
Abstract
The advantages of endovascular aneurysm repair (EVAR) are probably related to the avoidance of the three major physiological insults associated with open abdominal aortic aneurysm (AAA) repair: laparotomy, aortic cross-clamping and ischemia reperfusion injury. Continuing aneurysm expansion indicates a failure to exclude the AAA from the circulation. We describe our experience with open surgery of post-EVAR sac expansion. A consecutive series of 68 EVAR patients was followed up. Endovascular and minimally invasive procedures were the initial treatment option. Failure of these attempts to curtail AAA sac expansion or type 2 large endoleaks (EL) resulted in opening of the aneurysm sac. The procedure includes positioning of a deflated occlusion balloon proximal to the stent graft (SG). Laparotomy with opening of the eneurysm sac was then performed. The thrombus was removed and backbleeding vessels oversewn. The aneurysm sac was then plicated over the SG. Four patients (5.9%) were diagnosed as having either persistent large type 2 EL or sac enlargement. In all patients the procedure was accomplished successfully. One patient died from acute myocardial infarction perioperatively. Three patients recovered uneventfully and follow-up computed tomography confirmed the absence of endoleak and a disappearance of the AAA. We believe that whenever EVAR fails to exclude the aneurysm from the circulation, open exploration without graft replacement should be considered.
The safety and efficacy of endovascular aneurysm repair (EVAR) in preventing abdominal aortic aneurysm (AAA)-related deaths, with a reduction in perioperative mortality, have been proven in large-volume studies. 1 Deployment of an aortic endoluminal stent graft (SG) avoids the three major physiologic insults associated with open AAA repair: laparotomy, aortic cross-clamping, and ischemia reperfusion injury. Although the surgical insult of EVAR is significantly less than that of open repair, 1,2 the results do not appear to be as durable as those for open aneurysm repair in terms of persistent exclusion of the aneurysm sac from the circulation. Approximately 15 to 27% of EVAR patients ultimately require secondary intervention in some form or other 3,4 and as such require lifelong postoperative surveillance.
Continuing aneurysm expansion following EVAR indicates ongoing pressurization of the sac and a failure to exclude the AAA from the circulation. This is usually due to the presence of an endoleak (EL), although sac expansion in the absence of a demonstrable EL, so-called “endotension,” has been documented. 5 Persistent type 2 EL (backbleeding from the lumbar or inferior mesenteric artery) and sac expansion have been shown to be more frequently associated with reintervention following EVAR. 6 The optimal management of this clinical scenario has yet to be defined, and the variety of reported treatments serves to highlight the confusion surrounding this issue.
Open AAA sac exploration has been described in cases of endotension. 7 Herein we describe our experience with open surgical management of aneurysm sac expansion owing to type 2 endoleak or endotension where previous minimally invasive treatment methods had failed.
Patients and Methods
From April 2001 to April 2004, a consecutive series of 68 patients who underwent elective EVAR of an AAA at Sir Charles Gairdner Hospital were entered into a prospectively maintained database. The devices used were the Zenith (W.A. Cook, Brisbane, Australia) in 65 cases (95.6%) and the Talent (Medtronic, Santa Rosa, CA) in 3 cases (4.4%). In 11 cases (16.2%), a Zenith fenestrated graft (W.A. Cook) was used.
Patients were followed up with clinical review and a computed tomographic (CT) scan at 1, 6, and 12 months and once yearly thereafter. The mean follow-up was 15.2 months (range 1–36 months). End points were 30-day mortality, late mortality and morbidity, sac shrinkage, secondary intervention rate, and the presence of EL. Type 2 ELs were managed conservatively provided that the aneurysm sac did not increase in size. ELs persisting for more than 6 months or ELs associated with sac expansion were subsequently investigated with a digital subtraction angiogram (DSA), with selective cannulation of the superior mesenteric and internal iliac arteries. This served to exclude a type 1 or type 3 EL and identify a potential source of a type 2 EL. Plain abdominal films were examined in patients demonstrating an increase in AAA sac size but with no demonstrable EL on either CT or DSA to rule out stent disruption or migration. Coil embolization of the lumbar arteries and laparoscopic clipping of the inferior mesenteric artery were employed when these vessels were identified as the source of a type 2 EL. Failure of these attempts to obliterate the EL or curtail AAA sac expansion resulted in the patient undergoing open AAA sac exploration and oversewing of the source of the EL (Figure 1).
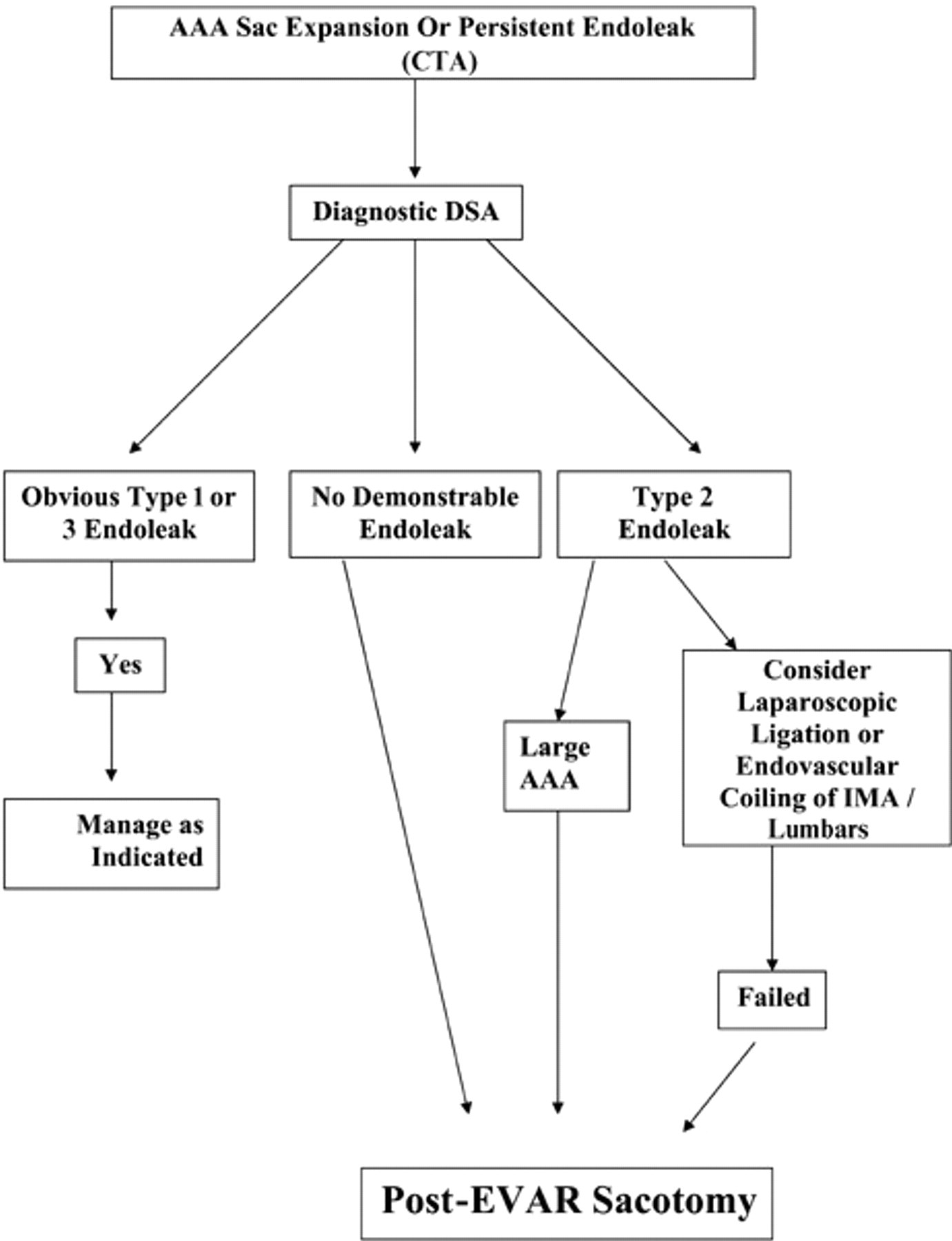
Algorithm for management of post–endovascular aneurysm repair (EVAR), abdominal aortic aneurysm (AAA) sac expansion, or persistent endoleak. CTA = computed tomographic angiography; DSA = digital subtraction angiography.
Under general anesthesia and fluoroscopic guidance, an aortic occlusion balloon (Zenith AAA Moulding Balloon, W.A. Cook) was introduced via an exposed right femoral artery and positioned deflated in the aorta proximal to the SG. Through a midline laparotomy, the AAA was exposed as per a standard open repair and a longitudinal aortotomy was performed, taking care not to damage or disturb the previously placed endoluminal graft. All intraluminal thrombus was removed, and visible backbleeding vessels were oversewn. The aneurysm sac was then plicated over the SG. Postoperatively, patients were followed up as per the protocol described above.
Results
The 68 patients included 56 men (82.4%) and 12 women (17.6%). The mean age was 75.3 years (range 56–94 years), and the mean aneurysm size was 57.9 mm (range 32–85 mm). The time interval from endovascular graft deployment to open exploration ranged from 1 to 33 months.
The secondary intervention rate was 11.8% (8 patients). Four patients (5.9%) were diagnosed as having either persistent type 2 EL (2 patients) or endotension (2 patients). Of the two patients with persistent type 2 ELs, one underwent an attempted laparoscopic clipping of the inferior mesenteric artery, the presumed source of the EL. Intraoperatively, the aneurysm sac was inadvertently penetrated and the patient required an emergency open conversion. The second patient with a persistent type 2 EL had previously had a fenestrated EVAR. Coil embolization of the presumed source of the EL, two lumbar arteries, was unsuccessful, and the AAA sac continued to expand. In one patient with presumed endotension, at the time of surgery, significant backbleeding from the lumbar arteries was encountered once the mural thrombus had been evacuated from the AAA sac (Figure 2). In the other patient with presumed endotension, the AAA was pulsatile, but no backbleeding was identified. It seems that the pressure was transmitted to the fluid content of the AAA. In three patients, postoperative recovery was uneventful and follow-up CT confirmed the absence of endoleak and a reduction in AAA sac diameter. The fourth patient died from acute myocardial infarction within 48 hours of surgery.
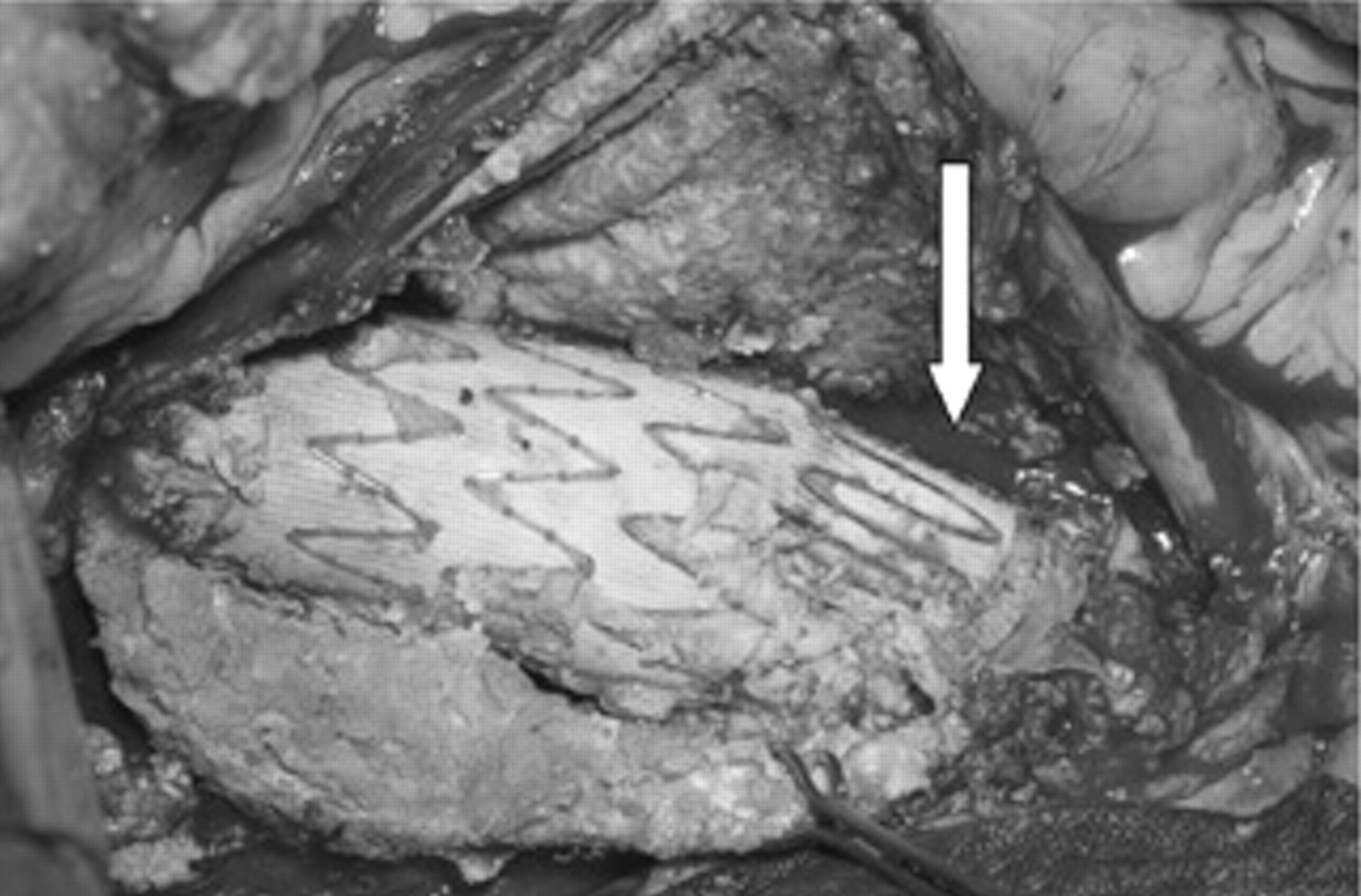
Abdominal aortic aneurysm sac opened revealing a stent graft with bleeding from the lumbar artery (arrow).
Discussion
Few would dispute the need to intervene in situations in which the AAA sac continues to expand following treatment, irrespective of whether an EL is demonstrated. The four cases in this series in which open surgical repair was employed represent the last step available to the surgeon in the algorithm of EL management (see Figure 1).
Current limitations in endovascular technology and technique mean that, on occasion, the vascular surgeon must resort to open surgery to resolve post-EVAR complications. Such cases are important to the development of endovascular surgery as they expose inadequacies in the technique that need to be addressed if current standards of practice are to be advanced.
Despite the need to repair the endoleaks by means of open surgery, two of the three major insults of open AAA repair, placement of an aortic cross-clamp and ischemia-reperfusion injury, were avoided. Thus, the need to progress to open sac exploration should be viewed not as a treatment failure but rather as a satisfactory means of solving a difficult clinical complication of EVAR, which was still less traumatic than standard open AAA repair. The fact that one of the four patients in this series succumbed to a fatal cardiac event within 48 hours of surgery emphasizes how fragile many of these patients are and strengthens the case for the least invasive treatment option available. All four patients included in this series had exhausted all other minimally invasive options, and three patients made an uneventful postoperative recovery.
Follow-up has been according to the post-EVAR protocol, despite the fact that the aortic sac has been opened and plicated. Maintenance of a seal between the SG and the aorta still depends on radial compression force and the hooks and barbs of the uppermost stent. Stent migration could still theoretically take place; therefore, these patients should be followed up according to our standard post-EVAR protocol.
The placement of a deflated aortic occlusion balloon in the aortic lumen proximal to the SG is an important aspect of this procedure. As demonstrated in the patient whose AAA sac was inadvertently breached during attempts at laparoscopic inferior mesenteric artery clipping, this can result in torrential life-threatening hemorrhage. Control of such bleeding by conventional means in a patient with an aortic SG would require the application of a supraceliac cross-clamp, with associated visceral ischemia and all of its attendant complications.
EVAR is a relatively new treatment modality, having been first described by Parodi and colleagues in 1991. 8 The operation is still undergoing constant modification, along with the devices themselves. It is likely that as SG technology advances, the incidence of EL will decrease, as will the need to resort to open surgery, such as reported in this series. Comparisons drawn between open aortic surgery and EVAR are therefore unfair. 9
Although the decision to intervene in the presence of ongoing AAA sac expansion is a readily accepted one, more controversial is the situation in which the sac neither increases nor decreases in size following graft placement. Some advocate a conservative course of treatment for this scenario 10 ; others are more aggressive. 11 Dias and colleagues employ intraluminal pressure measurements from the AAA sac to help determine whether further intervention is warranted. 12
Endovascular intervention is the treatment method of choice for dealing with EL following previous EVAR. Failed attempts of minimally invasive treatment mandate open AAA sac exploration. Up to one-third of EVAR patients ultimately require some form of secondary intervention, 3,4,13 with endovascular methods possible in 70 to 90% of such cases. Laparoscopic clipping of the lumbar arteries feeding the aneurysm sac has been described as an option for dealing with type 2 EL and may be a last resort in the attempts to avoid recourse to open surgery. 14
The significance of persistent type 2 EL is controversial. A report from the EUROSTAR database in 2002 found type 2 EL not to be associated with increased risk of AAA rupture and conversion, 15 whereas a later report from the same group concluded that type 2 EL is more frequently associated with AAA sac enlargement and reintervention. 6 Longer follow-up and correlation of results from databases and registries worldwide are required to resolve this issue.
In conclusion, we believe that whenever endovascular technology fails to exclude the aneurysm from the circulation, open exploration without graft replacement is a rational next step in the treatment algorithm.