
Abstract

Cocaine abuse can cause a variety of cardiovascular emergencies, especially myocardial ischemia and infarction and is one of the leading causes of emergency room visits for chest pain evaluation in the young population. 1 In 1998, 1.7 million Americans were using cocaine at least once per month, with the highest rates of use among Americans age 18 to 25 years. 2 We present a unique case of cocaine abuse with multiple life-threatening cardiovascular effects.
A 43-year-old African American man presented to emergency room with shortness of breath of 4 hours’ duration. He had chest pain earlier in the day, described as a mild pressure-like sensation localized in the substernal area, which gradually got better. Past medical history was significant for untreated hypertension. Family history was noncontributory. The patient admitted to tobacco, ethanol, and cocaine abuse for years, including cocaine within the last 12 hours.
On examination he was alert, oriented, and in minimal distress because of dyspnea. Vital signs were pulse, 130 beats/min; blood pressure, 120/70 mm Hg and equal in both arms and legs; afebrile; and respiratory rate, 20/min. No jugular venous distension noticed. Carotid upstroke was normal without audible bruits. Chest examination revealed basal crackles bilaterally. Examination of the heart revealed a nondisplaced point of maximal impulse. First and second heart sounds were normal; a third heart sound was heard at the apex with a grade 2/6 holosystolic murmur of mitral regurgitation. No aortic regurgitation murmur was audible. Abdominal, rectal, and neurological examination was unremarkable.
Initial laboratory data revealed that complete blood count, blood urea nitrogen, creatinine, and electrolytes were normal; total creatinine kinase, 133 mg/dL; creatinine kinase-MB fraction, 4.1; Relative Index, 4.1; and Troponin (I), 2.1. Urine drug screen was positive for cocaine metabolites. Chest X-ray showed mild cardiomegaly and prominent upper lobe vasculature, but no mediastinal widening (Figure 1). A 12-lead electrocardiogram revealed atrial flutter, with a ventricular rate of 130 beats/min and nonspecific T wave changes.
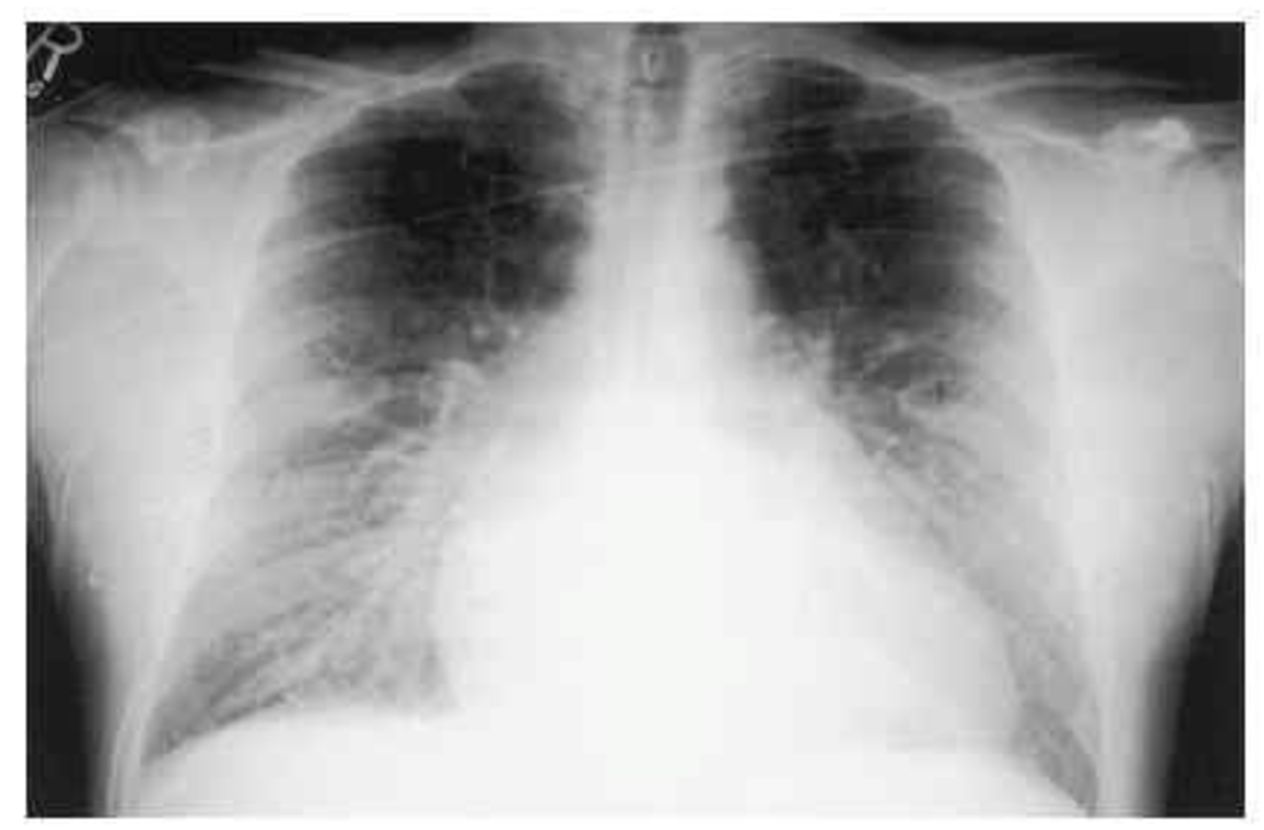
Chest X-ray on admission showing mild pulmonary congestion.
Initial diagnoses were mild congestive heart failure, cocaine-induced myocardial infarction with mitral regurgitation secondary to papillary muscle dysfunction, and cocaine induced atrial flutter. He was placed on 2 L/min of oxygen, given 40 mg of furosemide intravenously, and was started on diltiazem infusion with intravenous digoxin. He also received anticoagulation with intravenous heparin in view of the evidence of non-ST segment elevation myocardial infarction and atrial flutter.
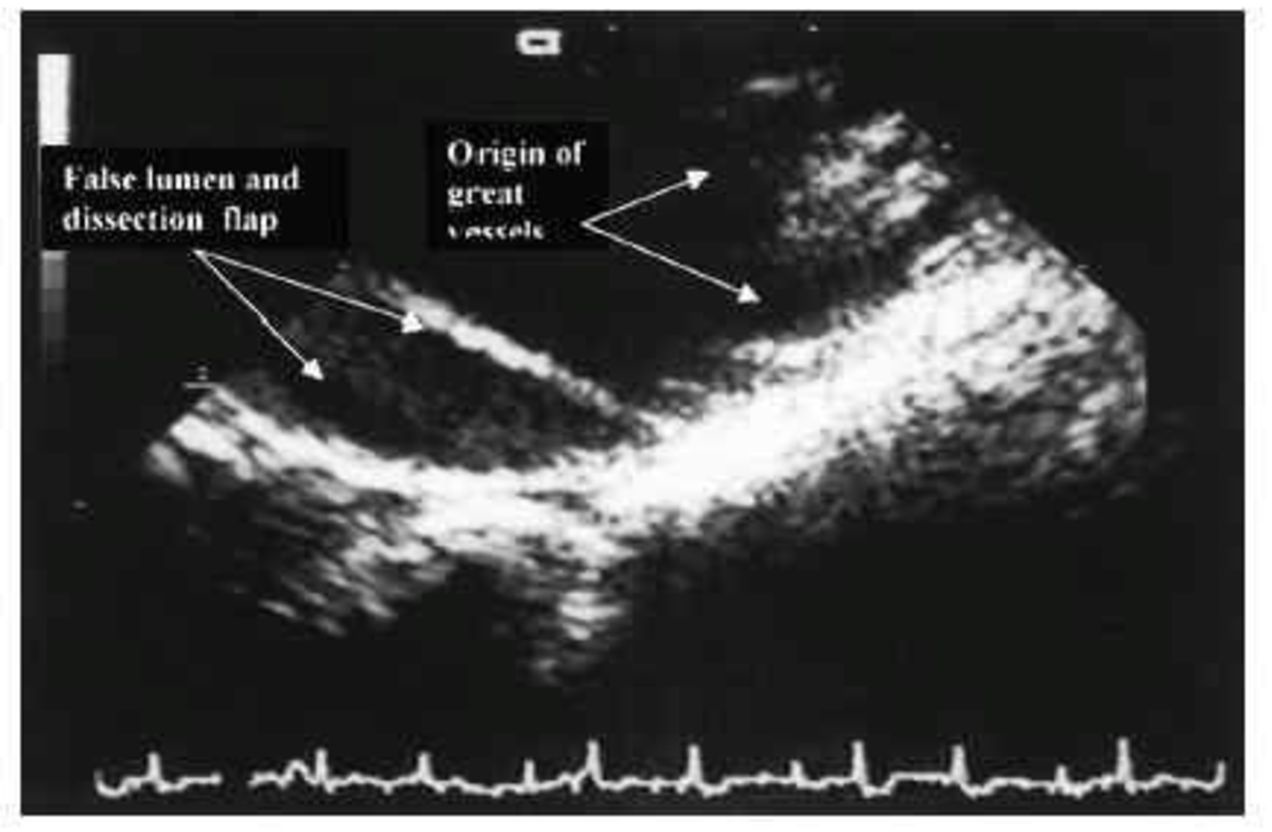
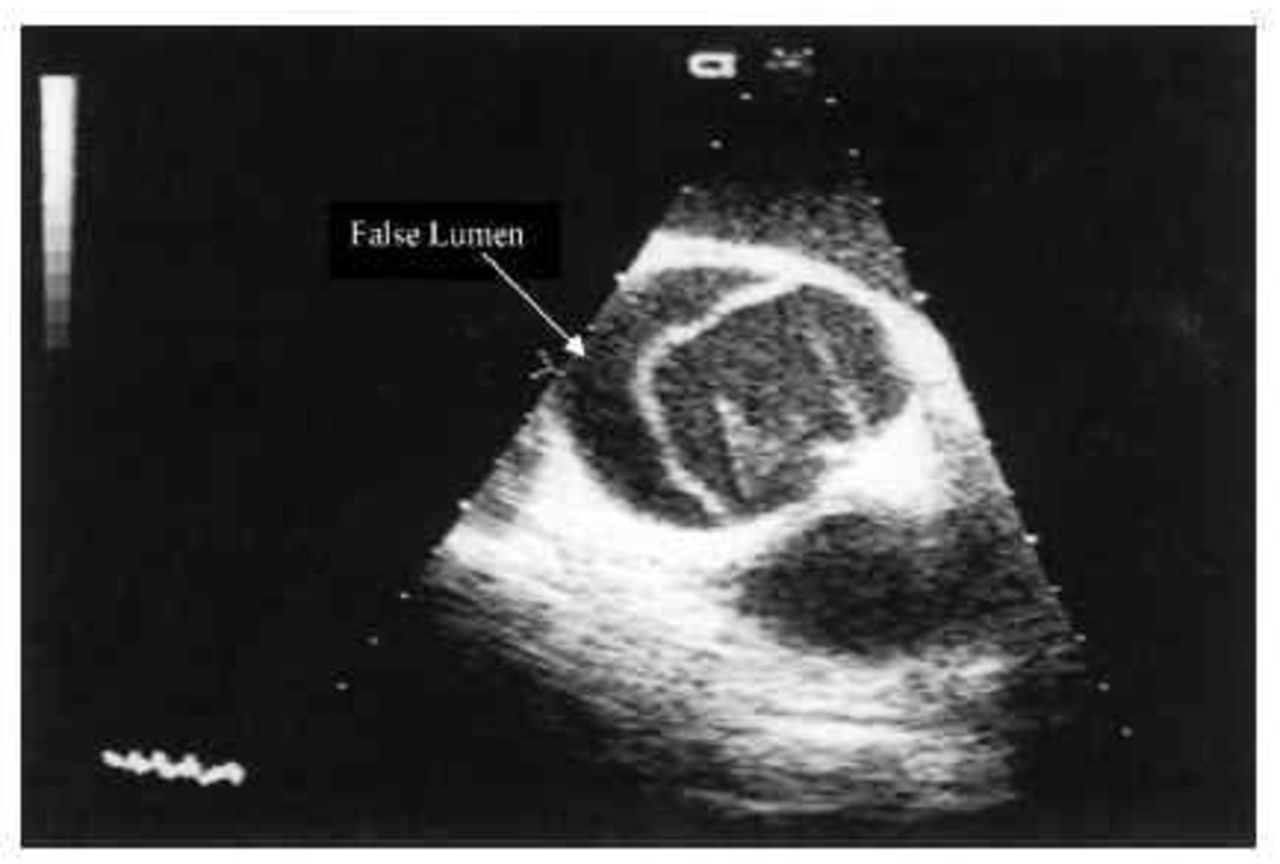
During the next several hours the patient became less short of breath and had no recurrence of chest pain, but remained in atrial flutter. He was transferred to intensive care unit, where a limited transthoracic, followed by a transesophageal echocardiogram (TEE) was performed, to evaluate mitral valve structure and to rule out left atrial thrombi before proceeding with direct current cardioversion. The transthoracic echocardiogram, to our surprise, showed severe aortic insufficiency, because no signs of aortic insufficiency were present on the physical examination. The presence of aortic insufficiency was confirmed by TEE, which also revealed ascending aorta dissection flap extending into the arch, but not involving the great vessels (Figure 2 and Figure 3). Mild to moderate mitral regurgitation was noted. Left ventricular wall motion and ejection fraction were normal. The intravenous heparin was immediately stopped and the patient was urgently transferred to the cardiothoracic unit of a nearby hospital where he underwent repair of the aortic root with Dacron graft and resuspension of the aortic valve. Coronary arteries were not involved. The postoperative course was unremarkable; the patient was discharged taking metoprolol 100 mg twice per day and amlodipine 10 mg once per day, with good blood pressure control on subsequent clinic visits. Follow-up imaging studies revealed no progression of the disease.
Transesophageal echocardiogram (short-axis view at aortic valve level), showing dissection flap and false lumen.
Transesophageal echocardiogram (view at the level of aortic arch), showing the dissection near, but not involving, the origin of great vessels in the neck.
Cocaine exerts a variety of deleterious effects on the cardiovascular system. The most common cardiac manifestation is chest pain 1 of myocardial ischemia. Cocaine can also lead to development of left ventricular hypertrophy, cardiac arrhythmias, coronary artery dissection, and congestive heart failure. 3 In addition to these cardiac effects, cocaine can also cause severe hypertension.
Cocaine abuse has been implicated in the pathogenesis of aortic dissection.4–11 Cocaine-induced dissection is usually present within hours of its ingestion, with severe chest pain; however, there are case reports of patients presenting with chronic Type A aortic dissection days or weeks after cocaine ingestion. The pathogenesis of cocaine-induced Type A aortic dissection is not clear, but acute hypertension plays a key role, with acute shear stress on the aortic wall. Anterior chest pain, the most common symptom of acute aortic dissection, contrary to generally held belief, can be sharp in nature and not classic severe tearing or ripping pain. 12 In addition, the other dissection findings, such as pulse deficit and mediastinal widening on chest X-ray may be absent in these patients. 6 The diagnosis depends upon a high index of suspicion, clinical findings, and immediate screening with an imaging modality, which is readily available. Transesophageal echocardiography is 99% sensitive and 97% specific for diagnosing aortic dissection, compared with 100% sensitivity and specificity of the newer generation of magnetic resonance imaging. 13 Immediate surgery is the treatment of choice in Type A aortic dissection, which, if left untreated, can have fatal consequences. 12
This is an interesting case of cocaine addiction, with a variety of cardiovascular manifestations of cocaine toxicity. The atypical nature of presentation and the presence of multiple cardiovascular toxicities, including atrial flutter, myocardial injury, and aortic dissection, in the same patient differentiate this patient from the sporadic cases of cocaine-related isolated aortic dissection in the literature. The patient was fortunate that a TEE was performed before cardioversion, which led to the correct diagnosis. We conclude that aortic dissection should be included in the differential diagnosis of chest pain in patients who screen positive for cocaine, even if the classical signs and symptoms are absent.