
Abstract
We report our endovascular management of a highly kinked aortomonoiliac stent graft. This complication is unusual because kinks generally occur in bifurcated stent grafts and they are managed with extra-anatomic bypass. We will then expose the possible reasons for such complication. With long term follow-up severe kink might be reported more often.
Since the development of endovascular aneurysm repair (EVAR), different complications have been described following this technique. Changes in the shape and configuration of endovascular stent grafts have been reported during long-term follow-up. 1 In a large series of first-generation devices, Umscheid and Stelter demonstrated with 4 years of follow-up that 56.7% revealed some type of kinking of the endovascular aortic graft. 2 However, in this series and recently in the EUROSTAR registry, involving more recent devices, the incidence of kinking exceeding 90° was around 4%. 3 Moreover, it has been demonstrated that angulations up to 90° may favor graft limb stenosis, thrombosis, and graft migrations. 4 Despite many reports concerning the incidence of this complication, the literature remains poor concerning the endovascular management of severe kinking in an aortomonoiliac stent graft.
We report the case of an 80-year-old patient in a poor physical condition with an aortomonoiliac stent graft (Cook, Bloomington, IN) and a femorofemoral bypass left-right implanted 5 years before for a 53 mm maximum diameter abdominal aortic aneurysm (AAA). The preoperative angiogram showed an angulation of 133° between the aorta and the left iliac artery that was considered not significant. After stent graft implantation, this angulation was not modified. The stent graft had a one-piece configuration. After 5 years, the angulation was 95°, determining a subocclusive stenosis at the level of the kink (Figure 1). The aneurysm size was stable at 44 mm, without migration or endoleaks, and the patient was not complaining about claudication. Because of the risk of acute occlusion, we decided to treat the patient.
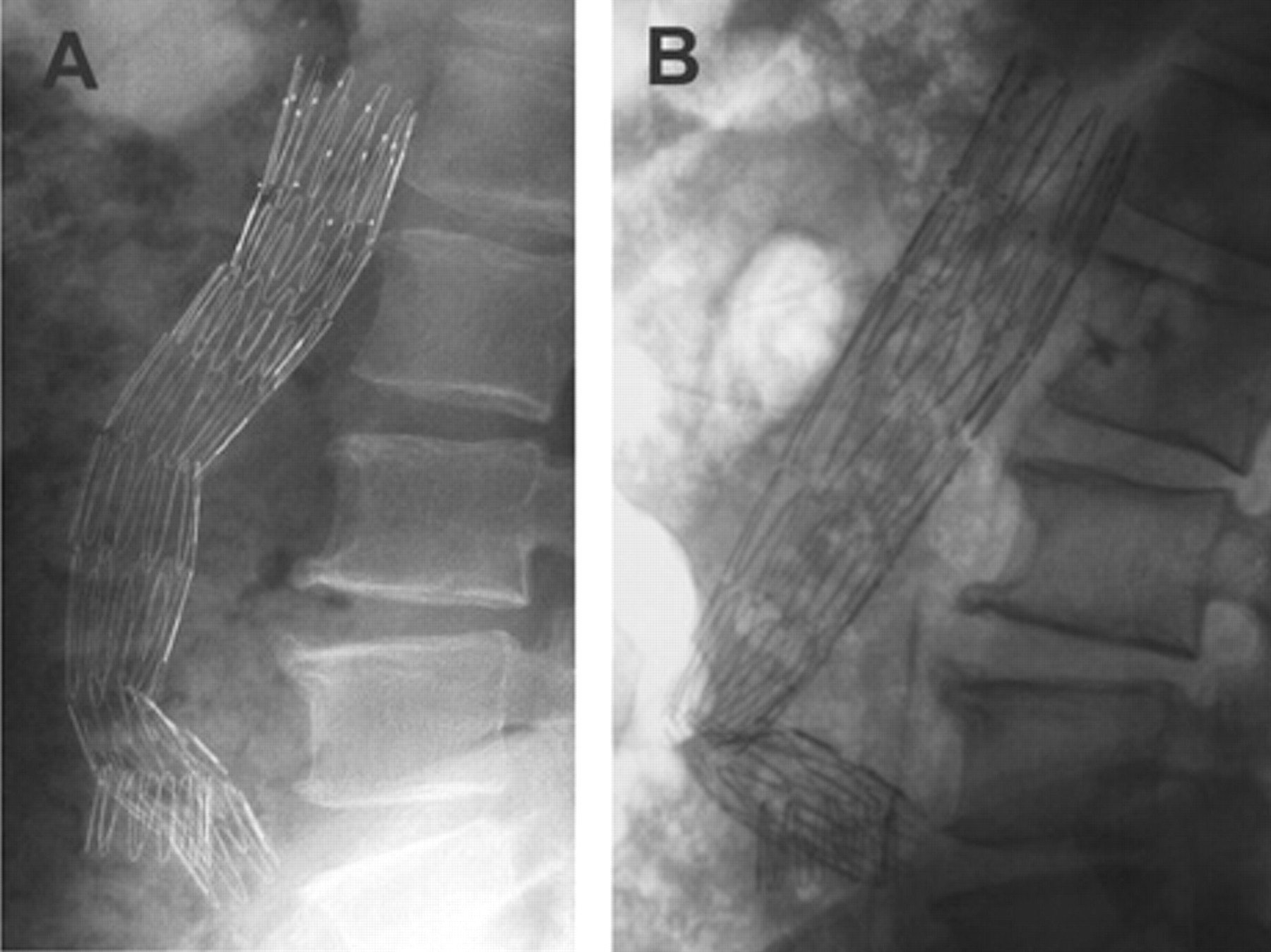
Evolution of stent graft shape over 5 years of follow-up, ending with a severe kink in the distal part of the device on a profile plain radiograph. A, Initial; B, 5-year control.
Procedure
Under general anesthesia, we did a surgical femoral access of the left groin. On this side, the initial starter wire was exchanged for a superstiff guidewire, the 180 cm Meier guidewire (Boston Scientific, Natick, MA), to provide extra support. The patient was heparinized with 5,000 UI of heparin. We first made several inflations with the compliant large balloon CODA-10.0-35-100-32 (Cook). As expected, we were able to reopen the stent graft lumen. To obtain an optimal result, we implanted a limb extension (nontapered stent graft), ESLE 22-55 (Cook), positioning the middle stent in front of the residual kinking of the stent graft. To remove the device launcher, we had to apply a manual pressure on the right side of the abdomen, the transition at the nose level blocking on the lesser curve of the newly implanted stent graft, and we feared to dislodge it. After positioning, we fully applied the device with a new series of balloon inflation. The final peroperative control showed the kink resolution without any migration or new endoleaks (Figure 2). The postoperative course was uneventful. Six months later, the patient did not complain about new symptomatology, and the computed tomographic scan showed that the reduction of the kink was maintained (Figure 3).
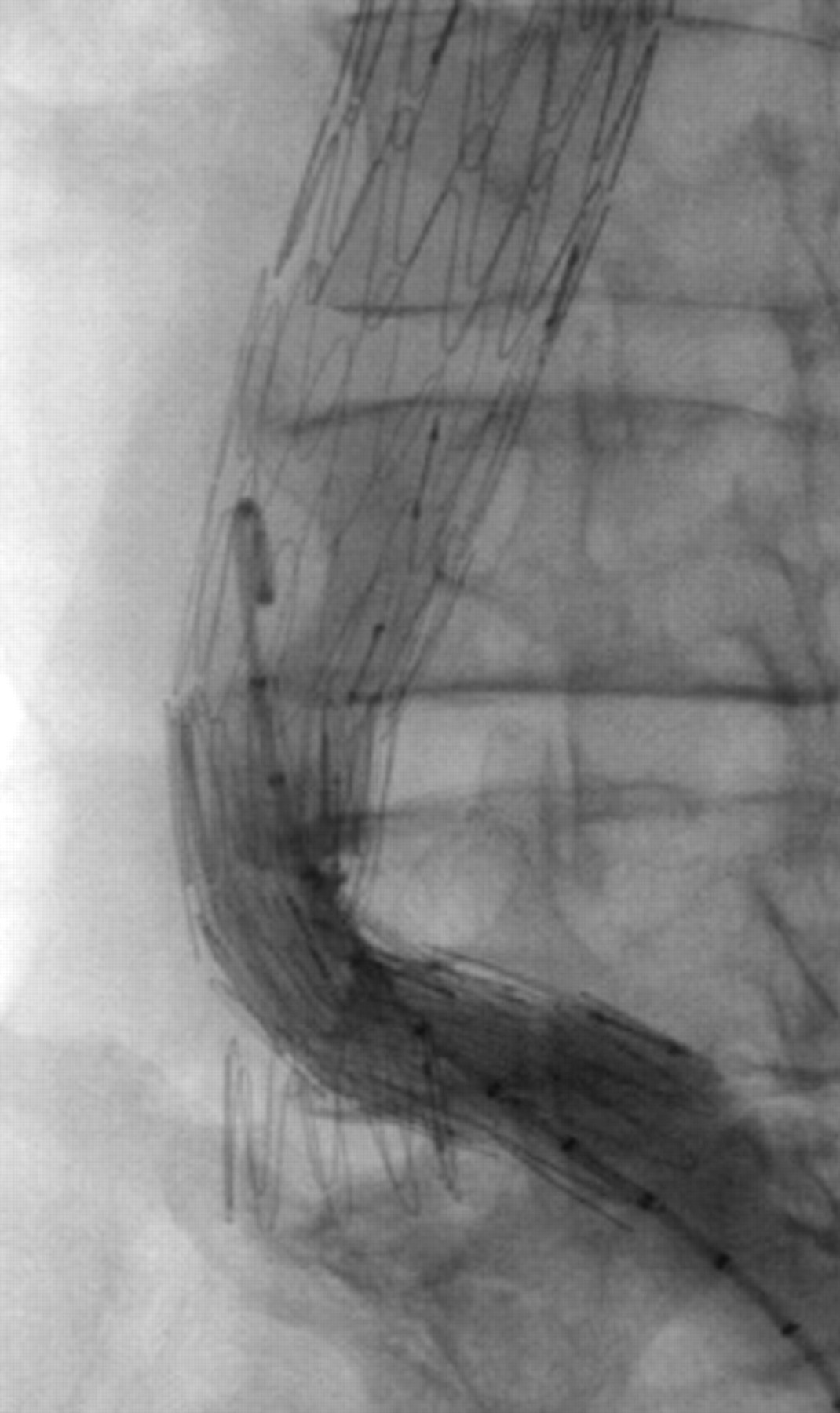
Angiographic control after implantation of the covered stent in the previous stent graft at the level of the kink.
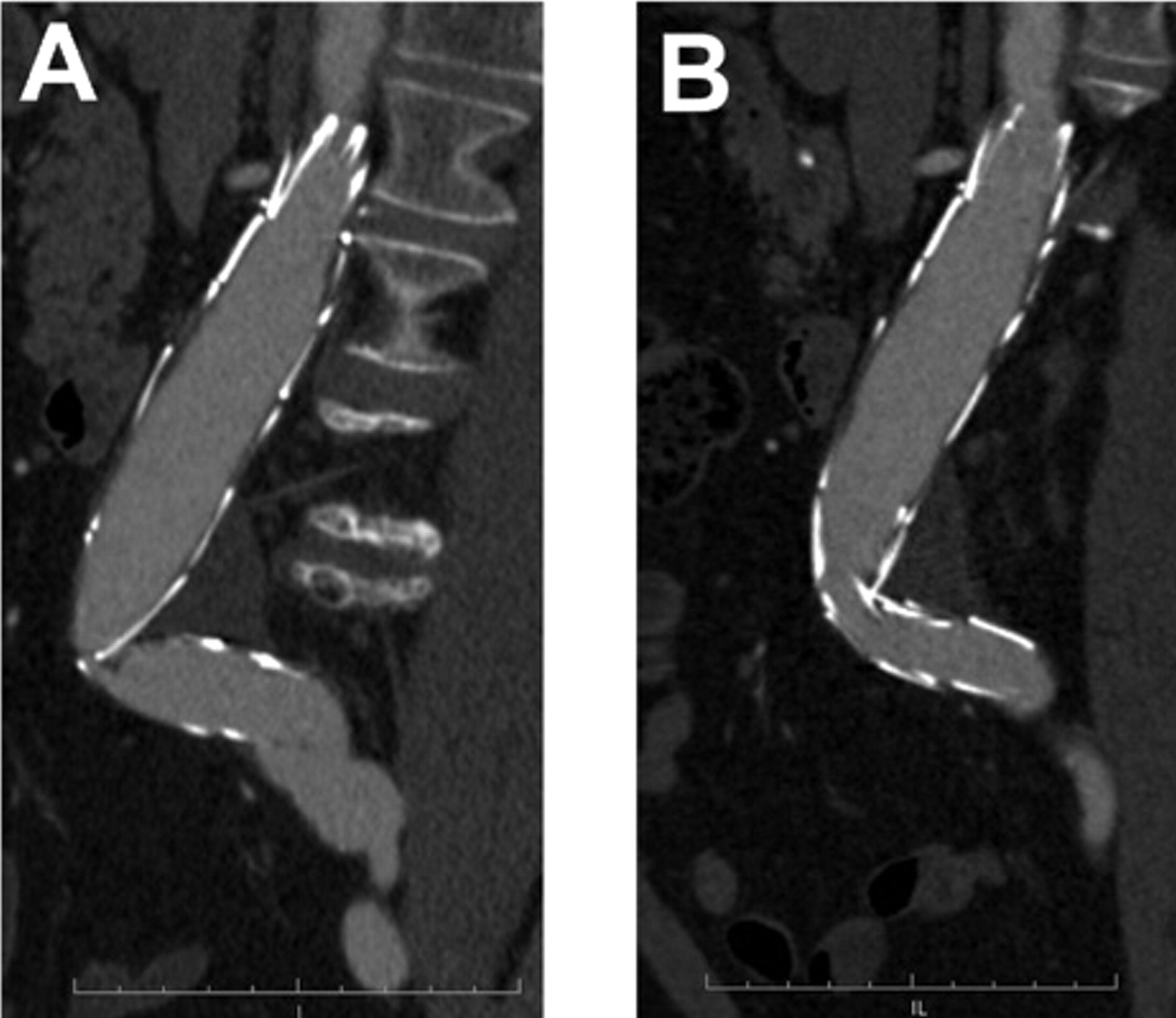
The results of the intervention, 6 months later, with computed tomographic two-dimensional multiplanar reconstructions (Osirix software). A, Preoperative; B, 6-month control.
Discussion
Late complications and secondary procedures remain the main drawbacks of EVAR. Stent graft kinking is one of the late complications observed. Reviewing the EUROSTAR registry, kinking exceeding 90° is managed conservatively in about 50% of the cases, and the rest of the patients are not always managed with endovascular techniques. Indeed, if the device is an aortobi-iliac prosthesis, it might be less invasive to perform a femorofemoral crossover bypass instead of an endovascular procedure when the kink is localized in one limb. In this case, the only surgical alternative is an axillary bifemoral bypass.
Different theories have been established concerning the kinking formation. 2,5,6 In this case, we did not observe migration of the stent graft at the level of the proximal or distal fixation after a limited sac shrinkage (ie, 52 to 48 mm maximum diameter). Interestingly, the vertical length of the stent graft, measured on the plain radiograph, was reduced by only 15 mm, leading to an increase in the angle between the fifth and sixth stent of 40°. We also observed the stretching of the proximal part of the device compared with the initial radiograph (see Figure 1). Independent stainless steel Z stent design provides graft flexibility; however, when the kinking is localized between two stents, it can lead to a high degree of graft stenosis. This observation illustrates that small modifications of the initial configuration of the stent graft may lead to severe angulations; therefore, it might be difficult to predict this kind of complication.
During the secondary procedure, the predilatation with a large compliant balloon had several advantages. First, during the first inflation, using a large field with the fluoroscopic C-arm, we were able to check the lack of movement of the stent graft, especially the proximal part in front of the renal arteries using bony marks. Second, after several inflations, we were able to evaluate the radial force needed to fully reopen the kink. It helped us select the appropriate device to implant. Finally, the balloon inflation decreased the severity of the stenosis, which facilitated the progression of the new stent graft at the level of the kink and increased the precision of the stent deployment.
We first ruled out implanting a large Palmaz stent (Cordis, Johnson and Johnson, Miami, FL), fearing to transfer the kink higher owing to the low flexibility of this stent. We also feared injuring the prosthesis Dacron with the edge of the stent struts, creating a type III endoleak. In the literature, this kind of complication has been described at the thoracic level. 7 Considering this possible complication, a second layer of Dacron created by the implantation of a covered stent was a security to implant, if needed, a Palmaz stent. We did not implant a nitinol stent, which has a good conformability, but after the balloon inflations, we thought that the radial force would be insufficient. The device extension used was tubular and not degressive on purpose to obtain a high radial force at the stenosis location.
The endovascular management of this complication remains unusual considering the relatively low rate of kinking requiring interventional management and the majority of bifurcated stent grafts. We advocate the predilatation of the stent graft and the use of an oversized covered stent. This observation emphasizes once again the need for a close follow-up of EVAR to obtain competitive results with surgery.