
Abstract
Massive bleeding from a tracheostomy developed in a 65-year-old woman with stroke after successful conservative management of a minor tracheostomy bleeding episode. Temporary hemostasis was achieved, and angiography showed a tracheoinnominate fistula (TIF), a rare complication of tracheostomy. Open surgery was contraindicated in this patient, so endovascular repair using a stent graft was performed. Permanent hemostasis was obtained, and there were no immediate complications from the procedure. The patient never recovered from her stroke and died 2 weeks later. The endovascular approach may be a feasible alternative to surgical repair of TIF, especially in patients unable to tolerate an open procedure.
Tracheoinnominate fistula (TIF) is a rare and potentially fatal complication of tracheostomy. 1 It occurs in approximately 0.7% of patients with a tracheostomy, 2 generally within the first 3 weeks after stoma creation. 3 Only about 14% of patients with a TIF-related hemorrhage survive, and early recognition and surgery have been considered essential to survival. 4,5 However, even with expeditious surgical management, TIF-related morbidity and mortality rates are high. Challenges in TIF repair include controlling the bleeding and decreasing the risk of innominate arteritis, which can result in rupture of the surgical site. 6,7 Recently, endovascular repair has been suggested as an alternative to open repair of TIF. 8 We describe a case of TIF in which this approach was used successfully.
Case Report
A 65-year-old woman with stroke was admitted to our intensive care unit, and orotracheal intubation was established. Fifteen days later, a tracheostomy was performed uneventfully. On postoperative day 14, there was a small amount of bleeding from the tracheostomy, which was controlled by external compression. Two days later, however, a massive hemorrhage occurred. Open surgery was considered too risky because of the patient's general condition. Bronchoscopy was judged to be too time consuming and to pose a risk of worsening the bleeding. Therefore, temporary hemostasis was achieved with overinflation of the tracheostomy cuff, fluid resuscitation, and continuous external compression. Angiography showed a TIF (Figure 1) and tortuosity in the transition between the brachiocephalic and subclavian arteries.
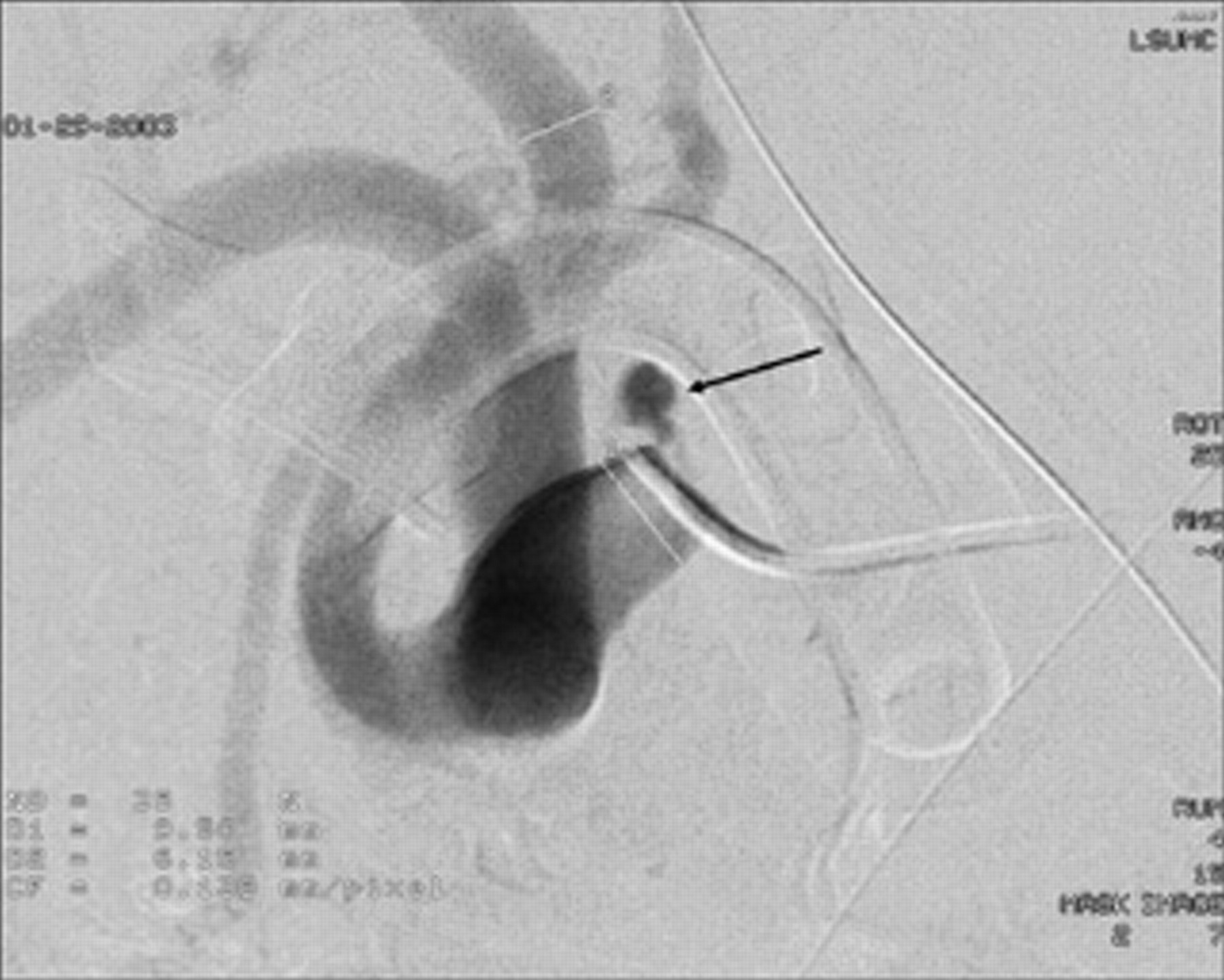
Arteriogram of the innominate artery shows the pathway of the tracheoinnominate fistula and extravasation of contrast material (arrow).
A 5F vertebral catheter (Boston Scientific, Natick, MA) was advanced distally to the fistula. Over a stiff exchange, an Amplatz guidewire (Boston Scientific) in the subclavian artery and a 10F long guiding sheath (Cook, Bloomington, IN) were positioned in the ostium of the brachiocephalic artery. A 0.025-inch guidewire (Boston Scientific) was then advanced to the proximal segment of the subclavian artery (Figure 2), and a 13 × 25 mm Viabahn stent graft (W.L. Gore & Associates, Flagstaff, AZ) was deployed over this guidewire in the innominate artery. The completion angiogram showed adequate stent graft placement and sealing of the TIF (Figure 3). Hemostasis was obtained, and the patient had no infection or recurrence of bleeding during the immediate postoperative period. Two weeks after the procedure, the patient's neurologic status worsened and she died.
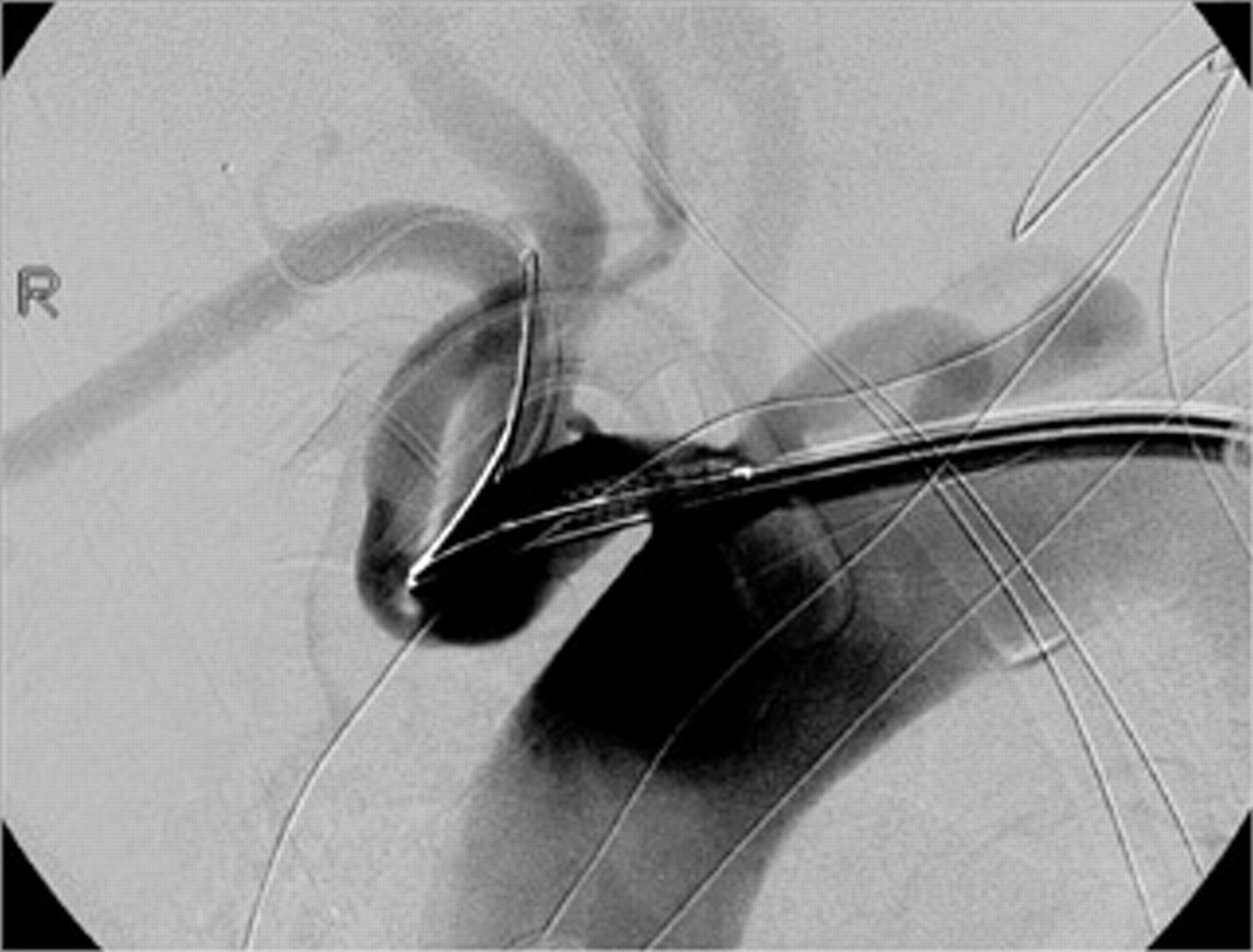
Arteriogram of the innominate artery obtained immediately before stent graft deployment.

Completion arteriogram of the innominate artery shows adequate stent graft placement and immediate sealing of the tracheoinnominate fistula.
Discussion
Although tracheostomies have been performed successfully for centuries, 9 about 0.7% of patients develop a tracheovasal fistula between the trachea and the innominate artery, 3,7 which traverses the trachea anteriorly at the level of the fifth or sixth tracheal ring. Fistula formation between the trachea and other structures (ie, the aortic arch, carotid artery, and innominate vein) has also been reported. 10
The first report of a TIF was published in 1879 by Korte, who observed the lesion in a child with diphtheria. 11 TIF can result from mucosal damage from the tracheostomy tube that leads to necrosis and fistulization with vascular structures in the pretracheal space. 2,5 Postmortem histopathologic studies have suggested a link between the mucosal necrosis and long-standing, high-pressure inflation of the tracheostomy tube cuff. 4,12 Other possible contributing factors are cuff overinflation, infection, low positioning of the stoma, and high location of the innominate artery. 6,8,12 However, the etiology of the TIF in our case report is unknown. By exclusion, the inadvertent overinflation associated with the period of time of endotracheal intubation most likely contributed to the TIF pathophysiology as there was no evidence of other etiologic factors.
Methods for preventing TIF include use of a low-pressure tracheal cuff, intermittent cuff deflation during long-term ventilation, minimal manipulation of the tracheostomy tube, sedation of an agitated patient, and immediate treatment of any tracheostomy infection. 4
TIF usually presents as an acute, brisk hemorrhage preceded by a minor bleeding episode that stops spontaneously in about 50% of patients. 3 Therefore, TIF should be included in the differential diagnosis of even minimal tracheostomy bleeding, especially if this is followed by hemoptysis. 1 Prompt investigation is essential because TIF has a high mortality. Easy control of bleeding with packing does not exclude TIF. 10 Aside from minimal tracheal bleeding, suprasternal pain with an irritable cough and pulsation in the tracheostomy tube have been reported as warning signs of a TIF-associated hemorrhage. 4,6,13,14
Any patient with suspected TIF should undergo angiography to confirm the diagnosis and facilitate an evaluation for endovascular treatment. Moreover, even if a fistula is not demonstrated angiographically, a strongly suggestive clinical history and presentation and a lack of response to conservative management may provide sufficient information to proceed with stent graft placement. 8
Successful endovascular treatment depends on the availability of stent grafts of various sizes or materials for creating a homemade device. A homemade device may be constructed with a metallic stent and vascular graft, but this is now seldom necessary because better stent grafts are commercially available. In our patient, we used a Viabahn endoprosthesis, which consists of a self-expanding, nitinol stent with a thin inner lining of expanded polytetrafluoroethylene. The device is available in lengths ranging from 25 to 150 mm and diameters of 5 to 13 mm, and it has an 8 to 12F profile. Because the Viabahn delivery catheter is 110 cm long, supra-aortic lesions can be treated through a percutaneous femoral approach.
During the stent grafting procedure, a long guiding catheter or introducer sheath is important for maintaining a stable access and allowing control angiography during device deployment. Innominate artery tortuosity may be present, as it was in our case. If the fistula tract is close to the origin of the carotid artery, a stiff exchange guidewire should be positioned in the carotid artery instead of the subclavian artery to maintain access to the carotid lumen if correction of stent misplacement is required.
Open repair of TIF, which involves sternotomy, is aggressive and associated with poor long-term results. Gelman and colleagues reported that only 40 of 71 patients survived for longer than 2 months after open TIF surgery. 13 Although the long-term results also were not very good in the present case report, the minimally invasive endovascular approach is attractive, especially for critically ill patients such as ours. So far, however, only a few cases of endovascular TIF repair have been reported. Deguchi and colleagues published the first endovascular treatment of a patient with TIF using a stent graft device. 8 The patient recovered uneventfully and remained well 14 months after the procedure, with no sign of infection. Vianello and colleagues reported on a 16-year-old boy with Duchenne muscular dystrophy who developed a TIF 26 months after tracheostomy. 15 The patient was treated using a Wallgraft device (Boston Scientific) and recovered uneventfully. Another patient with TIF related to peritracheal tumor invasion, radiation therapy, and tracheostomy was described by Wall and colleagues. 16 The fistula was initially excluded with a Viabahn stent graft, but a few weeks later, hemoptysis recurred secondary to deep tracheal erosion by the covered stent. The patient underwent surgical treatment but died owing to adult respiratory distress syndrome.
Endovascular or surgical repair could be followed by treatment with a broad-spectrum antibiotic agent to decrease the risk of infection, 8 although there are no good data showing that antibiotics given empirically in this type of situation actually reduce the percentage risk of infection. Also, the benefit of preventing infection in this scenario outweights the potential need for a thoracotomy and arterial bypass to treat local infection, procedures that theoretically increase the patient's morbidity.
Comparative studies including a substantial follow-up period are needed to determine whether endovascular repair of TIF is superior to open surgery with respect to effectiveness, safety, and financial cost. However, we suggest that an attempt be made to use stent grafting in all patients with TIF and that open surgery be employed only if this approach fails.
Footnotes
Acknowledgment
We thank Renée J. Robillard for editorial assistance.
C.S. is a consultant for W.L. Gore & Associates (Flagstaff, AZ).