
Abstract
Occasionally, standard stent grafts are not usable in emergency aortic bleeding, and custom-made stent grafts are not practical as a replacement. We describe a novel technique for the repair of such aneurysms by using the catheter-delivered liquid to solid embolic agent Onyx (Micro Therapeutics Inc., Irvine, CA). Two patients with ruptured aortic aneurysm, where endovascular or open repair was not considered as feasible, were treated by internal sealing of the aneurysm with Onyx, resulting in stoppage of bleeding and further expansion of the aneurysm-the plugging and sealing technique.
Endovascular aneurysm repair (EVAR) has proven feasible in acute operations of ruptured abdominal aortic aneurysms (rAAAs) and offers the potential for decreased morbidity and mortality. 1–8 Open repair is still an important method and is considered the only alternative in patients with a challenging anatomy, especially when sealing zones are insufficient. 2 A fenestrated stent graft is an option for a patient with a short infrarenal aortic neck or when there is a suprarenal extension of the aneurysm. 9,10 They are custom–made, and treatment of rAAA with fenestrated stent grafts in an emergency setting is therefore not very practical. The liquid embolic agent Onyx 34 (Micro Therapeutics Inc., Irvine, CA), an ethylene-vinyl-alcohol copolymer dissolved in dimethyl sulfoxide, has been used in the treatment of type II endoleaks after EVAR, 11,12 in embolization of peripheral vascular malformations, 13 and in the treatment of visceral aneurysms and pseudoaneurysms. 14 We treated one patient with acute bleeding from an aortic pseudoaneurysm and another with an aneurysmal aortic dissection by internal sealing with Onyx, thus resulting in the stoppage of bleeding and further expansion of the aneurysm-the plugging and sealing technique. We consider this to be a bridging technique to a later secondary intervention.
Case Report
Case 1
In June 2006, a 78-year-old woman underwent emergency open repair with a straight vascular prosthesis for a circulatory, unstable rAAA. In October 2007, she consulted the referring hospital with abdominal pain and fever and was initially observed at the hospital. As hemoglobin values decreased, 2 units of blood was given. Computed tomographic (CT) angiography showed a ruptured pseudoaneurysm measuring 7.7 × 6.0 cm in diameter with a left retroperitoneal hematoma (Figure 1). A broad-based neck was located at the level of the right renal artery. She had had her left kidney removed. Graft infection was considered, based on the medical history and location of the pseudoaneurysm. The patient was admitted to our vascular center. She was found to be unfit for an open repair and received an emergency endovascular procedure.

Ruptured pseudoaneurysm at the level of the right renal artery.
Through a left brachial access, a guidewire was directed into the pseudoaneurysm (Figure 2A) and shifted to a 4F Soft-Vu Berenstein catheter (AngioDynamics Inc, Queensbury, NY). An occlusion balloon (Equalizer Balloon Catheter, Boston Scientific/Medi-Tech, Boston, MA) was introduced through one common femoral artery in a percutaneously inserted 11F introducer sheet (Super Arrow-Flex, Arrow International Inc., Reading, PA). The balloon was inflated, covering the neck of the pseudoaneurysm-the cast technique-and the entire pseudoaneurysm was filled with 18 mL of Onyx (Figure 2B). The introducer was used to prevent migration of the inflated balloon. Repeated angiographies were performed through an angiocatheter, inserted through a femoral sheet on the contralateral side. After Onyx injection was completed, the balloon was expanded for another 5 minutes and then deflated (Figure 2C).
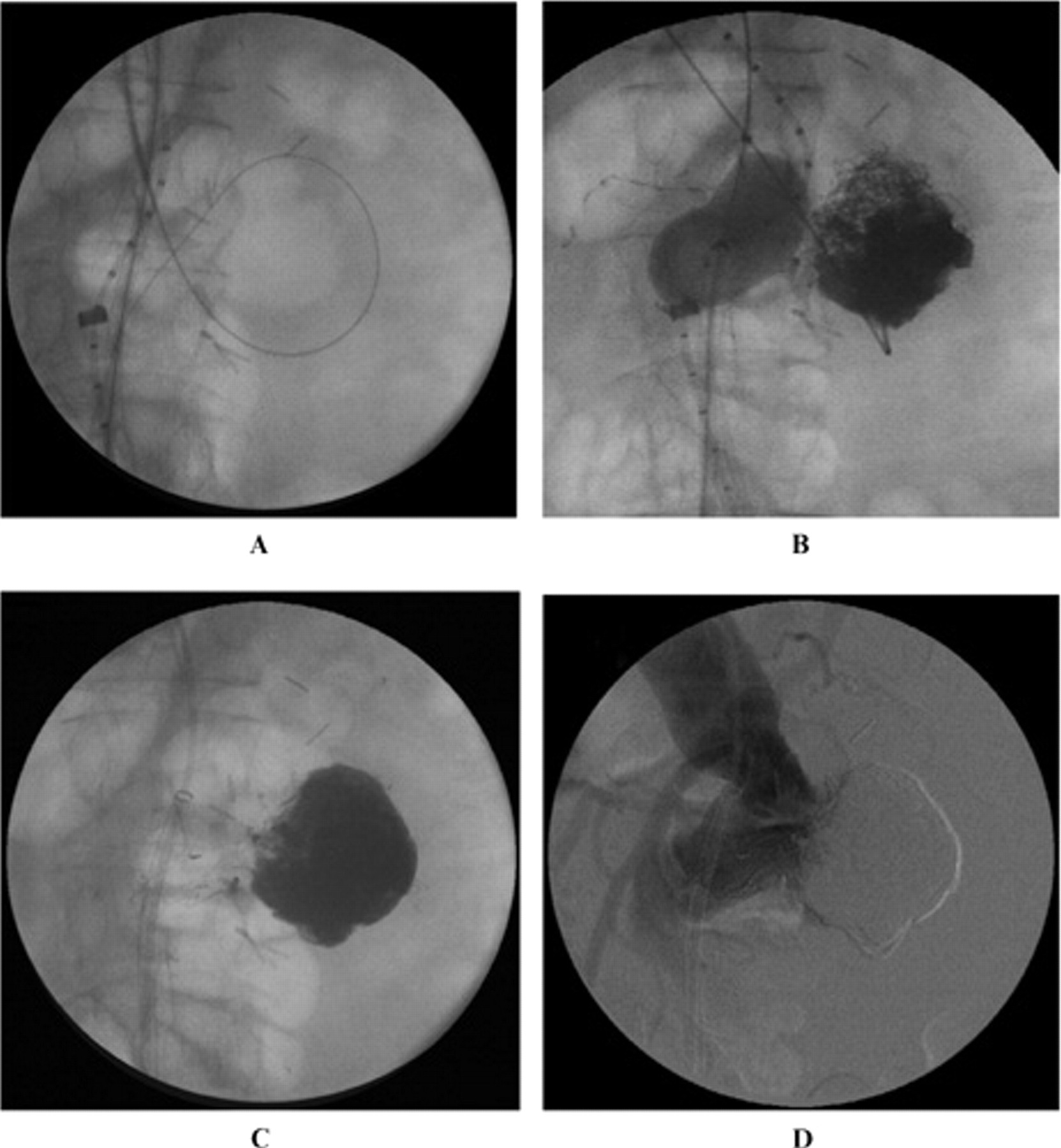
Brachial guidewire directed into the pseudoaneurysm (A). Balloon inflated to cover the neck of the pseudoaneurysm (B). Fluoroscopy showed a pseudoaneurysm completely filled with Onyx (C) and completion angiography without endoleak (D).
Peroperative completion angiography revealed no extravasation of contrast and preserved circulation to the right renal artery (Figure 2D). Postoperative CT angiography showed a decrease in the retroperitoneal hematoma. However, it was not possible to assess extravasation because of the artifacts from the tantalum powder, added to the Onyx.
Postoperatively, the patient suffered a subendocardial infarction and a minor stroke. Approximately 4 weeks later, the patient underwent a secondary intervention with a Zenith Fenestrated AAA Endovascular Graft (William COOK Europe, Bjaereskov, Denmark) with one fenestration to the right renal artery. Completion angiography showed no endoleak. At clinical follow-up, 17 months after the primary intervention, the patient still had a sequel after the stroke and used a wheelchair. She lives at home and is mentally in good shape. CT angiography at 17 months documented an unchanged aneurysm diameter.
Case 2
In 2001, a 46-year-old male had a type A aortic dissection. He had an emergency open repair with an ascending aortic graft. The operation was complicated with postoperative bleeding and reoperation. Postoperatively, he suffered a transitory renal dysfunction and a stroke with a left hemiparesis. He was hospitalized for 1 year. He achieved an acceptable mobility after neurorehabilitation. At follow-up, a type B dissection was revealed, and over time, the patient developed a thoracoabdominal aortic aneurysm. When maximum aneurysm diameter had reached 74 mm, the patient was scheduled for an open repair of the thoracoabdominal aorta at another hospital. Before the scheduled operation had taken place, the aneurysm ruptured in October 2007. The patient was in circulatory shock when he arrived at the referral hospital with a minimum systolic blood pressure of 50 mm Hg. Acute CT angiography showed a rupture at the iliac bifurcation with a right retroperitoneal hematoma (Figure 3). He was transported by helicopter to our hospital and had a systolic blood pressure of 65 mm Hg on arrival. He was transferred directly to the operating/endovascular theater for endovascular repair. Open repair was not considered an option.

Axial computed tomographic angiogram with contrast in the true and the false lumen and the right retroperitoneal hematoma.
A Cook Zenith aortouni-iliac (AUI) stent graft (William COOK Europe, Bjaereskov, Denmark) was inserted through a right percutaneous femoral access into the true lumen and deployed with the proximal edge of the fabrics just below the renal arteries. By percutaneous femoral approach from the left side, a catheter was placed into the false lumen with the tip at the suspected level of the rupture. The false lumen was filled with 8.8 mL of Onyx (Figure 4A). A retrograde angiography from the left iliac artery showed no persistent flow into the false lumen (Figure 4B). Completion angiography with the catheter placed at the top of the stent graft showed contrast in both of the renal arteries and the stent graft. No contrast was seen in the false infrarenal lumen (Figure 4C). As the patient had an AUI stent graft in the true lumen and the false lumen was embolized in the contralateral iliac artery, a femorofemoral bypass was performed with an 8 mm ring-supported Gore-Tex Vascular Graft (W. L. Gore & Associates Inc., Flagstaff, AZ).

Fluoroscopy after completed Onyx injection (A and B) and completion angiography (C).
Postoperatively, the patient developed symptoms of moderate abdominal compartment syndrome with a maximum pressure of 26 mm Hg. The patient was not decompressed because we feared a bleeding complication. He was reintubated because of an acute respiratory failure and aspirated to the lungs during that procedure. Treatment for sepsis was initiated. He also experienced acute renal failure, and continuous venovenous hemodialysis was initiated. A heparin-induced thrombocytopenia was also diagnosed. There was also a need for a pacemaker implantation owing to a sick sinus syndrome. After about 2 months of intensive care unit (ICU) care, the patient was transferred to a surgical ward. The patient was also neurorehabilitated after having suffered a stroke with a minor hemiparesis. His kidney failure was resolved. Seven months after the acute operation, he was ready for ambulant rehabilitation and discharged to his home. CT angiography at 6 months showed an increased diameter of the thoracic portion of the aorta with blood flow in both the true and false lumen. The distal abdominal aorta, where the rupture had been embolized, showed no increase in the aneurysm diameter.
In August 2008, another operation was performed in two steps. A left carotid-subclavian bypass was performed in the first stage followed by a second step, 6 days later, with endovascular debranching of the entire aortic arch. Through a sternotomy, a straight 14 mm Gore-Tex Vascular Graft was anastomosed to the ascending graft. The other end of the graft was surgically anastomosed to the brachiocephalic artery. An 8 mm GORE-TEX sidebranch was connected to the left carotid artery with a bridging 8 mm Viabahn endoprosthesis (W. L. Gore & Associates Inc.) according to the Viabahn Open Revascularization Technique (VORTEC). 15 Subsequently, a one-stage operation using three thoracic GORE TAG thoracic endoprostheses (W. L. Gore & Associates Inc.) was performed with deployment from the ascending graft to the distal portion of the descending aorta. A length of 12 cm of the thoracoabdominal aorta was left uncovered.
Five days with ICU care was necessary, and 10 days after the operation, the patient was transferred to his home hospital. Two weeks after the operation, he was discharged to his home after an uncomplicated postoperative course.
An additional operation was planned with a hybrid technique, covering the last portion of the aorta with a stent graft and debranching of the visceral arteries and the right renal artery. The left kidney was atrophied after the acute operation in 2008 and was not planned for bypass. However, computed tomographic follow-up did not reveal any further increase in aneurysm diameter and transesophageal ultrasonography showed no blood flow in the false lumen. The operation was postponed, and in April 2009, 18 months after the rupture, the patient was enrolled in a surveillance program.
Discussion
Endovascular treatment of standard rAAAs offers a potential benefit for survival. Occasionally, standard stent grafts are not usable in emergency aortic bleeding, and custom-made stent grafts are not practical as a replacement. Internal sealing with the embolic agent Onyx-the plugging and sealing technique-addresses such limitations by offering a solution where the patient is “bridged” from an unstable condition to a controlled situation giving the clinician time for decision making and planning of his next move. Our early experiences indicate that considerable time can be gained. Our first patient had the completion procedure after 4 weeks and the second patient after 10 months.
Onyx embolization was originally used as a definitive treatment of cerebral aneurysms. 16 It has also been a treatment modality for peripheral congenital vascular malformations 13 and visceral aneurysms. 14 This work shows that the plugging and sealing technique using a polymer such as Onyx can work even in the treatment of huge pseudoaneurysms that have ruptured.
Another option is to use coils to fill aneurysms. 17 Onyx has the advantage that it can be applied in any volume required, even in huge aneurysms, where total filling of the aneurysm with coils is a practical impossibility. Onyx has the ability to transform from a liquid to a solid state. That makes it more versatile in its application than coil embolization.
A disadvantage is the interference with postoperative imaging. The artifacts from Onyx in CT angiography make it hard to diagnose an endoleak. Another major drawback is the excessive cost of the product.
One cannot conclude from these early experiences that this treatment modality will function as a definitive treatment. Further studies are necessary. Another question that needs to be addressed is whether the combination of stent grafts and polymer embolization will decrease the presence of endoleaks.
Conclusions
We have described early experiences of successful treatment of acute aortic bleeding by using liquid embolization with Onyx delivered through a 4F catheter using the plugging and sealing technique. The internal sealing has stabilized a ruptured pseudoaneurysm and in another patient stopped the bleeding from a dissected aorta. The method has in these cases been used to bridge the patient over to a definitive treatment under controlled circumstances. This technique may be useful in emergency situations where standard procedures are not an option. However, this technique is under development and further experiences are required.
Footnotes
Acknowledgments
We thank Håkan Geijer, radiologist at Örebro University Hospital, for his help in gathering relevant figures and his general input.
Financial disclosure of authors and reviewers: None reported.