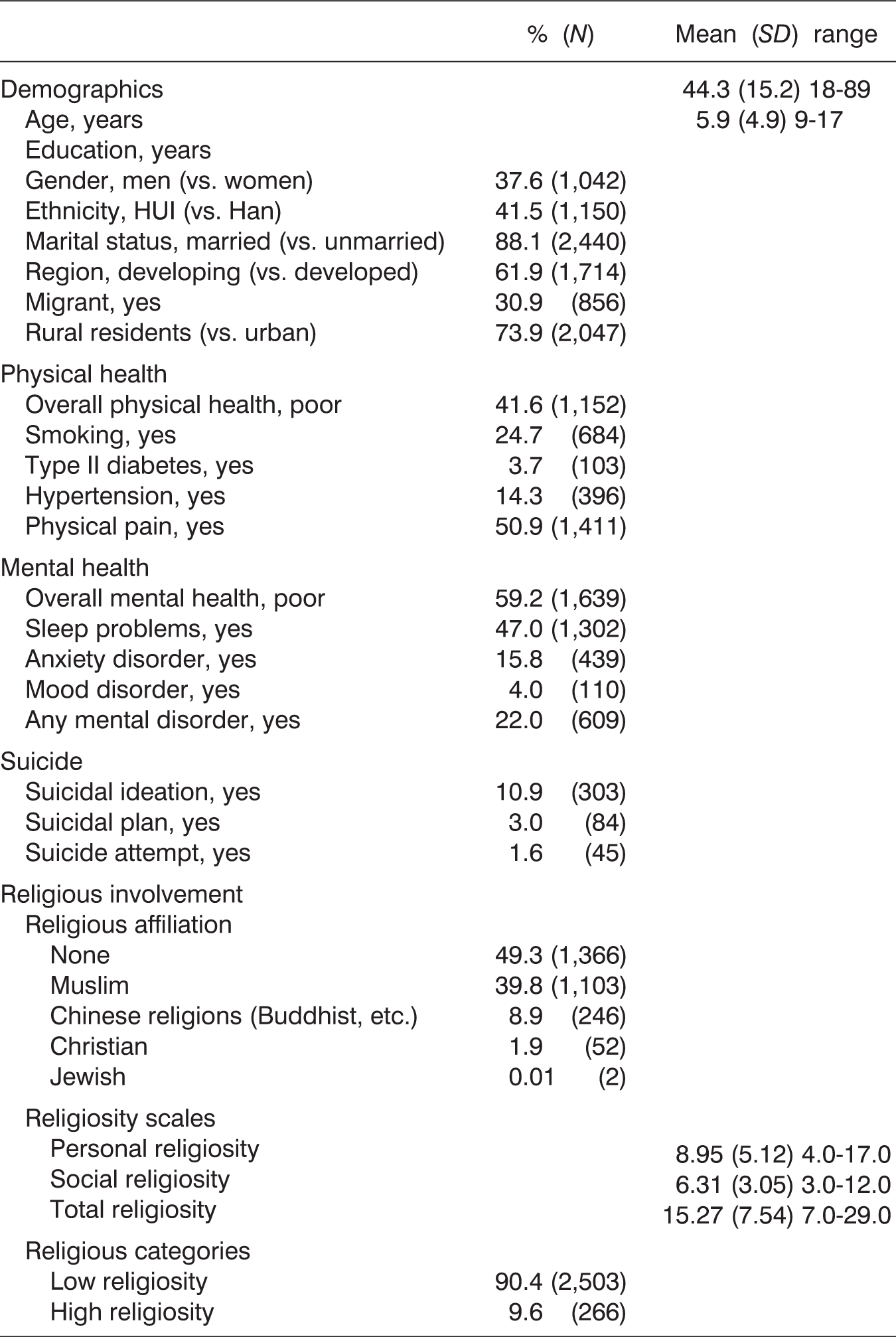
Characteristics of the Sample (n = 2,769)
Bivariate Associations between Participant Characteristics and Suicidal Ideation, Plan, and Attempt (n = 2,769) for All Comparisons)
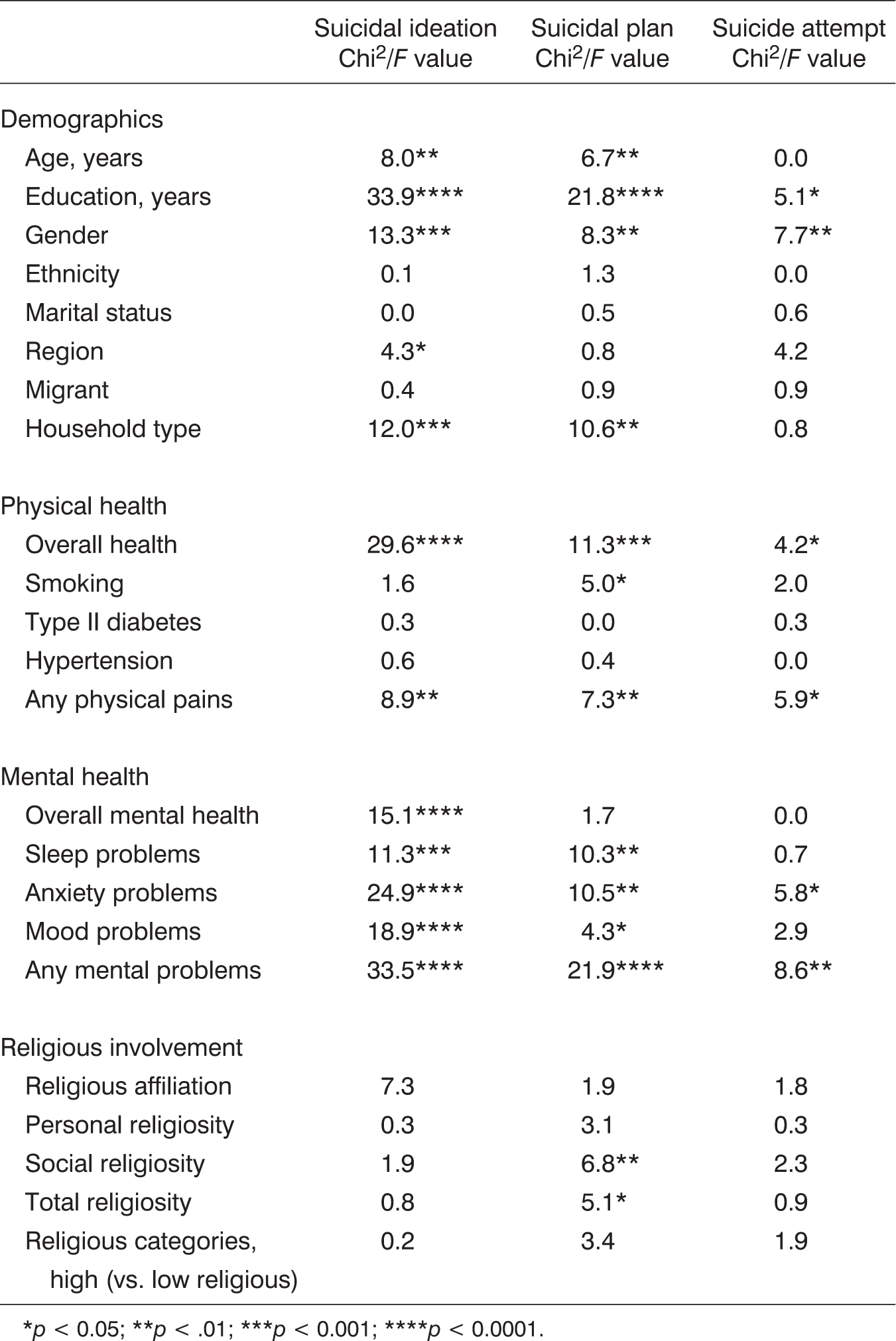
p < 0.05;
p < .01;
p < 0.001;
p < 0.0001.
Logistic Regression Analyses Examining Relationships between Religiosity and Suicide Ideation, Plan, and Attempt (n = 2,769 for All Models)

Model 1 = religious variable; Model 2 = Model 1 + demographics; Model 3 = Model 2 + physical health; Model 4 = Model 3 + mental health.
p < 0.05;
p < 0.01; B = beta, SE = standard error.
Logistic Regression Analyses Examining Relationships between Religiosity and Suicide Ideation, Plan, and Attempt in Muslims vs. No Religious Affiliation (n = 2,769 for All Models)

Model 1 = religious variable + demographics; Model 2 = Model 1 + physical health + mental health.
p < 0.05;
p < 0.01; B = beta, SE = standard error.
Discussion
This is one of the first studies to examine the relationship between religious involvement and suicide in a population-based community-dwelling sample of adults in mainland China, a country with one of the lowest rates of religious involvement and one of the highest suicide rates in the world [6]. We found no correlation between religious involvement and suicidal ideation, planning, or attempt in the residents of Ningxia province, China. Even among Muslims, a religious group known for having some of the lowest suicide rates in the world, religious involvement was unrelated to suicidal ideation, plan, or attempt (and there was no difference between Muslims and those with no religious affiliation on any of these).
Previous research conducted primarily in Western countries has found that degree of religiosity is directly related to suicidality, with greater religiosity predicting fewer suicidal thoughts, attempts, and completed suicide [12, 13, 29]. Several reasons could explain the difference between our findings and the vast majority of other studies in this area.
First, the sample in the present study was drawn from a country that is much less religious than countries in which prior studies have taken place. Religious involvement in mainland China is reported to be anywhere from 8% to 31% [30, 31] and China is the country with the highest percentage of convinced atheists in the world (47%) [32]. Well established is the fact that religion is often turned to for comfort and strength during times of adversity. In countries where religion receives little support from the surrounding culture, people may only turn to religion when all other avenues of help have been exhausted. Those with emotional problems that are resistant to treatment may turn to religion for comfort, and while religious belief and practice may help them to some degree, they are unlikely to reduce negative emotional symptoms to the level of well-adjusted or otherwise situationally fortunate individuals who have no need for religion because they are experiencing little distress. Thus, religious involvement may serve as an indicator or marker of distress in such populations, and in cross-sectional studies like the present one, any benefit in relieving distress (or suicidal tendencies) may be concealed by the dynamic of persons turning to religion for comfort in response to that distress.
The second possibility is that there simply is no relationship between religious involvement and suicidal ideas or behaviors among those adults living in the Ningxia province of China. Because this is among the first studies of religiosity and suicidal behavior in a general adult population living in mainland China, there are no other studies that we are aware of to compare with. Although Liu and Koenig reported a significant inverse correlation between suicidal ideation and intrinsic religiosity (IR) in women aged 18 to 34 years old in the rural Hebei province in northeast China [33], no previous research has examined other indicators of religious involvement and suicidal behavior (such as plans or attempts) among adults of all ages and genders in the population. Another study conducted in a South Korean population (with a similar religious culture as mainland China) also found no relationship between religiosity and depression (a key risk factor for suicide) or quality of life among Buddhists (the main religion in most provinces of China) [34].
Phillips et al. [35] have suggested that beliefs about reincarnation might make suicide an attractive option in China and cite evidence that suicide was historically a culturally and morally approved response to certain circumstances. With rapid development and the “Opening Policy” in modern China, the motivation toward religious faith has become more rational than the situation in the 1980s [36]. The sharp decline in national suicide rates in recent years does not support the notion that suicide is culturally or morally encouraged in modern Chinese society.
Finally, the present study is unique in that the sample consisted of almost 40% Muslims. Muslims, who are mostly of Hui Min ethnicity (vs. Han, which is the primary ethnicity of China), are considered a minority (similar to African-Americans in the United States) and are under considerable economic and social pressures. There has never been a study on suicidal behavior and religiosity in this ethnic group in China (or in Chinese Muslims) until the present one. A previous report from the ESMD-NX study found that the prevalence of suicidal ideation was somewhat higher in Hui (5.9%, 95% CI = 4.9-6.9%) than in the largely secular Han (4.5%, 95% CI = 3.8-5.3%). However, after controlling for demographic variables, no statistically significant difference persisted between the two ethnic groups [37].
The impact and influence of the Islamic faith on suicidality in non-Muslim countries like China has received little attention from researchers. Although suicide rates tend to be lowest in Muslim countries, particularly those in the Middle East and South Asia, studies have found that Muslims in some non-Muslim countries and in European Muslim countries have much higher suicide behaviors [38]. For example, a study in Israel that compared 5-year suicide registry data with findings from other national community surveys found that, while completed suicides were lower in Muslims than in Jews (3.0 vs. 8.2 per 100,000, respectively), lifetime suicide attempts were significantly higher in Muslims (2.8%) compared to Jews (1.2%), and no difference was found in lifetime suicide ideation or planning between Muslims (6.6% and 2.1%) and Jews (5.2% and 1.9%) [39].
Likewise, in a study from Turkey (considered to be a modern and more liberal Muslim country), Eskin and colleagues found no relationships between religious belief and suicidal ideation or suicide attempt in a sample of high school students [40]. Even in a conservative Muslim country like Pakistan, a survey of college students found that suicide ideation was relatively high and equal in both men and women [41],
The present study has several limitations. First, since both religiosity and suicidal ideation/behavior were measured by self-report, recall bias may have influenced the accuracy of the data reported. Second, the questionnaire used to assess religiosity was not a standard one whose psychometric properties were established, although the face validity of the items should be apparent. Third, given the relatively low rates of suicide attempt and planning, this study had relatively low power to detect differences in suicidal behaviors based on religious involvement. Only 45 participants (1.6%) reported a suicide attempt and 84 (3.0%) indicated a suicidal plan in the total sample, and among those with no religious affiliation, only four subjects scored high on religiosity and none of these attempted suicide (affecting betas and standard errors in the logistic regression models). Finally, the sample selected for this study was from only one province in China, and generalizing results to the entire country must be done with caution.
In summary, this study found no association in either bivariate or multivariate analyses between religiosity and suicidal ideation or suicide attempts. When stratifying analyses by Muslim vs. no religious affiliation, no association was found between religiosity and suicidal behaviors in either group. These findings are different from those reported by more than three-quarters of over 140 studies conducted largely in Western or Middle Eastern countries that have reported inverse relationships between religiosity and suicidal ideation or behaviors [42], As a result, the present results provide important cross-cultural information that advances our understanding of (1) the relationship between religious involvement and suicide more generally, (2) the relationship between religious involvement and suicide in mainland China, and in particular, (3) the relationship between religiosity and suicide in Muslims compared to non-religious persons in China.