
Abstract
Takayasu arteritis is a chronic granulomatous vasculitis with multivessel involvement, causing significant mortality and morbidity in affected individuals. A 32-year-old patient with severe right common carotid stenosis underwent expanded polytetrafluoroethylene graft interposition to the carotid artery. A bare Wallstent endoprosthesis (Boston Scientific Medi-Tech, Natick, MA) was implanted for the abdominal aortic stenosis incidentally diagnosed during follow-up 1 year after the carotid operation while the disease was inactive. Close follow-up of the activity of the vasculitic process is warranted owing to the progression of the vascular lesions or formation of de novo lesions in Takayasu disease.
Takayasu arteritis is a chronic granulomatous vasculitis causing significant mortality and morbidity in affected individuals, causing stenosing or occlusing lesions and, rarely, poststenotic dilatations or aneurysms, resulting in ischemic syndromes of the involved vessels. 1,2 We report on a young patient who presented with abdominal aortic stenosis 1 year after surgery for carotid artery stenosis.
Case Description
A 32-year-old man of Azerbaijani origin with a previous history of severe right common carotid artery stenosis and left hemiparesia was diagnosed as having a 24.7 × 8.5 mm stenosing lesion in the infrarenal aorta on the first year follow-up computed tomographic (CT) angiogram. The abdominal aorta was spared on the initial admission (Figure 1). He had been hypertensive for over 6 months. At the initial operation 1 year previously, a carotid thromboendarterectomy was scheduled as he was experiencing transient ischemic attacks following the development of left hemiparesia; however, a complete endarterectomy with adequate flow was not possible owing to a highly necrotic vessel wall and fibrotic lumen. Interposition of an 8 mm Dacron graft (Gelweave, Sulzer Vascutek, Renfrewshire, Scotland) was eventually performed. The excised carotid artery specimen was sent for pathology, and chronic inflammatory changes were observed (Figure 2). The diagnosis of Takayasu arteritis was then made on the basis of the pathologic findings and the previously presented criteria regarding clinical and laboratory findings. 3 His disease status was then classified as type I (A2) according to Numano's classification but apparently was later transposed to +C status with abdominal aortic involvement.
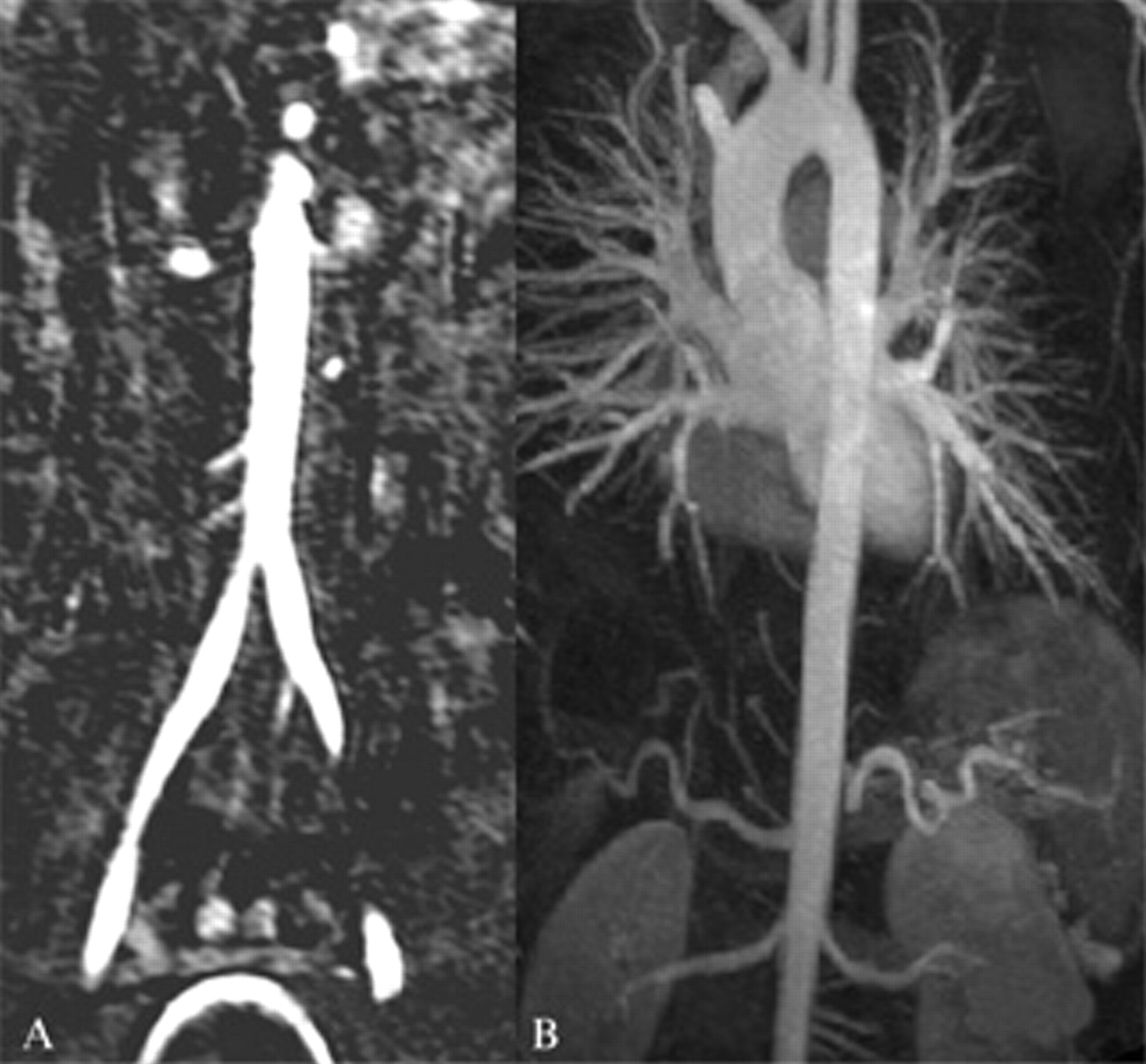
A and B, Right common carotid artery occlusion with normal abdominal and thoracic aorta at the time of the carotid operation.
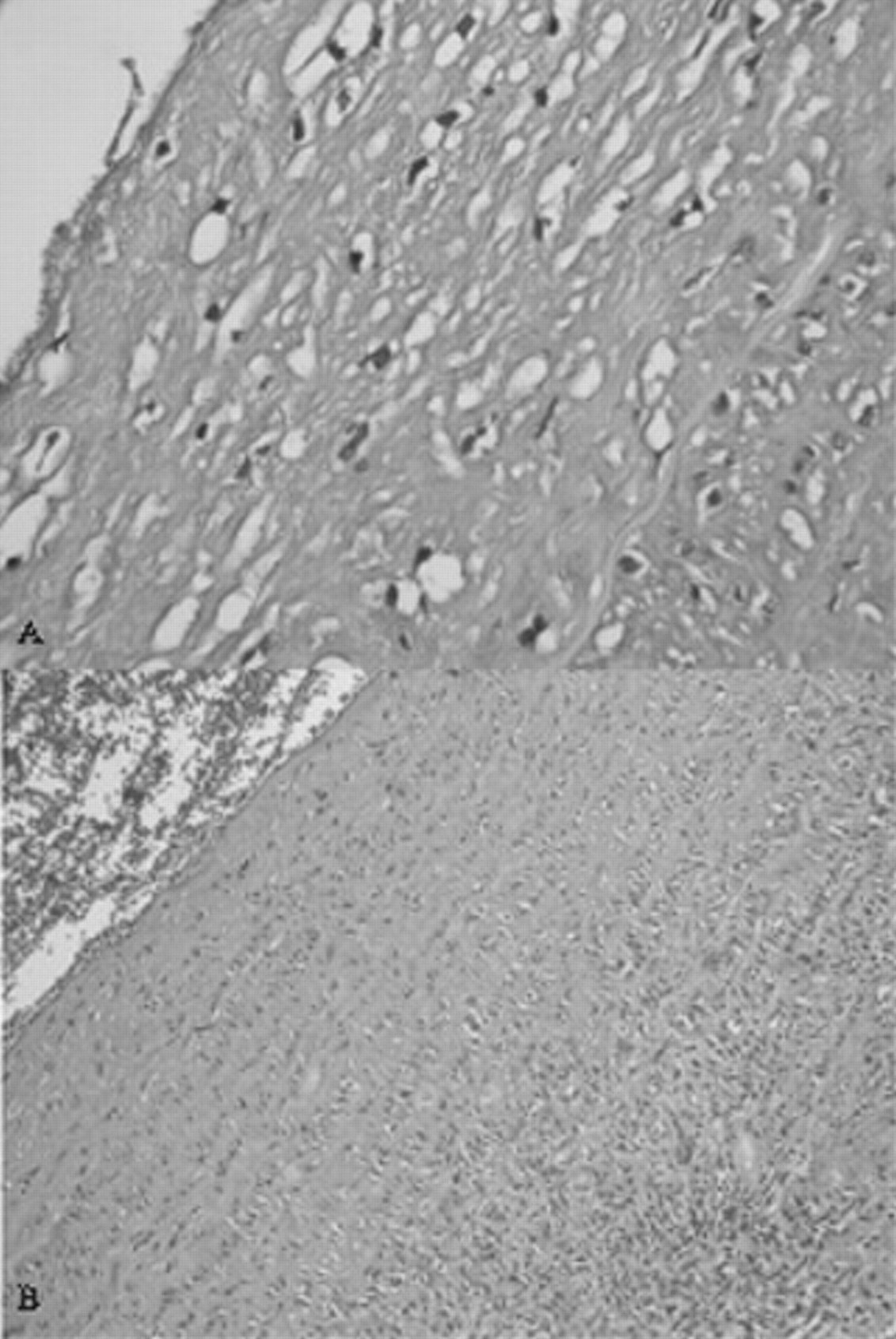
Histographs of the carotid artery demonstrating chronic degeneration (hematoxylin–eosin stain; ×20 original magnification). A, Areas of coagulation necrosis with rare residual viable intimal cells. B, Regenerative activity with neovascularization admixed with chronic inflammatory cells.
Elevated C-reactive protein and erythrocyte sedimentation levels yielded active disease, necessitating 100 mg/d of oral prednisolone and 325 mg/d of acetylsalicylic acid. However, an extra-anatomic aorta to right common carotid artery bypass with a 9 mm Dacron graft through a book-shaped ministernotomy was necessary following deterioration of the patient's neurologic status on day 1 owing to occlusion of interposed the graft (see Figure 1B). The patient's neurologic status recovered, and the levels returned to normal in 3 months, precluding immunosuppressive therapy; a gradual decrease in oral prednisolone dose to as low as 15 mg/d was possible in 6 months and to 5 mg/d in a year. Contrast-enhanced magnetic resonance imaging (MRI) of the thoracic and abdominal vascular structures at the time of carotid endarterectomy and CT angiography at the sixth month follow-up revealed a normal abdominal aorta with a patent carotid graft, in contrast to the CT angiogram at the first year (Figure 3). A bare self-expandable endoprothesis 40 × 20 mm in size (Wallstent, Boston Scientific Medi-Tech, Natick, MA) was inserted via the right femoral route with epidural anesthesia at the same stage with percutaneous transluminal coronary angioplasty (PTCA) and stenting to the left anterior descending (LAD) artery. Control CT angiograms demonstrated excellent deployment of the aortic stent with patent aortic side branches (Figure 4). The patient was discharged on day 1 without complications. He was normotensive on third month controls and was on 25 mg/d of metoprolol. Both the carotid graft and the aortic stent were patent, without complications, on 300 mg/d of acetylsalicylic acid and 5 mg/day of oral prednisolone 6 months after stenting.

A and B, De novo abdominal aortic stenosis 1 year after the carotid procedure.
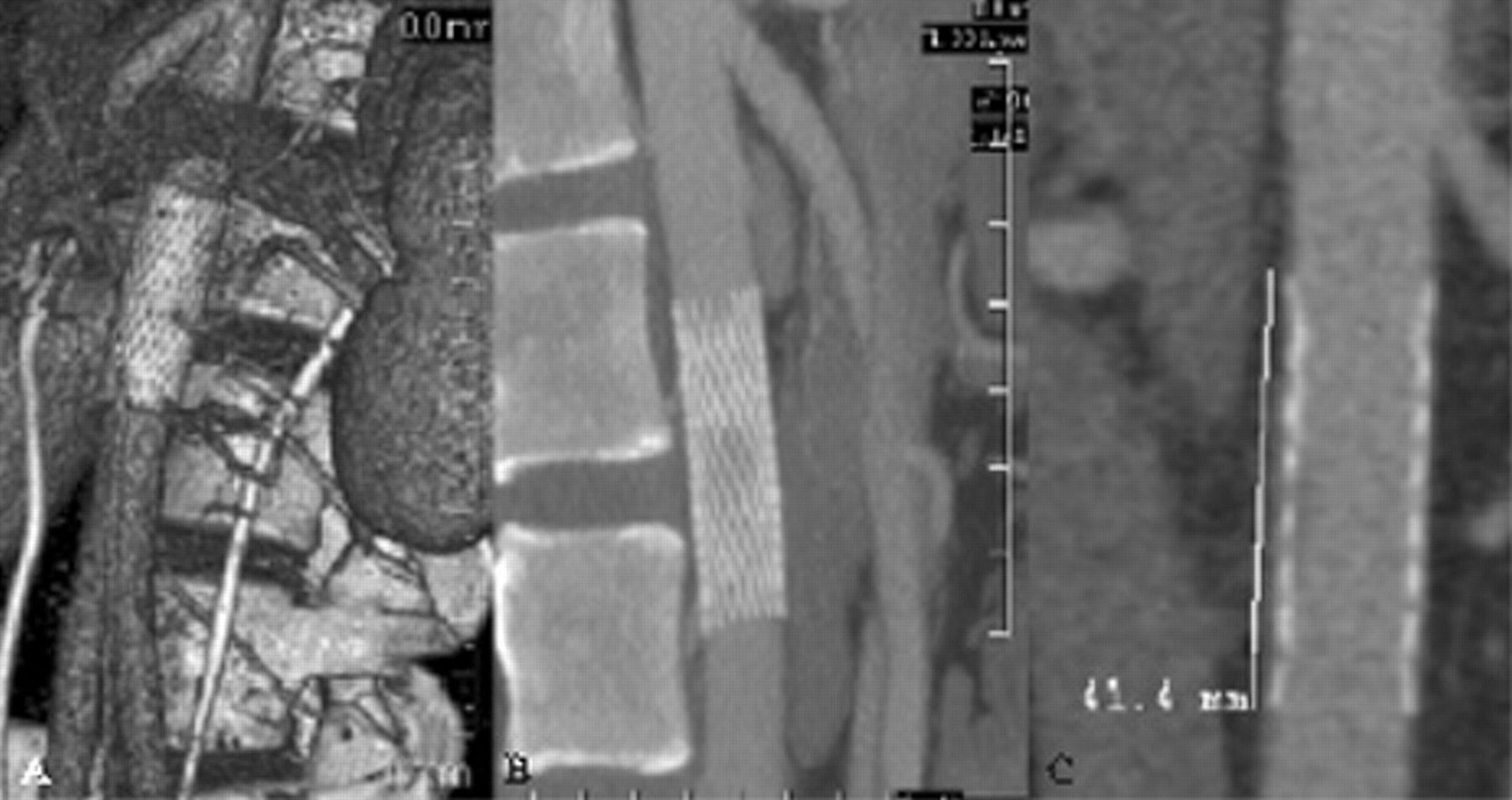
Bare Wallstent endoprosthesis in the abdominal aorta. Note that the rich collateral supply from the aorta is patent (A) in the segment covered by the bare stent (B and C).
Discussion
Takayasu arteritis is a chronic vasculitis commonly involving the aorta and its main branches, the brachiocephalic, carotid, subclavian, and renal arteries. Takasayu arteritis may cause a variety of ischemic clinical conditions with stenosis or occlusion of the involved vessels. 1 Media wall destruction may ensue in patients with more acute and progressive disease with aneurysmal formation and rupture. Cumulative data revealed a definitely high female to male ratio particularly in Asian countries and a relatively lower ratio in Turkey. 1 Our patient was a young man of Azerbaijani origin; some studies have suggested the confounding epidemiology of the disease and its manifestations, particularly in our region. 1,4,5
Our patient demonstrated a progressive presentation of the disease with carotid artery stenosis followed by development of a de novo abdominal aortic lesion after a possible active state within the following year. As stated, the abdominal aortic lesion was incidentally diagnosed and the patient was asymptomatic in this aspect and on low-dose prednisolone with normal C-reactive protein and erythrocyte sedimentation levels. Reduced aortic elastic properties in addition to a possible undetected, subclinical relapse of the vasculitic process may have contributed to this clinical outcome. 5,6 The extensive, progressive, and relapsing nature of the disease is strikingly different from that of atherosclerosis and influences the prognosis and the outcome of the intervention. In this patient, we performed a bare Wallstent endoprosthesis deployment for the preservation of a rich collateral supply to the intra-abdominal organs while the patient was stable in terms of vasculitis (see Figure 3) to avoid possible progression of the stenosing process following a relapse of the inflammatory process. It is noteworthy that a secondary benefit of using bare Wallstent endoprostheses for abdominal aortic lesions is the feasibility of future interventions for side branches covered by the endoprosthesis. 7 Numan performed endovascular therapy in 9 patients with stenotic lesions in the aorta among a cohort of 69 patients with Takayasu arteritis. 8 No compromise of any of the aortic side branches was reported.
Open surgery is the primary treatment of tubular aortic narrowing associated with renovascular hypertension and visceral artery stenosis. This entails aortoaortic bypass of the diseased segment or, less often, patch aortoplasty and, usually, bypass grafting of the stenosed renal and visceral arteries performed with autologous conduits, particularly in the youngest patients. Endovascular therapy may provide a sound, minimally invasive treatment caused by discrete aortic stenoses that do not encompass the mesenteric and renal arteries. 9 It is noteworthy that we performed endovascular stenting at the same stage with PTCA and stenting to the LAD coronary artery. This approach not only minimized surgical trauma to a patient with multivessel involvement on corticosteroids but also allowed quicker recovery with less intensive care or ward stay in addition to avoidance of multiple interventions and admissions. Delis and Gloviczki reported improved or cured hypertension following endovacular treatment in more than 70% of patients, 9 as occurred in our patient. The prognosis after uncompromised surgical reconstruction is rewarding in the mid- and long term in patients with congenital aortic coarctation but deteriorates in patients with aortoarteritis and recurrent inflammatory activity. 9 Moreover, open surgery is a complex approach owing to multisystem involvement with usually comorbidities; the variable extent of the disease in addition to reported cases of early and late anastomotic aneurysms and pseudoaneurysm formation. 10
Close follow-up for progressive or de novo vascular lesions in Takayasu disease is very important, as observed in our patient. Carotid involvement with abdominal aortic stenosis is not a common phenomenon without side branch involvement. F 18 Fluorodeoxyglucose (FDG) positron emission tomography is a noninvasive metabolic imaging modality based on the regional distribution of F 18 FDG that is highly effective in assessing the activity and extent of Takayasu arteritis. 11 Similarly, gadolinium-enhanced MRI may be used for follow-up to establish the active state of the vasculitic process. 12 Treatment of such aortic lesions with bare stents may enable future access to side-branch lesions.