
Abstract
Background
Nitric oxide synthase (NOS) inhibition has been demonstrated to correct systemic vasodilation and renal hypoperfusion in studies of patients with cirrhosis. In patients with decompensated cirrhosis, NOS blockade increases arterial pressure, but the acute effects on hepatic and renal hemodynamics are not known.
Methods
We examined the acute systemic, hepatic, and renal hemodynamic effects of NG-monomethyl-l-arginine (l-NMMA) in 10 patients with decompensated cirrhosis. After baseline measurements, 3 mg/kg l-NMMA was administered as an IV bolus. At 20 minutes, if mean arterial pressure did not increase by at least 10 mm Hg above the baseline value, a second injection of 6 mg/kg was administered.
Results
In 5 of 10 patients, the second injection of l-NMMA 6mg/kg was necessary to achieve at least a 10 mm Hg increase in mean arterial pressure. Acute NOS inhibition increased systemic vascular resistance and decreased cardiac output, without causing changes in the hepatic venous pressure gradient. Hepatic blood flow decreased, but the indocyanine green intrinsic clearance and extraction remained unchanged. Plasma renin activity (from 9.5±2.9 to 6.7±1.6 ng/ml/h) and urinary prostaglandin E2 (from 299±40 to 112±36 pg/ml) significantly decreased. No significant changes in glomerular filtration rate, renal plasma flow, and natriuresis occurred, however.
Conclusions
Acute l-NMMA infusion in patients with decompensated cirrhosis reduced hepatic blood flow and decreased plasma renin activity and urinary prostaglandin E2, without causing significant changes in renal hemodynamics.
Keywords
Introduction
Portal hypertension is associated with a hyperdynamic circulation. Arterial (mainly splanchnic) vasodilation participates in this hyperdynamic circulation 1 and activates potent vasoconstrictor and antinatriuretic mechanisms, thereby contributing to reduced renal perfusion. 2 A strong body of experimental evidence suggests that nitric oxide (NO), a potent vasodilator, plays a pivotal role in this condition.3–6 Accordingly, increased production of NO has been reported in patients with cirrhosis.7–9
In patients with cirrhosis with portal hypertension, the role of NO is complex and not entirely understood. In the liver, NO may play a role in the dynamic regulation of intrahepatic vascular resistance. 10 Decreased sinusoidal NO release in the cirrhotic liver may participate in increased sinusoidal pressure. 11 In the kidney, cortical vasoconstriction in conjunction with the increased production of vasoconstrictors is balanced by increased intrarenal production of vasodilator substances such as NO 12 or prostaglandins. However, the contribution of intrarenal NO in this delicate equilibrium between vasoconstrictors and vasodilators is not known. Therefore, it is difficult to predict the effects of nitric oxide synthase (NOS) inhibitors on hepatic blood flow (HBF) and renal function in patients with cirrhosis and impaired renal perfusion. On the one hand, the systemic and splanchnic effects of NOS inhibition may increase mean arterial pressure (MAP) and deactivate vasoconstrictor systems; on the other hand, inhibiting NOS in the liver and the kidney may have deleterious effects.
Two studies of patients with cirrhosis examined the hemodynamic effects of NG-monomethyl-l-arginine (l-NMMA) administration.13,14 Forrest et al., 13 using a 30-minute infusion of 3 mg/kg l-NMMA, observed a significant increase in MAP in Child A and Child B but not in Child C patients. No effect on hepatic venous pressure gradient (HVPG) or azygous blood flow was observed. Renal hemodynamics and HBF were not investigated. In the La Villa et al. study, 14 a 3-mg/kg bolus followed by a 120-minute infusion of l-NMMA corrected the altered hemodynamics and improved renal function in patients with Child A cirrhosis. The aims of this study were to determine the dose of l-NMMA that may increase MAP by at least 10 mm Hg above baseline values (i.e., dose-finding phase) and to study the invasive effects of acute NOS inhibition on systemic, hepatic, and renal hemodynamic changes in 10 patients with cirrhosis, ascites, and moderate to severe liver failure.
Patients and Methods
Patients
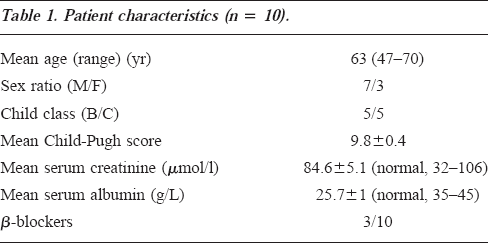
The characteristics of the 10 patients with biopsy-proved alcoholic cirrhosis with ascites are shown in Table 1. All of the patients had stopped drinking at least 6 weeks before the study. All patients had baseline MAP up to and including 90 mm Hg and presented with clinical indications for transjugular liver biopsy. The presence of hepatic encephalopathy, documented hepatocellular carcinoma, recent (<2 wk) gastrointestinal bleeding, nephrotoxic drug administration, cardiac failure, known pulmonary arterial hypertension, severe renal failure (serum creatinine >120 μM, proteinuria >0.5 g/24 h), organic kidney disease (defined as the presence of casts and red blood cells in the urinary sediment), or abnormal kidney as determined by ultrasonography were considered exclusion criteria. All patients were on a salt-restricted diet (88 mM/d Na), and diuretics (spironolactone and/or furosemide) were stopped at least 3 days before the study began. Three patients were being treated with β-blockers. Paracentesis was not performed within 3 days of the start of the study.
Patient characteristics (n = 10).
Study protocol
After completion of the liver biopsy, baseline measurements, including sinistrin (an analogue of inulin) and p-aminohippurate (PAH) clearances, were performed. The primary endpoint was an increase in MAP at least 10 mm Hg above the baseline value. We chose the primary endpoint of 10 mm Hg because this threshold value approximated the 12 mm Hg increase in MAP in the study by Forrest et al. 13 MAP was measured using a semiautomatic sphygmomanometer, whereas heart rate (HR) and electrocardiographic data were monitored continuously.
Dose-finding phase
A 3 mg/kg l-NMMA dose diluted in 10 ml 0.9% saline (Clinalfa AG, Läufelfingen, Switzerland) was administered as a slow bolus injection for 5 minutes. If MAP did not increase by at least 10 mm Hg above baseline values 20 minutes after the end of the first 3 mg/kg l-NMMA injection, a second dose of 6 mg/kg was administered, followed by the same MAP measurements. The decision to administer a double-dose of l-NMMA was made on the basis of the observation that five of seven patients did not increase their MAP in the study by Forrest et al. 13 This observation period was chosen because peak hemodynamic changes occur 20 minutes after l-NMMA infusion. 13 In addition, hemodynamic changes after l-NMMA administered as a single bolus have been shown to last longer than 1 hour. 15 The systemic, hepatic, and renal function parameters were repeated at the end of the study period.
Hemodynamic measurements
With the patients under light sedation with meperidine (25–50 mg IV), a 9-French central vein introducer (Maxxim Medical Europe, CITY, The Netherlands) was placed in the right internal jugular vein. Then, using fluoroscopic control to record free and wedged hepatic venous pressures, an 8-French catheter (Cordis Europa, Amsterdam, The Netherlands) was inserted in the right hepatic vein. HVPG was calculated as wedged minus free hepatic venous pressure. A Swan Ganz thermodilution catheter was used to measure cardiac output and mean pulmonary arterial pressure (MPAP), with the midchest being used as the external zero reference. Cardiac output was averaged on the basis of three consecutive measures. The systemic vascular resistance (SVR) was calculated using the standard formula. Hepatic blood flow was measured using the standard indocyanine green (ICG) clearance and extraction method. 16 Briefly, after a bolus infusion of 0.5 mg/kg ICG in a peripheral vein, a continuous infusion was started at a rate of 0.3 to 0.5 mg/min. After allowing 25 minutes for equilibrium, serial blood samples were collected every 2 minutes from a central vein and the hepatic vein simultaneously. After centrifugation, the samples were analyzed by spectrophotometry. The hepatic extraction ratio (ICGExt) was then calculated. Hepatic blood flow was calculated only in patients with ICGExt greater than 10%. Indocyanine green intrinsic clearance (ICGCli) was also calculated according to the standard formula ICGCli = HBF x ICGExt÷(1-ICGExt). 16
Renal hemodynamics
Under sterile conditions, an indwelling bladder catheter was placed in all patients to measure constant urine output. Effective renal plasma flow (RPF) and glomerular filtration rate (GFR) were assessed by clearances of p-amino-hippurate and sinistrin, respectively, as described by Buclin et al. 17 An intravenous loading dose of PAH and sinistrin was followed by a continuous infusion throughout the study period. After a 75-minute equilibration period, baseline urine and plasma levels were obtained from a central vein. Thirty-minute urinary collection was then performed, and serial plasma levels of sinistrin and PAH were measured. Plasma and urine levels of sinistrin and PAH were determined by a photocolorimetric method (Kontron Uvicon 80; Kontron, Munich, Germany). Clearances (ml/min) were calculated using the formula Cx=UxV÷Px, where Ux and Px represent urine and plasma concentrations of x, and V is the urine flow rate in ml/min. Renal vascular resistance was calculated using the following formula: (MAP-inferior vena cava pressure) x (80÷RPF)÷(1-hematocrit). 18 The filtration fraction (FF) was calculated as the ratio of sinistrin and PAH clearances.
Blood sampling
Blood sampling for the assessment of plasma renin activity (PRA) was drawn with the patient supine, collected under ice in potassium ethylenediamine tetra-acetic acid tubes, centrifugated at 4°C, and frozen at -70°C until assayed. We used a specific, sensitive radioimmunoassay of the generated angiotensin-1 after an incubation period of 1 hour.19,20 The normal values are 0.23 to 1.55 ng/ml/h with a salt-restricted diet.
Atrial natriuretic peptide
Plasma samples were purified by the solid phase extraction procedure using Sep-Pak minicolumns as described by the manufacturer (Sep-Pak Classic C18; Waters AG, Rupperswil, Switzerland). Thereafter, atrial natriuretic peptide (ANP) was determined by radioimmunoassay 20 using 125I-ANP (Sodiag, Losone, Switzerland), rabbit anti-αANP antiserum (Phoenix Pharmaceuticals, Mountain View, CA), and αANP (Peninsula Laboratories, Belmont, CA). The detection limit for ANP determination was 5 pg/ml plasma. The mean value in healthy humans is 13.2±1.8 pM. The intra- and interassay coefficients of variation were estimated to be 5 and 7%, respectively. The ANP recovery rate was estimated by extracting two additional samples of 125I-ANP (approximately 3000 cpm) with each series of ANP extractions. Using this method, we found a mean recovery rate of 69±2%.
Endothelin-1
Plasma endothelin-1 (ET-1) concentration was measured by a solid phase enzyme-linked immunosorbent assay after a 90-minute incubation time, using the quantitative enzyme immunoassay technique (R & D Systems, Abingdon, UK). The mean value in healthy humans is 0.6 pg/ml (0.3–0.9 pg/ml). The intra- and interassay coefficients of variation were 4.5 and 5.1, respectively. Cross-reactivity with Big Endothelin, ET-2, and ET-3 were <1, 45, and 14%, respectively.
Aspartate aminotransferase
Aspartate aminotransferase (AST) concentration was measured using a standard enzymatic colorimetric method performed with an autoanalyzer (Beckman Coulter, Gagny, France). The normal value is 12 to 50 IU/L. The intra- and interassay variations are 5.3 and 3.5%, respectively.
Urine sampling
Prostaglandin E2.
Urinary excretion of prostaglandin E2 (PGE2) was measured by a 125I-PGE2 radioimmunoassay system (Amersham International, Buckinghamshire, UK). Urine was centrifugated to exclude sediments and was kept frozen until analysis. Nonesterified fatty acids, which can interfere with the PGE2 assay, were removed by the solid phase extraction procedure using Amprep minicolumns as described by the manufacturer. To evaluate extraction efficiency, 3H-PGE2 was used as an internal standard. The relative affinities of the anti-PGE2 for eicosanoids were found to be as follows: 100% for PGE2; 5% for PGE1; and <0.01% for 6-keto-PGF1α PGD2, 6-keto-PGE1, and arachidonic acid. The detection limit for PGE2 determinations was 1 pg/tube, whereas the intra- and interassay coefficients of variation were estimated to be 7 and 9%, respectively.
Drugs and chemicals
The study drug was purchased from Clinalfa, Läufelfingen, Switzerland. Sinistrin (Inutest) was purchased from Laevosan Gesellschaft (Zürich, Switzerland), and PAH was obtained from SERB Laboratoires Pharmaceutiques (Paris, France). The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the University Hospital of Geneva in 1998. Written informed consent was obtained from each patient studied.
Statistics
All clearance calculations were performed on the basis of standard formulae using the value of the plasma levels before and after each clearance period. The results are expressed as mean±standard error of the mean (mean±SEM). The differences measured before and after l-NMMA administration were analyzed using a two-tailed, paired Student's t test and the Wilcoxon signed-rank test for nonparametric data. The Bonferroni correction for multiple comparisons was used in the evolution of HR after l-NMMA administration. P<0.05 was considered significant.
Results
Systemic hemodynamics
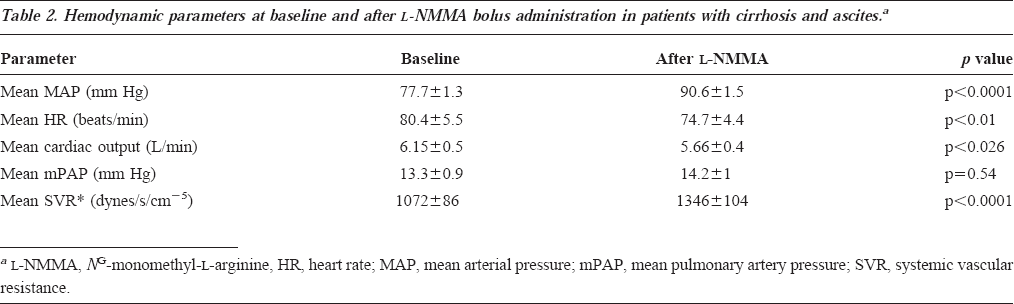
One patient presented with transient nausea during the injection. Hemodynamic parameters at baseline and after l-NMMA injection are shown in Table 2. We observed a significant reduction (p<0.01) in HR 10 and 20 minutes after the end of the bolus injection. MAP increased from 77.7 to 90.6 mm Hg (mean±16.6%, p<0.01). In five patients (Child B/C, 3/2; with β-blockade, 1 of 5), MAP did not increase by at least 10 mm Hg above the baseline value 20 minutes after l-NMMA, and a second injection of 6 mg/kg was administered. There was a significant reduction in cardiac output (mean, -8%; p<0.05) and an increase in SVR (mean, 26%; p<0.01) without significant changes in MPAP.
Hemodynamic parameters at baseline and after l-NMMA bolus administration in patients with cirrhosis and ascites.a
Hepatic hemodynamics
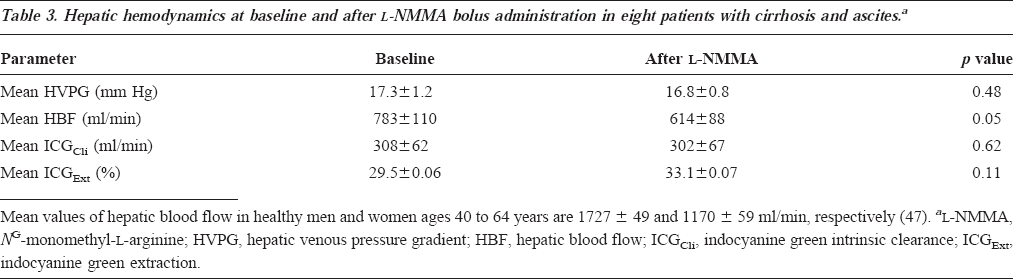
l-NMMA as assessed by HVPG did not affect portal pressure. The criterion of ICGExt greater than 10% was met in eight patients. The results are presented in Table 3. The l-NMMA injection induced a 22% reduction in HBF (p=0.05), which resulted from a stable ICGCli and a nonsignificant increase in ICGExt value. The effects of NOS inhibition on HBF and ICGCli are depicted in Figure 1.
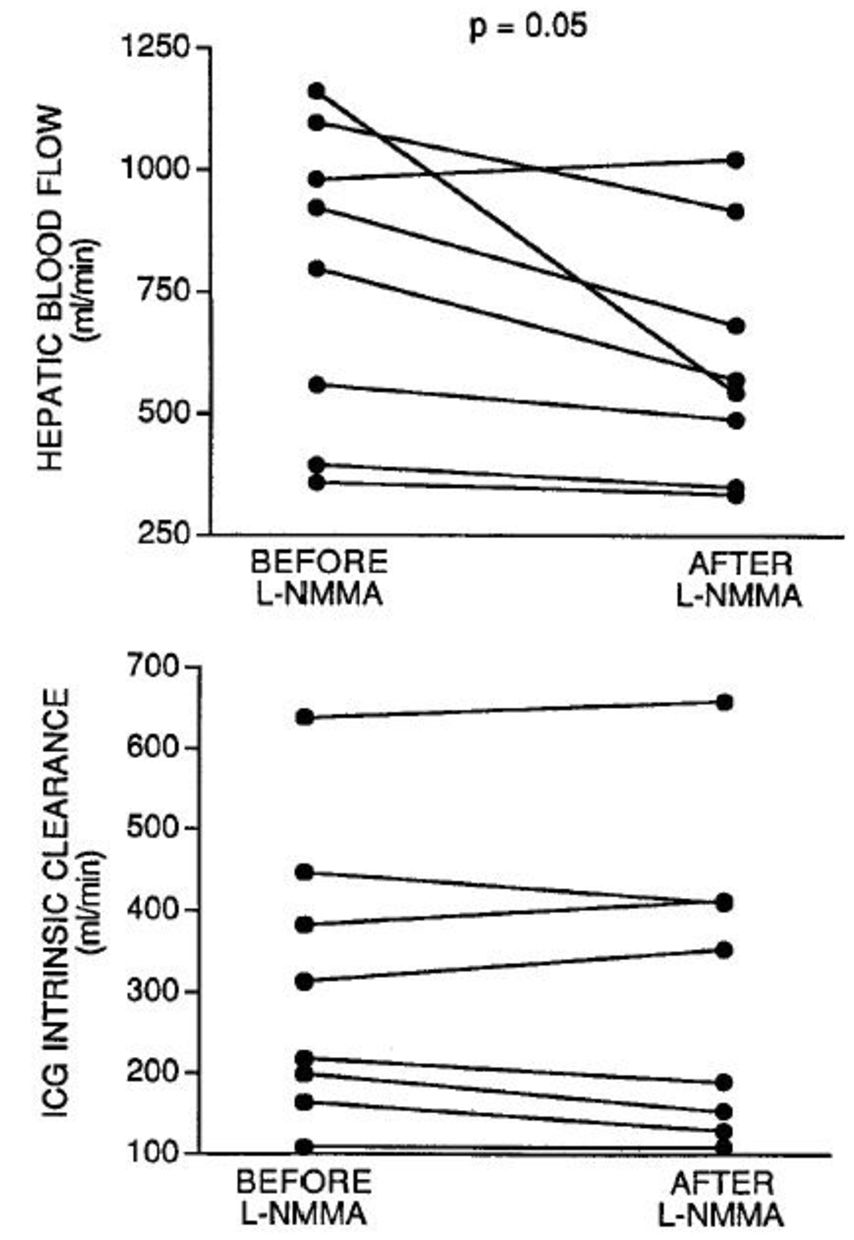
Evolution of HBF and ICG hepatic intrinsic clearance before and after intravenous l-NMMA bolus administration in patients with decompensated cirrhosis (n=8).
Hepatic hemodynamics at baseline and after l-NMMA bolus administration in eight patients with cirrhosis and ascites.a
Renal hemodynamics
For technical reasons, renal hemodynamic measurements could not be performed in three patients. The results obtained in seven patients are shown in Table 4. The evolution of individual values is illustrated in Figure 2. There were tendencies toward an increase in GFR and a decrease in RPF during the study, but urinary sodium remained unchanged. Thus, a statistically significant increase in FF was observed (+21%, p<0.05). Renal vascular resistance increased as compared with the baseline value (+32%; p<0.05; see Table 4).
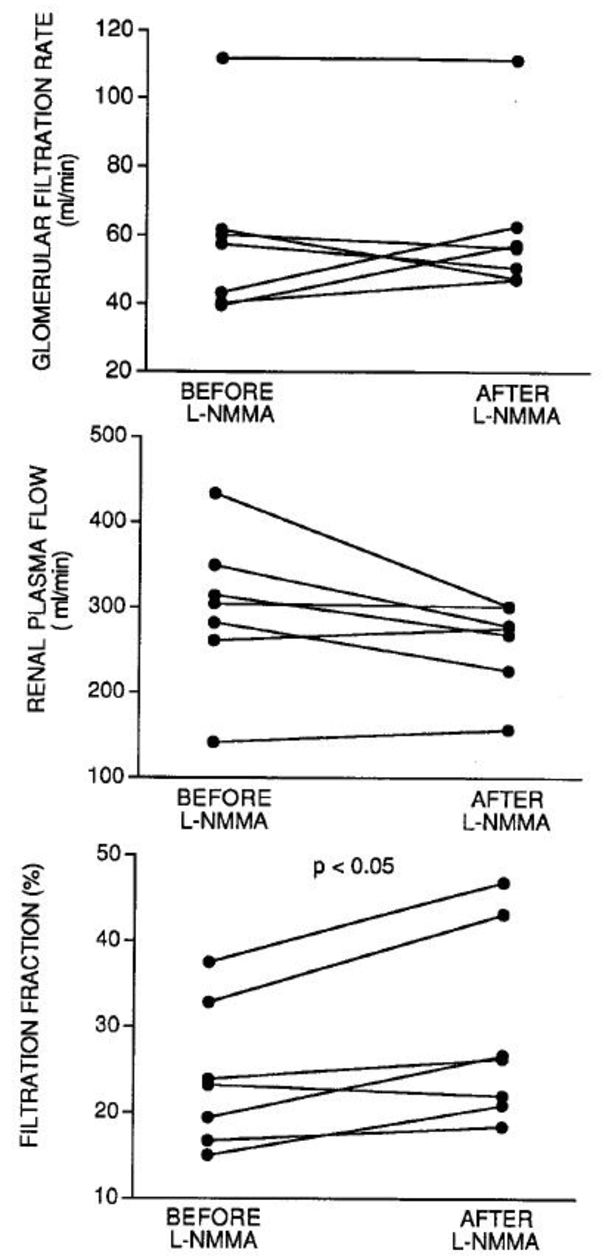
Evolution of GFR, RPF, and FF before and after intravenous l-NMMA bolus administration in patients with decompensated cirrhosis (n=7).
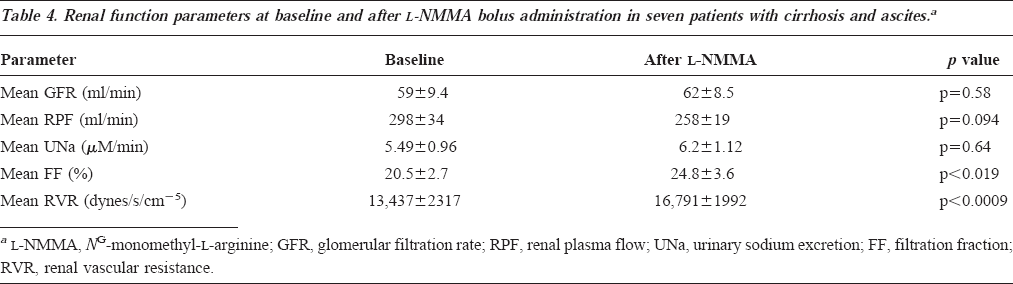
Renal function parameters at baseline and after l-NMMA bolus administration in seven patients with cirrhosis and ascites.a
Biological parameters
Pra.
Mean baseline and post-l-NMMA values are presented in Table 5. Individual values are depicted in Figure 3. PRA was significantly decreased after l-NMMA administration (p<0.05).
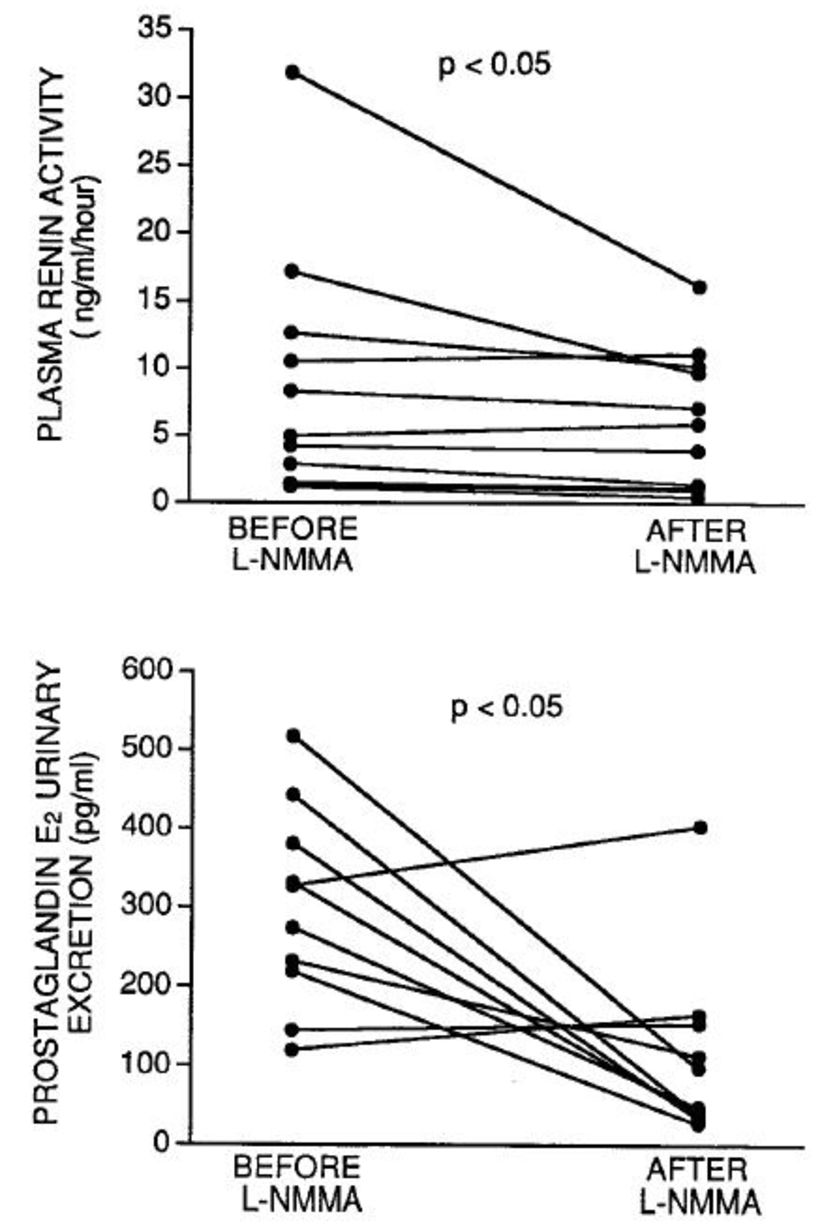
Evolution of PRA and urinary excretion of PGE2 before and after intravenous l-NMMA bolus administration in patients with decompensated cirrhosis (n=10).
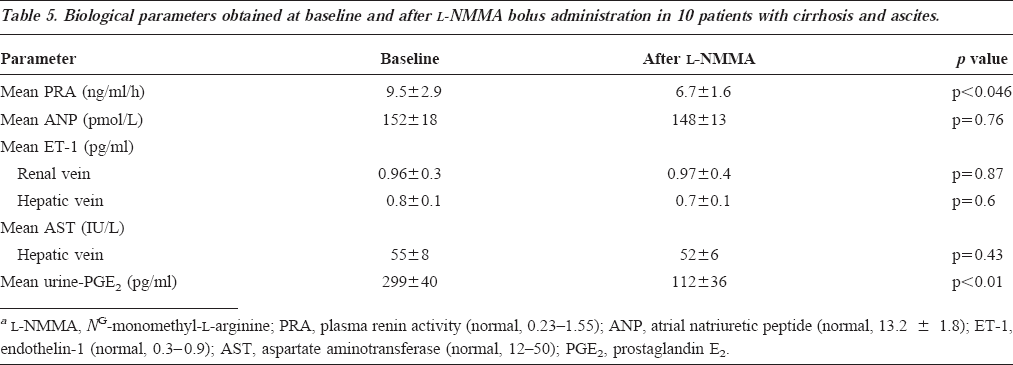
Biological parameters obtained at baseline and after l-NMMA bolus administration in 10 patients with cirrhosis and ascites.
PGE2.
Urinary excretion of PGE2 significantly decreased after NOS inhibition (p<0.05), as depicted in Figure 3. No significant changes were observed after l-NMMA regarding ANP, ET-1, and AST plasma levels.
Discussion
In this article, we report the results of our study of hepatic and renal hemodynamics after acute systemic NOS inhibition in patients with decompensated cirrhosis. In the first invasive hemodynamic study examining the effects of l-NMMA in these patients, Forrest et al. 13 observed an increase in MAP that was limited to Child A and B patients. In a more recent study, l-NMMA administration was followed by a 9% increase in MAP in patients with compensated cirrhosis. 14 The primary endpoint of our study was an increase in MAP of at least 10 mm Hg above basal value. Thus, we performed a dose-finding study to obtain a MAP response, whereas hepatic and renal hemodynamic changes were monitored together with vasoactive mediators. We showed that l-NMMA infusion was associated with an increase in MAP and SVR and a decrease in HR and cardiac output, but no change in MPAP. HVPG remained stable. A significant reduction in HBF was related to a nonsignificant decrease in ICGCli and a nonsignificant increase in ICGExt. The effects of l-NMMA on the kidney showed an increase in renal vascular resistance and FF, without significant changes being observed with regard to GFR, RPF, and urinary sodium. Because l-NMMA is a well-described competitive inhibitor of all isoforms of NOS, we think that the effects measured in this study were related to NOS blockade.
Our findings regarding MAP and HR are consistent with previous results in patients with cirrhosis.13,14 Similar effects were observed in studies of patients with portal hypertension21–23 and might be consistent with excessive production of NO in patients with cirrhosis. 2 NOS inhibition in healthy adults provides similar effects, however, demonstrating that vascular NO production plays a physiological role in the control of blood pressure. 24 Dose-ranging studies demonstrated that cirrhotic rats are more sensitive to the effects of NOS inhibition than are normal rats, but such studies have not been done in humans.3,5 In this study, we show that a double-dose (6 mg/kg) was necessary to achieve a 10-mm Hg or greater increase in MAP in 5 of 10 patients (1 of whom was being treated with β-blockade). Those patients who required a double-dose did not differ from the rest of the group in terms of baseline MAP, Pugh score, and HVPG. We hypothesize that these patients might have greater endogenous production of NO or other vasodilating substances as compared with the others. We chose not to measure systemic NO metabolite production, which is known to be elevated in individuals with cirrhosis 7 and is a poor indicator of regional NO production.
The absence of effects on HVPG after l-NMMA is in line with the findings of other experimental studies. 25 It may be speculated that the vasoconstriction of the splanchnic vascular bed may have been balanced by an increase in portocollateral resistance. 26 However, a new concept has emerged from the demonstration of the dynamic nature of intrahepatic blood flow modulation. According to this concept, the altered sinusoidal perfusion in cirrhosis results from dysequilibrium between sinusoidal overexpression of ET-1, a powerful vasoconstrictor,27,28 and from reduced expression of NOS.10,29 We hypothesize that in our patients, NOS inhibition was not associated with further vasoconstriction of functional sinusoids as reflected by maintained ICGExt and ICGCli after l-NMMA administration. Consistent with this hypothesis, total HBF did not seem to be the limiting factor for metabolic capacity, as already demonstrated in patients with cirrhosis.30–33 In addition, stable AST levels in the hepatic vein were inconsistent with significant liver ischemia.
In contrast to healthy individuals,34,35 GFR and natriuresis were not altered after acute NOS inhibition in our patients. This difference provides evidence that the physiological role of NO in the control of renal circulation is altered in patients with cirrhosis. To interpret these results, it must be remembered that there is an important variation in the degree of renal hypoperfusion in patients with cirrhosis, without clear correlation with liver function or portal pressure. 36 Indeed, baseline GFR was normal in one of our patients, despite the presence of portal hypertension and ascites. Because cardiac output, SVR, and MAP are not the sole determinants of renal blood flow in patients with cirrhosis, 37 no clear association between systemic and renal hemodynamics can be postulated. In the setting of decompensated cirrhosis, decreased renal perfusion pressure, activated renal vasoconstrictors, and prostaglandins seem to have a predominant role. 38 By increasing MAP, we improved renal perfusion pressure and deactivated a major vasonstrictor (PRA). Subsequently, GFR and RPF became less prostaglandin-dependent, as documented by the associated decrease in PGE2 urinary excretion, an estimate of its renal synthesis. 39 Thus, the decrease in both PRA and urinary PGE2 suggests improved intrarenal hemodynamics. Similar findings in urinary prostaglandins were reported in chronic bile duct ligation rats that were administered an NOS antagonist. 40
Why did NOS inhibition not induce the beneficial effects on renal function in our patients with cirrhosis and ascites, which was demonstrated previously in experimental cirrhosis5,12,41 and in patients with compensated cirrhosis 14 ? Indeed, in experimental cirrhosis, acute NOS inhibition did not promote renal vasoconstriction while it increased GFR and natriuresis. These results were interpreted as a lower renal sensitivity of cirrhotic animals to NOS inhibition. The renal response to l-NMMA may differ in animals and humans because of variations among species regarding the role of NO in the control of renal circulation. In healthy humans, renal vasculature seems to be particularly sensitive to NOS blockade, because renal vasoconstriction occurs independently of NOS inhibition-induced MAP changes.34,42
The absence of increased GFR and natriuresis in the present study of patients with cirrhosis, ascites, and liver failure suggests three hypotheses. First, NOS inhibition might have been incomplete because of an insufficient l-NMMA dosage. This hypothesis seems unlikely, given the lack of improved renal response in the five patients who received double-doses of l-NMMA. Second, the administration of l-NMMA might not have been prolonged enough to elicit renal function changes. Indeed, chronic NOS blockade (7 d) in cirrhotic animals was associated with increased natriuresis, 43 and the beneficial effects of l-NMMA on renal function and natriuresis were evident after 1 hour in patients with cirrhosis. 14 Third, the presence of NO in cirrhosis might be beneficial for the maintenance of renal perfusion. Accordingly, Tajiri et al. 44 observed marked natriuresis, together with systemic hypotension after administration of l-arginine, a substrate of NO synthesis, in patients with cirrhosis and ascites. In this study, NO urinary metabolites were increased, suggesting that the natriuretic effects of l-arginine were at least partially induced by the intrarenal action of NO. Therefore, in patients with cirrhosis, altered intrarenal hemodynamics might counteract pressure-induced natriuresis related to the increase in MAP.
As previously reported, 45 circulating levels of ANP are elevated in patients with cirrhosis and ascites. These concentrations were not altered after l-NMMA, however, which was in accordance with constant right atrial pressure. Similarly, elevated plasma concentrations of ET-128,46 remained unchanged. It may be that any functional changes in sinusoidal or glomerular concentrations of a peptide that principally acts in a paracrine fashion are not accessible to hepatic or renal venous sampling.
Conclusions
Acute NOS inhibition in patients with decompensated cirrhosis resulted in the deactivation of the renin-angiotensin system and increased urinary PGE2 excretion. Although this presentation partially reflected improved intrarenal hemodynamics, there were no overall effects on RBF and GFR. Further studies with NOS inhibitors, either chronically or at different dosing regimens, are warranted in such patients.
Footnotes
Acknowledgments
The authors thank the endoscopy staff, and in particular Amparo Jacot and Jacques Lyvet, for excellent technical assistance. They also thank Jacqueline Bornand for expert laboratory work in measuring sinistrin and PAH clearance.