
Abstract
Background
This report summarizes a survey conducted in 2004 by the Association of Clinical Research Training Program Directors’ Evaluation Committee. The purpose of this survey was to determine the early capacity of the 59 National Institutes of Health (NIH) K30 programs (funded between 1999 and 2004) to produce clinical investigators trained in core skills required in clinical research.
Methods
In July 2004, a 37-item Web-based survey was distributed to institutions funded by the NIH K30 award mechanism. Frequencies and proportions were computed for each categorical response, and means were calculated for nominal responses using SPSS, version 11.5 (SPSS, Chicago, IL). Items 7 (funding year) and 8 (recruitment year) were cross-tabulated to ascertain the tempo at which programs were able to establish their enrolment processes.
Results
Forty-five of the 59 programs funded by the K30 award (76%) responded to this survey. The average number of active trainees in each program is 32. Women constitute 53% of active trainees, and 22% of them are underrepresented minorities. Ninety-six percent of active trainees have medical degrees. The average number of graduates over the 5-year funding period is 18. Of the graduates, 50% are women and 17% are underrepresented minorities. Fifty-six percent of them earned certificates, 44% earned master of science degrees, and 13% earned other degrees. Sixty-one percent of K30 program graduates have some extramural funding to support their research. The average number of publications per trainee for all trainees (active and graduate) is 2.3.
Conclusion
The K30 program has been a catalyst at multiple US institutions for improving the pedagogy for clinical research training. It has successfully fulfilled the mandate set forth by the 1998 NIH Director's Panel on Clinical Research (Nathan Report).
In 1998, the National Institutes of Health (NIH) Director's Panel on Clinical Research issued a report affirming the need to stimulate more clinical research in the United States. 1 One of the recommended actions was to promote clinical research training programs for physicians who choose this career pathway. In response, the NIH released a request for applications for clinical research curriculum awards (CRCA) to develop didactic training programs through the K30 award mechanism. The CRCA program is managed through the National Heart, Lung, and Blood Institute with input and financial support from other NIH institutes. Between 1999 and 2003, 59 academic institutions were granted approximately one million dollars each (direct costs) to develop and implement these programs. In 2002, their directors formed a nonprofit corporation, the Association of Clinical Research Training Program Directors (ACRTPD), which is dedicated to advancing and supporting the career development of clinician-scientists and the discipline of clinical research.
Program evaluation is a central goal of the ACRTPD. Therefore, the Board of Directors decided to assess the early impact of these programs between 1999 and 2004 to advocate for continued support from NIH. This report summarizes a survey conducted in 2004 by the ACRTPD Evaluation Committee. The purpose of this survey was to determine the capacity of the K30 programs to produce investigators trained in core methodologies required in clinical research. The data provide a “snapshot” of the range of programs and participants in the first 5 years of the CRCA.
Methods
A 40-item questionnaire was developed by a member of the ACRTPD's Evaluation and Accreditation Committee and was distributed to other committee members for review. After incorporating the Committee's feedback into the questionnaire, it was distributed to the ACRTPD's Communication Committee for a second review in preparation for an on-line format. On further modification, a 37-item Web-based survey was distributed to 59 institutions funded by the NIH K30 award mechanism and 2 institutions that receive their support from other sources. Program directors were contacted by electronic mail and were asked to complete the survey during a 3-week period in July 2004. A reminder was sent to all program directors during July, and a second reminder was sent to nonrespondents in August. Respondents were asked to provide their institutions’ names for tracking purposes only. This information was stripped from each record in the database prior to being given to the Evaluation Committee for analysis.
Data were analyzed using the Statistical Package for the Social Sciences (SPSS), version 11.5 (SPSS, Chicago, IL). Frequencies and proportions were computed for each categorical response, and means were calculated for numeric responses. Additionally, items 7 (funding year) and 8 (recruitment year) were cross-tabulated to ascertain the tempo at which programs were able to implement their enrolment processes following the award. Comments regarding the institutional impacts of the K30 programs were independently coded by two individuals and were analyzed for major themes.
Results
Forty-seven program directors responded to the survey. Two respondents were excluded from the analyses because the K30 award does not fund them; therefore, 45 of the 59 programs funded by the K30 award (76%) were included in this analysis. Of the 45 K30-funded respondents, 57% of them are publicly funded institutions, and their average rank for NIH funding is 42. Twenty-nine percent of the respondents are located at Midwest institutions, followed by middle Atlantic (20%), southern (20%), south Atlantic (11%), Pacific (9%), New England (7%), and Rocky Mountain states (4%).* The departmental homes of the programs vary, with many programs housed in departments of medicine, epidemiology, public health, or statistics. Eighty-four percent of the programs are affiliated with NIH-funded General Clinical Research Centers.
Mid-Atlantic: DE, DC, MD, NJ, NY, PA; Midwest: IL, IA, IN, KS, MI, MN, MO, NE, ND, OH, SD, WI; New England: CT, ME, MA, NH, RI, VT; Pacific: AK, CA, HI, OR, WA; Rocky Mountain region: AZ, CO, ID, MT, NV, NM, UT, WY; south Atlantic: FL, GA, NC, SC, VA, WV; southern: AL, AR, KY, LA, MS, TN, TX.
After three attempts to contact program directors, 14 K30-funded programs did not respond to the survey. Thirty-six percent of them are located in Midwestern, 21% in south Atlantic, 21% in southern, 14% in mid-Atlantic, and 7% in New England states. Their average ranking for NIH funding is 52 (excluding one institution that could not be found in the rankings and one institution that ranked nearly 300 places lower than the next highest ranking).
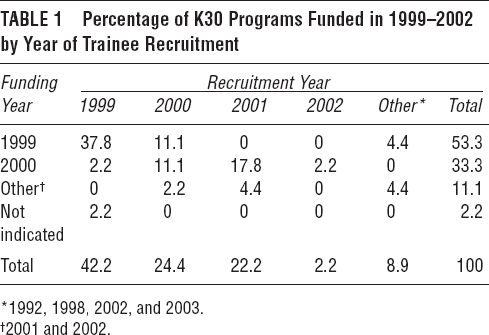
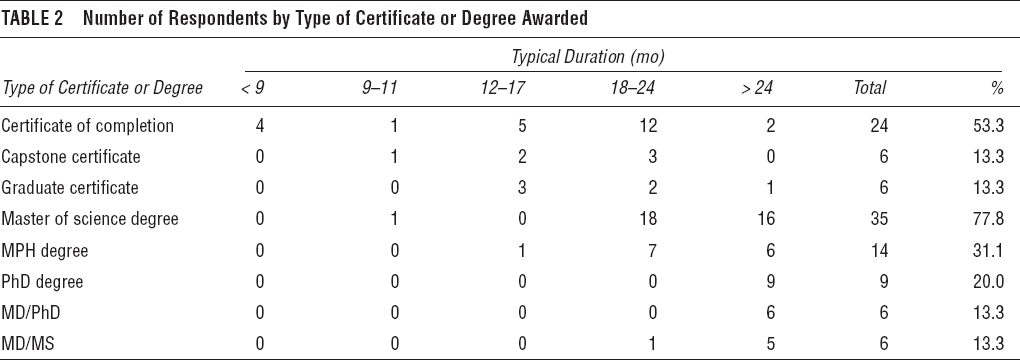
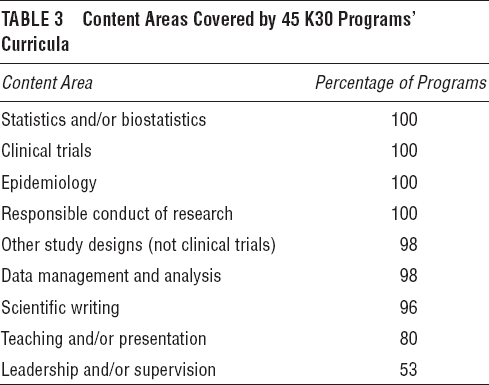
Fifty-three percent of the respondents were funded in 1999, 33% in 2000, and 11% in 2001 and 2002. Trainee recruitment usually began during the first year of funding. Forty-two percent of respondents began recruitment efforts in 1999, 24% in 2000, 22% in 2001, and 11% in other years. The percentage of responses by recruitment year and funding year is shown in Table 1 majority of respondents offer a formal (eg, a university-approved Capstone certificate for adult students wishing specialized job training) or informal certificate (80%) or a master of science (MS) degree (78%). Thirty-one percent offer a master of public health degree (MPH). Twenty percent offer a doctor of philosophy degree (PhD), and 26% offer a graduate degree (MS or PhD) in conjunction with a medical (MD) degree. Many of these are new degree programs, and most of them require at least 18 months of training (Table 2). Ninety-eight percent or more of the respondents indicated that the content of their curricula covers statistics and/or biostatics, clinical trials, study design (not clinical trials), data management and analysis, epidemiology, and the responsible conduct of research. Ninety-six percent of the respondents include scientific writing in their curricula, whereas 80% and 54% of the respondents, respectively, include leadership (and/or supervision) or teaching (and/or presentation) in their curricula (Table 3).
Percentage of K30 Programs Funded in 1999–2002 by Year of Trainee Recruitment
Number of Respondents by Type of Certificate or Degree Awarded
Content Areas Covered by 45 K30 Programs’ Curricula
The average number of active trainees in each program is 32. Women constitute 53% of active trainees, and 22% of them are minorities underrepresented in science. These proportions exceed those previously reported for research training programs.2,3
Ninety-six percent of active trainees have medical degrees, and 28% of them have salary and research support through individual K awards (eg, K01, K08, or K23) or institutional T32 or K12 awards. The K30 award typically supports 64% of the programs’ operating budgets, with other support coming from medical schools (21%) or other sources (18%).
The average number of graduates over the 5-year funding period is 18. Of the graduates, 50% are women and 17% are underrepresented minorities. Fifty-six percent of them earned certificates, 44% earned MS degrees, 6% earned MPH degrees, 4% earned PhD degrees, and 3% earned other degrees. Seventeen percent of graduates are principal investigators (PIs) on individual K awards, 11% are PIs on research awards (eg, R01 or R03), and 33% have nonfederal funding (eg, private foundation or industry support). Thus, 61% of K30 program graduates are PIs with some extramural funding to support their research.
The average number of publications per trainee for all trainees (active and graduate) is 2.3, representing a combined total of 116 publications for institutions responding to this survey.
Forty-three programs provided narrative comments (too numerous to list in this article) citing the multiple impacts of the programs on their institutions. Major themes that emerged from an analysis of the comments included (1) new or expanded interdisciplinary or multidisciplinary research collaborations, (2) K30 programs’ function as a core or central resource for investigators, (3) development of new courses and degree programs, (4) new grant proposals and awards, (5) increased awareness and visibility of clinical research, and (6) training program affiliations. Fundamentally, the CRCA programs are catalyzing changes in commitment to clinical research training, recognizing it as an essential component of many multidisciplinary research efforts. The institutional impacts of these programs are many and often extend beyond the boundaries of the K30 programs and their faculty and trainees.
Conclusions
This survey is the first attempt to document the impact of the K30 funding mechanism since the grants were awarded in 1999. The results of this survey reflect the important early effects that the K30-funded programs are having on the training of clinical researchers in the United States. Many of these programs are in a beginning stage of development. Twenty-five percent of respondents began recruiting trainees in 2002 or later and have likely just graduated their first cohorts. With an average of 18 graduates per program, nearly 800 health professionals, mostly physicians, have been trained during the first 5-year period; this is an underestimate of the total, given the incomplete response rate from all K30 programs. This number represents approximately $57,000 invested for each trainee and roughly $25,000 per publication, figures that will drop as the training programs mature.
Sixty-one percent of graduate trainees have independent funding, which is likely an underestimated figure because some trainees may have pending K awards—awards that are encouraged by program directors at the end of the K30 training period. This is an encouraging outcome because less than 20% of physicians trained on T32 awards eventually obtain funding as PIs on NIH grants, 1 whereas 28% of K30-trained physician-investigators receive NIH grants, as reported in this survey. Furthermore, it is interesting to note that 33% of graduates have nonfederal funding (eg, industry support or private foundation) for their research. This may explain Kotchen and colleagues’ findings that physicians are less likely to apply for R01 grants following their K awards when compared with their nonphysician colleagues. 4 Pharmaceutical companies often fund clinical studies, specifically clinical trials. It is likely that physicians frequently turn to this source of support when seeking research funding.
Fifty-three percent of the trainees are women, and nearly all of them appear to finish their training program. This is an encouraging figure because 49.7% of medical school graduates are women, 5 but only 14% of tenured faculty in academic medical centers are women. 6 Twenty-two percent of active trainees are underrepresented minorities, and approximately three-fourths of them have graduated, indicating the programs’ success at recruiting these individuals. These figures exceed those for underrepresented minorities reported for other clinical research training programs.2,3
The major limitations of this survey are the incomplete response rate and additional data that would further demonstrate the impact of the K30 programs and allow for some limited comparisons to other NIH-funded training programs, such as the Medical Scientist Training Program (MSTP). We suspect that because electronic mail was used to contact directors for their responses, messages may not have been read or program staff may not have followed through with the request for data. Requiring this information in a standardized format in annual progress reports to NIH would facilitate complete and accurate data collection on a program-wide level. Having this information turned over to an outside evaluator yearly could prospectively provide detailed analyses of a range of outcomes (eg, publication rates and impact, employment, NIH funding).
A second limitation was our failure to collect data that would help determine whether trainees are promoted to academic positions as a result of their participation in K30 programs. Additionally, data were not collected in sufficient detail to determine specific funding mechanisms that support these trained investigators or at what point in time they received a K award. Because K awards fund 9% of active trainees and 17% of graduate trainees have these awards, the survey data suggest that approximately half of them receive K awards after they complete the K30 programs. As with any survey, there are trade-offs between the purpose of the investigation, the level of detailed information requested, and the resulting response rate. Future efforts to collect data on the K30 programs could request this information with more formally defined evaluation requirements.
A third study limitation is the need to rely on self-report information from program directors. Although we believe that program directors can quickly refer to summary information regarding numbers of enrollees and graduates and racial and gender characteristics, we were not in a position to independently verify this. We do not have information about how accurately the program directors completed the survey. Prospective data, collected each year on each center's enrollees as part of a K30-wide program evaluation, would remedy this problem.
The CRCA program graduates nearly 800 clinician-investigators each year across 59 programs, at a cost of $12 million (FY 2004). These figures compare favorably to the MSTP (MD/PhD), which graduates about 150 physician-scientists across 40 programs at a cost of $31 million (FY 2000), and the former National Center for Research Resources-sponsored Clinical Associate Physician (CAP) program, which trained 260 clinical investigators over a 20-year period. The K30 program has been an effective catalyst at multiple US institutions for improving the pedagogy for clinical research training. It successfully fulfills the mandate set forth in the Nathan Report. The ACRTPD survey of K30 awardees highlights the promise of these programs and offers potential solutions for more rigorously evaluating their long-term success.
2003–2004 Program Evaluation and Accreditation Committee, Association of Clinical Research Training Program Directors
Footnotes
Acknowledgments
We would like to thank the members of the ACRTPD Communications Committee (W. Paul McKinney, MD, chair) for their efforts in providing suggestions for the survey and making it available to the association's membership through its Web site. Special thanks go to Christy Mayberry, who converted the survey to an on-line format, tracked responses, and provided data to the Evaluation Committee in a timely and efficient manner. The ACRTPD Evaluation Committee members who so diligently gave of their time and efforts to make this survey possible are listed in ![]() .
.