
Abstract
Isolated mycotic common iliac artery aneurysms are rare, and as such, there is no consensus opinion on management. Traditional surgical options include resection with extra-anatomic bypass, placement of allograft or antibiotic treated synthetic graft, or autogenous vein reconstruction. We report the case of a 46-year-old, human immunodeficiency virus-positive male who presented with a recurrent pneumonia and new onset of right lower quadrant abdominal pain associated with right lower extremity swelling. computed tomographic scan revealed an isolated 9.5 cm right common iliac artery aneurysm with no evidence of rupture. Preoperative blood cultures grew out Streptococcus pneumoniae. Operative repair included aneurysm resection and reconstruction using an autogenous femoropopliteal vein interposition graft from the ipsilateral thigh. The patient had an uneventful recovery with resolution of his lower extremity swelling and a normal duplex exam at follow-up. Large mycotic common iliac artery aneurysms can be successfully treated with aneurysm resection and reconstruction using an autogenous femoropopliteal vein conduit. This technique obviates the need for extra-anatomic bypass or other forms of reconstruction using prosthetic material.
Case Report
A 46-year-old, human immunodeficiency virus (HIV)-positive male presented to the infectious disease clinic with fevers and shortness of breath in January 2006, 2 weeks after a previous admission for pneumococcal pneumonia. His chest radiograph showed persistent but decreasing bilateral consolidative opacities compared with his chest radiograph in December 2005. He was admitted for intravenous antibiotics and respiratory therapy. His CD4 count was greater than 600 cells/mm3, but the count was less than 200 cells/mm3 during his admission in December 2005. His HIV was diagnosed in 1998, and he was subsequently diagnosed with non-Hodgkin's lymphoma, which was treated with radiation in 1999. He has had no recurrence of lymphoma and has been maintained on antiretroviral medication since 1998.
During his hospital stay, the patient began complaining of right lower quadrant abdominal pain associated with right lower extremity swelling. On examination, he had a tender, pulsatile mass in the right lower quadrant with a markedly swollen right lower extremity. Computed tomography (CT) revealed an isolated 9.5 cm right common iliac artery aneurysm (CIAA) (Figures 1 and 2). Blood cultures were obtained and grew Streptococcus pneumoniae. A diagnosis of a mycotic CIAA was made, and preparations were made to take the patient to the operating room. Preoperative duplex examination of the right lower extremity revealed a patent deep venous system, with the femoropopliteal vein measuring from 0.84 to 1.09 cm in diameter.

Computed tomographic scan revealing a 9.5 cm right common iliac artery aneurysm.
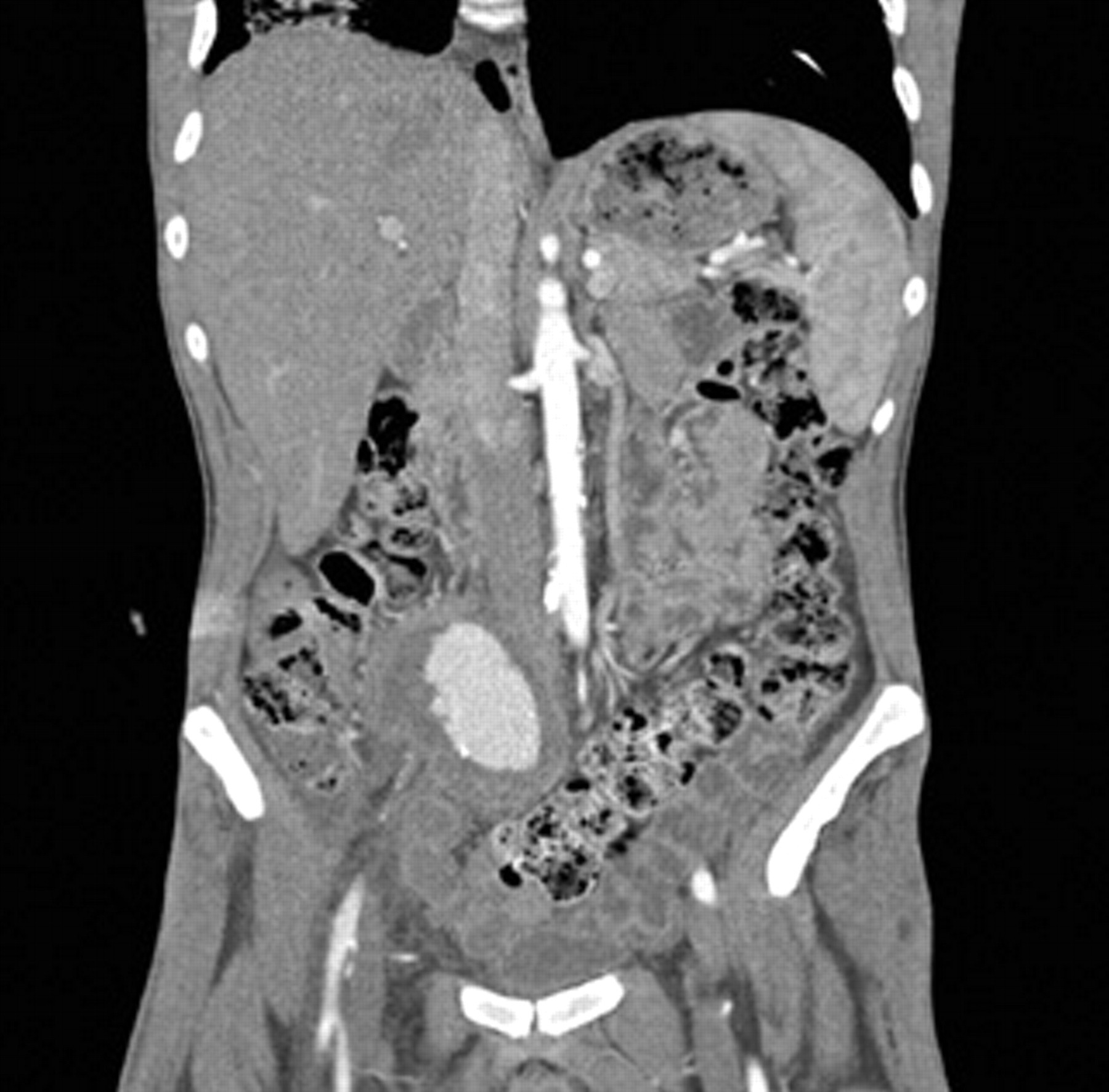
Coronal computed tomographic scan revealing a large right common iliac artery aneurysm with extrinsic compression of the right iliac venous system.
A lower midline incision was used to approach the aneurysm, where a dense, fibrotic reaction with adhesions to the small bowel and ureter was encountered. There was no evidence of free aneurysm rupture or contained leak. Proximal and distal control of the aneurysm was obtained prior to resection from the aortic bifurcation to the right external iliac artery. A partial-thickness injury to the right ureter, which was encased in the inflammatory mass, occurred and was closed primarily. Aneurysmal tissue was sent for culture and evaluation by pathology. Reconstruction was performed using a reversed femoropopliteal vein interposition graft harvested from the ipsilateral thigh. Branches of the femoropopliteal vein were doubly ligated prior to performing end-to-end anastomoses with the right common and external iliac arteries. The midline skin incision was left open for wet to dry dressing changes, whereas the thigh incision was loosely closed. A retrograde ureteral stent was placed cystoscopically at the completion of the case.
The patient had an uneventful postoperative recovery. He did experience persistent lower extremity swelling, and duplex ultrasonography was performed, with no evidence of deep venous thrombosis. His swelling was treated with leg elevation and compression stockings. The persistent swelling was attributed to postoperative inflammation causing persistent iliac vein compression despite his aneurysm resection. It is also possible that some of this swelling was also secondary to harvesting the femoropopliteal vein. Microbiology results on the operative tissue sample demonstrated no organism growth. Piperacillin-tazobactam and ceftriaxone were administered from the time of his admission until his discharge home on postoperative day 7, hospital day 16. At 1- and 2-week follow-up visits, his wounds were granulating and his right lower extremity swelling was markedly improved. He was seen in clinic 7 months postoperatively and had no right lower extremity swelling or pain. His wounds had completely healed, he had palpable pedal pulses, and arterial duplex imaging of the reconstructed iliac artery was normal.
Discussion
Isolated CIAAs are rare, with a reported frequency of 0.03% in one autopsy series. 1 There have been multiple reports of mycotic CIAAs in the literature, but their true incidence is unknown. 2–7 The etiology of mycotic aneurysms varies, but increased risk appears to be associated with an immunocompromised state, bacteremia, a history of intravenous drug abuse, and advanced age (or any combination of the above). 4,8,9 There is frequently a concomitant source of infection, but this does not appear to be absolute. 8 Microbial pathogens cultured from these aneurysms vary, but Salmonella, Staphylococcus, and Streptococcus species are frequently implicated. 7 Reports of iliac artery aneurysm infections involve a wide range of other microbes, including Klebsiella pneumoniae, Acinetobacter baumannii, Candida albicans, and Clostridium septicum. 2–8
Surgical management of mycotic iliac artery aneurysms is required to prevent rupture or thromboembolic events, control infection, relieve extrinsic compression of adjacent structures, and preserve blood flow to the lower extremity. 9 Following aneurysm excision and débridement, there are multiple options for revascularization, including extra-anatomic bypass, in situ graft replacement with an allograft or an antibiotic-treated prosthetic graft, or reconstruction with an autogenous vein. There have also been reports on successfully treating infected iliac artery pseudoaneurysms with endografts. 10,11 However, this technique should be used with caution as there is also a report of endograft failure and expulsion through a patient's wound. 12 An ideal reconstructive procedure should have minimal risk of postoperative graft infection with excellent durability and optimal blood flow.
A significant amount of literature exists regarding treatment of mycotic aortic aneurysms, much of which can be used to guide the management of mycotic iliac artery aneurysms. Extra-anatomic bypass is a well-described approach that can be performed in a staged fashion. It is considered by many to be the gold standard for repair of infected aortic aneurysms because it avoids placement of prosthetic material in an infected field. 13 Reported 5-year patency rates for axillary-femoral bypass (performed for occlusive disease) approached 75% in one series, although this figure remains controversial. 14 Femorofemoral bypass is another extra-anatomic consideration for a patient with a unilateral CIAA, but this approach still fails to restore in-line flow. Extra-anatomic bypasses carry the additional risk of aortic (or common iliac artery) stump blowout, and despite the placement of a prosthetic graft in a clean field, the potential for reinfection exists, with a reported risk as high as 20% in one series. 15
The use of antibiotic-treated prosthetic grafts or allografts in the repair of mycotic aneurysms has the advantage of in-line reconstruction for revascularization. Data from the aortic aneurysm literature suggest that in situ prosthetic grafts can be used after antimicrobial sterilization and operative débridement of infected aneurysms, with a reinfection rate of 10%. 16 Rifampicin-bonded grafts performed well in a study from Leicester, England, but a significant proportion of those patients (6 of 11) were treated for either aortoenteric fistula or graft occlusion, whereas cases involving methicillin-resistant Staphylococcus aureus aortic graft infections had poor outcomes. 17 Cryopreserved arterial allografts have been used by cardiac surgeons with reasonable success for some time. Their use in abdominal aortic infections has been successful from the standpoint of reinfection; however, the development of aneurysmal degeneration occurred in a significant percentage (17%) of patients in one series. 18
The use of an autogenous deep vein for neoaortoiliac system reconstruction (or NAIS procedure) is another approach to treating aortic graft infections and mycotic aneurysms. 9,19 The NAIS reconstruction relies on the availability of a suitable conduit (ie, femoropopliteal vein). In-line flow is reestablished with a low risk of reinfection while avoiding the risks of aortic stump blowout and the use of prosthetics in or near an infected field. 20 Harvesting the femoropopliteal vein appears to confer minimal morbidity, with a reported incidence of lower extremity swelling of less than 30% perioperatively and no reported major chronic venous changes after long-term follow-up. 21 Critics of this procedure argue that the prolonged operative time and inability to perform a staged procedure detract from its usefulness. Although this may be true for the NAIS reconstruction, an isolated common iliac artery reconstruction can be performed considerably faster.
In this case, we treated a mycotic CIAA with resection and reconstruction using an autogenous femoropopliteal vein because it allowed for infection-resistant in-line repair using a conduit with an excellent size and caliber match profile to the affected artery. Although the long-term patency of in situ autogenous superficial vein reconstruction of the common iliac artery is unknown, Clagett and colleagues showed excellent long-term results for the NAIS procedure, with a primary 5-year patency rate of 83% and a secondary patency rate of 100%, with no graft reinfections. 20 Our choice of procedure offered the greatest benefit to this patient in terms of infection resistance and avoidance of additional postoperative morbidity. The infection-resistant properties of autogenous vein reconstruction were particularly relevant to this patient given his HIV status and history of suboptimal CD4 counts. When feasible, mycotic aneurysmal disease of the aortoiliac system should be repaired using autogenous vein reconstruction over other alternatives.