
Abstract
Bovine pericardium was compared to great saphenous vein patch angioplasty regarding the neurologic events after carotid endarterectomy (CEA) with or without concomitant cardiac surgery (CS). From January 1996 to December 2007, 599 patients undergoing CEA (259 with concomitant CS) were enrolled; 456 patients were treated with the great saphenous vein (GSV group) and 143 were treated with bovine pericardium (BP group). Neurologic outcome and Rankin score (RS) were recorded after 24 hours and 30 days. We found comparable rates of neurologic complications (transient ischemic attack, stroke) between the two groups. Thirty-day mortality was 4% (17 of 456 patients) in the GSV group and 0% in the BP group (p = .12). None of the patients died as a consequence of a fatal stroke. Preoperative RS was a prognostic factor for postoperative neurologic deterioration (p = .001). Early neurologic outcome was comparable for the two types of patch material. Preoperative RS predicted postoperative neurologic deterioration.
Carotid endarterectomy (CEA) has a proven benefit in preventing future cerebral infarction in symptomatic and asymptomatic patients with internal carotid artery (ICA) stenosis. 1 The practice of CEA with patch angioplasty has been demonstrated to be more durable compared to primary closure. 2 There is, however, considerable debate over the choice of patch material. 2,3 Some authors favor vein patches, usually the great saphenous vein (GSV), on the basis that autologous, endothelium-lined material may be better at preventing stroke or death and restenosis. 2,4,5 Synthetic materials, such as Dacron or polytetrafluoroethylene (PTFE), are favored by others on the basis of a presumed lower risk of patch rupture and aneurysmal dilatation. 2,3,6 Bovine pericardium (BP) has been introduced in the last decade with encouraging results regarding the small number of early adverse events and low restenosis rate, but the overall number of cases presented in the current literature is still limited. 2,7,8 The aim of the present study was to compare the GSV with BP with regard to early neurologic events following CEA with or without concomitant cardiac surgery (CS).
Patients and Methods
A retrospective review of our prospectively maintained CEA database from January 1996 to December 2007 yielded 599 patients who had received a CEA. The GSV was preferred as patch material in 456 of 599 procedures (GSV group, 76%) and BP in 143 of 599 procedures (BP group, 24%). Thirteen of 599 (11 with GSV and 2 with BP) were redo procedures. Patient demographics, comorbidities, and characteristics are listed in Table 1.
Preoperative Patients' Demographics and Characteristics
BP = bovine pericardium; GSV = great saphenous vein; ICA = internal carotid artery; IDDM = insulin-dependent diabetes; NIDDM = non–insulin-dependent diabetes; TIA = transient ischemic attack.
Operation Techniques
Carotid Endarterectomy
All CEAs were performed under general anesthesia with routine use of a 10F or 12F shunt. The arteriotomy was routinely performed proximally to the carotid bulb and extended laterally into the ICA. This incision was lengthened distally across the diseased ICA until there was visualization of an undisturbed intimal surface. Only at this stage was the shunt inserted. The technique of endarterectomy included sharp, bevelled plaque transection at the level of the distal common carotid artery, eversion endarterectomy at the level of the external carotid artery, and neat feathering of the atherosclerotic disease away from the mid-to-distal ICA and its natural break point. Tacking sutures were used if required to secure the distal intimal step, preventing distal intimal dissection. Patients who were treated with a vein patch had a segment of GSV harvested from the lower leg, which was sutured with 6-0 polypropylene. In patients who received BP, 6-0 polypropylene sutures were also used. The vein patch was used at the harvested width, and the BP was a standard 7 mm in width. In isolated CEA, the neck wound was closed in standard fashion. In combined CEA-CS procedures, the neck wound was left open until the heparin had been reversed with protamine following the completion of CS to allow final inspection of the suture line.
Coronary Artery Bypass Grafting
Coronary artery bypass grafting (CABG) was performed through a median sternotomy. The left internal mammary artery was harvested as a pedicle and anastomosed to the left anterior descending artery in all cases. The saphenous vein and radial artery were anastomosed in most cases to the aorta as free grafts. Heparin was given to achieve a target activated clotting time above 400 seconds. Levels of hemoglobin lower than 8.5 g/dL resulted in red blood cell transfusion. Cardiopulmonary bypass was started by cannulation of the ascending aorta and the right atrium. Nonpulsatile flow was used. Rectal temperature was kept between 30 and 34°C. Myocardial protection was achieved by using intermittent antegrade cold blood or crystalloid cardioplegia. On completion of all distal anastomoses, the aortic cross-clamp was removed and the proximal anastomosis was performed under tangential clamping of the ascending aorta. In combined procedures, BP was used either in total arterial revascularizations or if the venous material was insufficient.
The choice of graft, that is, GSV versus BP, was left to the discretion of the surgeon in isolated CEAs. In concomitant CEA-CABG, BP was preferred either in total arterial revascularizations or when vein material was not available.
Definitions
Transient Ischemic Attack
Transient ischemic attack (TIA) was defined as focal cerebral dysfunction of presumed vascular origin that resolved completely within 24 hours.
Stroke
Stroke was defined as focal or global cerebral dysfunction of presumed vascular origin lasting more than 24 hours.
Rankin Score
We used the modified classification of the Rankin scale by Bonita and Beaglehole
9
: 0 points = no symptoms; 1 point
Statistical Methods
All analyses were performed with MedCalc 9.4.2.0 for Windows (Mariankerke, Belgium). Categorical variables and frequencies are presented as percentages and continuous variables are presented as means (range). Comparisons of patient characteristics, as well as comparisons of postoperative outcome (stroke, TIA, mortality), were performed using the chi-square test. For continuous variables, the Smirnov-Kolmogorov test was performed to control their distribution. For normally distributed variables, a t-test for independent variables was preferred. All variables not normally distributed are presented as medians (range) and compared with the Mann-Whitney U test. A logistic regression model was constructed to detect the independent factors contributing to neurologic complication. Comorbidities, gender, patch type, and preoperative RS were included in the regression model. A p value ≤ .05 was considered statistically significant for all tests.
Results
Hospitalization and Mortality
The median postoperative in-hospital stay was 13 (0–26) days for the GSV group and 9 (3–15) days for the BP group (p = .45). The stay in the intensive care unit was 1.8 (0–4.9) days in the GSV group and 0.8 (0–1.6) days in the BP group (p = .91).
Thirty-day mortality was 4% (17 of 456 patients) in the GSV group and 0% in the BP group (p = .12). In all 17 patients from the GSV group, concomitant CS and cardiopulmonary bypass had been performed. The cause of death was heart failure in the majority of patients (n = 16) and sepsis-related multiple organ failure in the remaining patient. None of the patients died as a consequence of a fatal stroke (RS = 6).
Neurologic Complications
In the first 24 hours, the rate of postoperative neurologic deficit was 8% in both groups (Figure 1). In 2.2% (10 of 456) of patients in the GSV group, the diagnosis was that of a transient cranial nerve injury of the hypoglossal or facial nerve, a TIA in 2.2% (10 of 456), and a stroke in 3.3% (15 of 456). In the BP group, 2.6% (4 of 143) of patients had a transient cranial nerve injury, 3.5% (5 of 143) had a TIA, and 2.1% (3 of 143) developed a stroke. There was no statistically significant difference for each complication between the two groups.
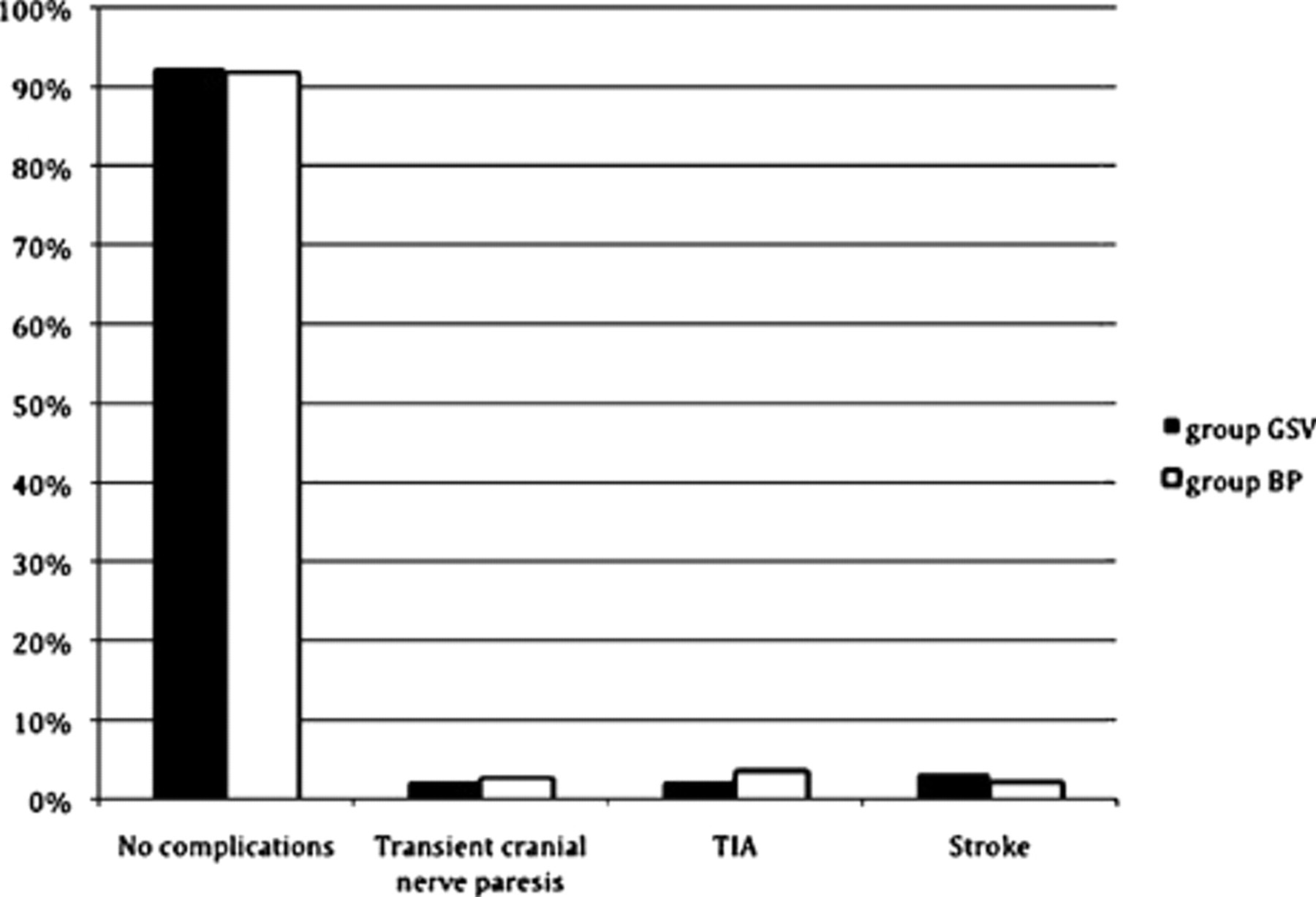
Frequency of postoperative complications during the first 24 hours postoperatively. BP = bovine pericardium; GSV = great saphenous vein; TIA = transient ischemic attack.
Between 24 hours and 30 days postoperatively, 7% of the patients in the GSV group and 4% in the BP group developed neurologic deficits (p = .27; Figure 2). In the GSV group, 1.9% (9 of 456) of patients showed a transient cranial nerve palsy, 1.3% (6 of 456) a TIA, and 3.5% (6 of 456) a stroke. In the BP group, 0.6% (1 of 143) of the patients had a palsy of the hypoglossal or facial nerve, 2% (3 of 143) had a TIA, and 1.4% (2 of 143) developed a stroke (see Figure 2). No significant difference was observed for each separate neurologic complication between the two groups.
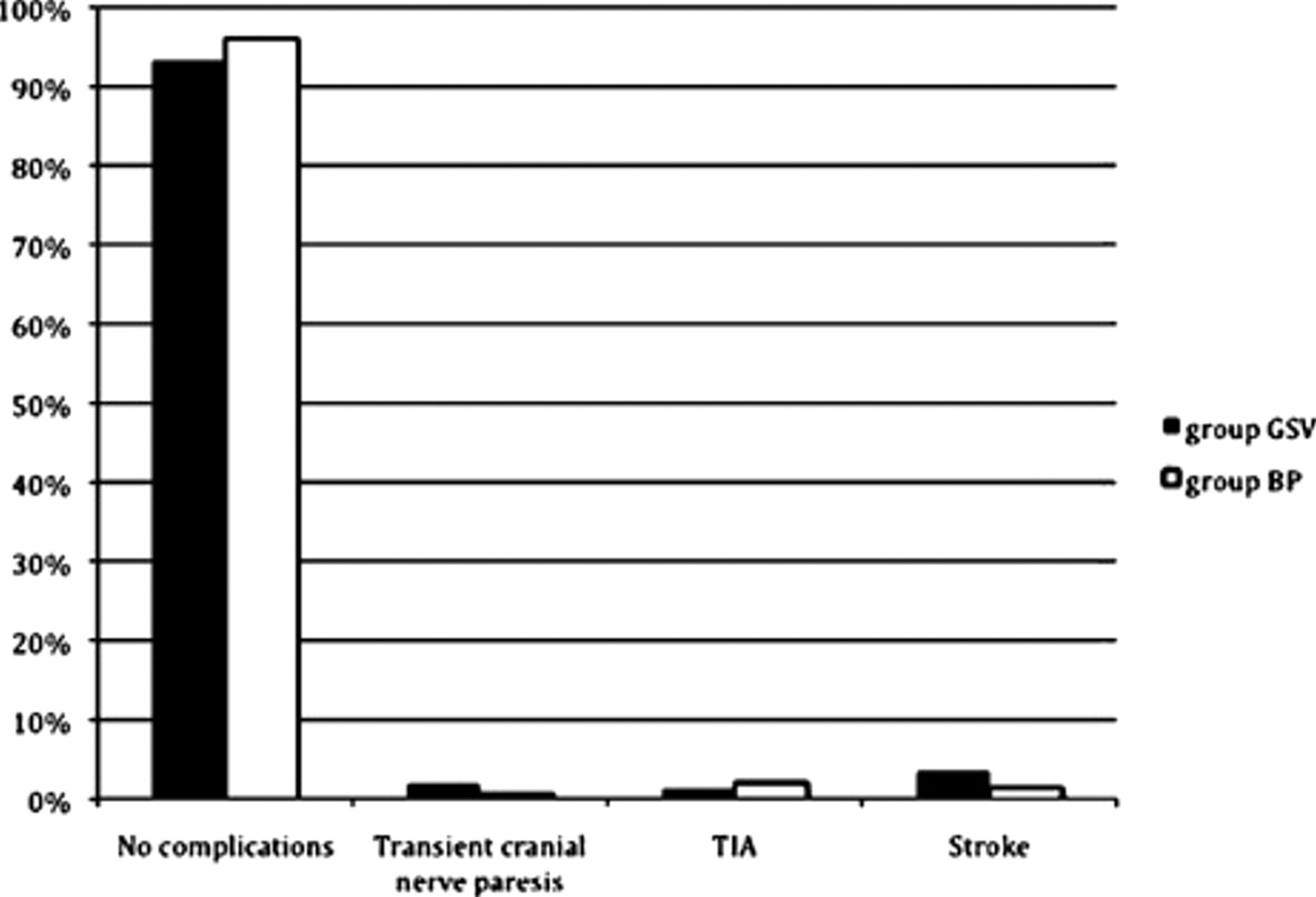
Frequency of neurologic complications between 24 hours and 30 days postoperatively. BP = bovine pericardium; GSV = great saphenous vein; TIA = transient ischemic attack.
Rankin Score
Multiple regression analysis, which included patients' demographics and comorbidities (Table 2), demonstrated the preoperative RS as the only significant positive predictor of postoperative neurologic deterioration in both groups (odds ratio 3.2; 95% CI 2.17–11.32; p = .001). Figure 3 shows the increase in the preoperative RS during the perioperative course in both populations. There was no statistically significant difference between the groups.
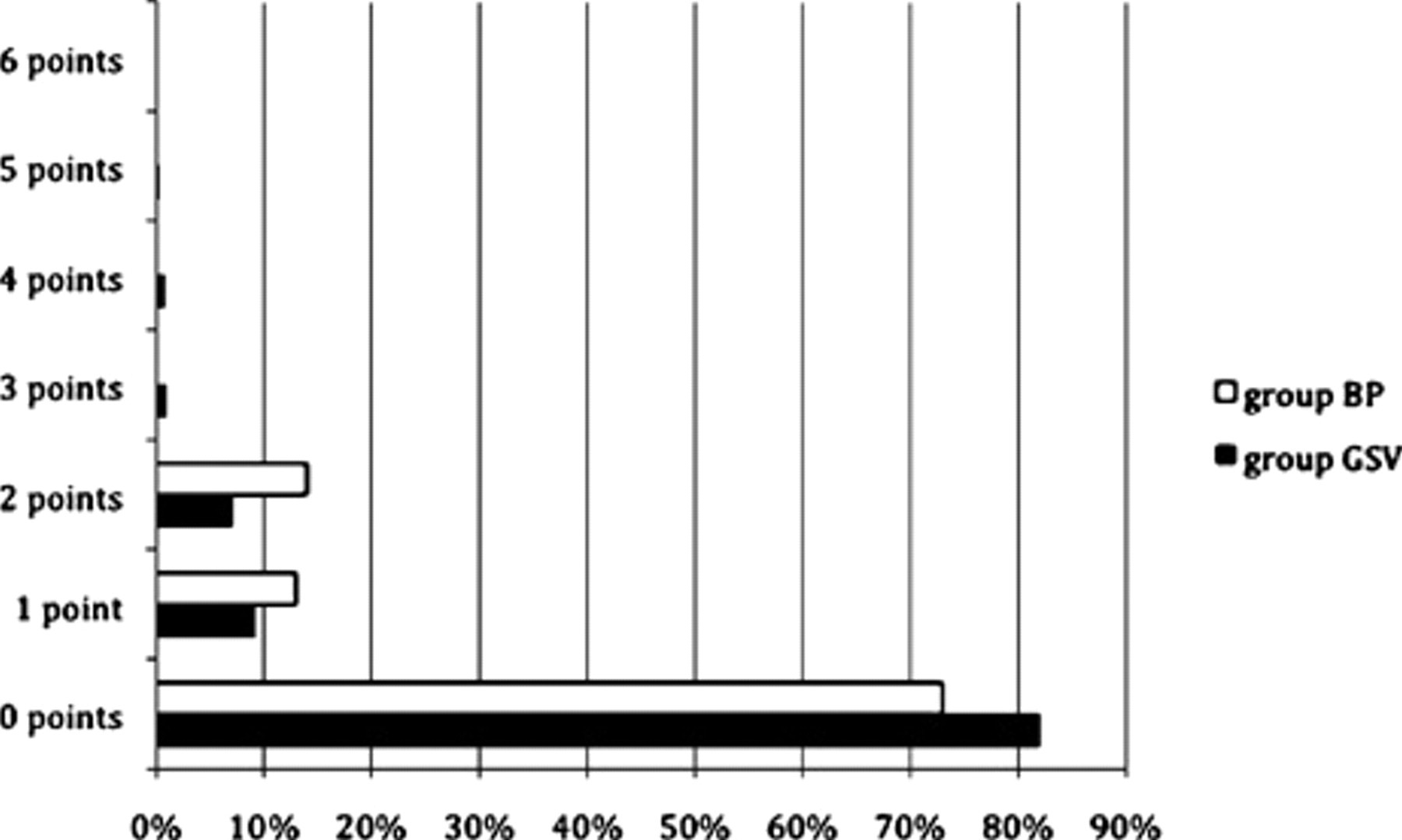
Comparison of the increase in preoperative Rankin score postoperatively. No significant differences were obtained between the cohorts (p > .05). BP = bovine pericardium; GSV = great saphenous vein.
Results of Multiple Logistic Regression Analysis for Positive Predictors for Postoperative Neurologic Complications in Both Groups
Discussion
CEA represents the gold standard for treating severe atherosclerotic carotid artery stenosis. The technique of vascular reconstruction after endarterectomy remains under debate. Bond and colleagues showed a significant and potentially clinically important trend in favor of routine patching versus primary closure in terms of both short- and long-term reduction in risk for ipsilateral stroke, side-independent stroke, and any stroke and death. 2 The selection of the patch material also remains controversial, with supporters for both autogenous tissue (vein) and synthetic patches (PTFE, Dacron). 2,3,6 However, a number of new materials, such as BP and thin-walled Fluoropassiv (a new polyester carotid patch), have been introduced but remain to be evaluated on a large scale. 2,3,7,10
Several randomized trials have shown that synthetic patches are “safer” than venous patches in terms of either neurologic events or patch rupture and aneurysmal dilatation. 3,6,11,12 However, in a systematic review of 1,200 randomized patients, Bond and colleagues were unable to find any statistically significant differences in the risk for stroke or death dependent on patch material (synthetic [PTFE or Dacron] or vein patches)-either perioperatively or during the long-term follow-up-or evidence to support the belief that synthetic patches are associated with a lower risk for patch rupture. 2 Hayes and colleagues addressed the hypothesis that prosthetic patches are as safe as vein patches with regard to their thrombogenicity with positive results. 13 Verhoeven and colleagues obtained an increased number of microemboli and a higher rate of restenosis related to Dacron patches compared to venous patch or primary closure in 319 patients. 5 Meerwaldt and colleagues, comparing Fluoropassiv with a venous patch, found no enhanced thrombogenicity and no higher rate of postoperative bleeding. 3
Several groups have previously reported experience with the BP carotid patch. 10,14–16 Hines and colleagues determined the incidence of restenosis in 61 patients who underwent CEA with BP with encouraging results, without, however, any comparison with other types of patch materials. 10 In 148 CEAs, Matsagas and colleagues showed early and midterm results, again without any control group, proposing BP as a suitable patch material for routine use in carotid surgery. 14 In this study, there were no late neurologic events and no late reoperations. In another work, no significant difference was observed in postoperative major events (stroke or death) between 323 procedures with BP and 194 procedures with primary closure. 15 However, Neuhauser and Oldenburg compared in 125 patients the short-term results between polyester and BP patching, suggesting that BP patching during CEA may have a lower restenosis rate. 16 In this report, there were no ipsilateral TIAs or strokes and the 30-day mortality was 0.8% in both groups.
We report our experience with BP in carotid patch angioplasty comparing the outcome to that of venous patching. Thirty-day mortality was 4% in the GSV group and 0% in the BP group, in concordance with other studies. 2,10,14 Biasi and colleagues presented 1.5% 30-day mortality in the BP group. 15 The higher mortality rates in our GSV group may be explained by the higher incidence of concomitant CS, especially as the majority of deaths (16 of 17) were cardiac related and no fatal strokes were reported.
The postoperative in-hospital stay was not statistically different between the two groups (p = .45). For the BP group, the stay was longer compared to that for the other groups, possibly owing to the concomitant CS. 14
The rate of early (< 24 hours) neurologic complications (see Figure 1 and Figure 2) was 8% in both groups, without any significant difference between the two methods of patching for the risk of an early stroke. Late neurologic deficits developed in 7% of patients in the GSV cohort and 4% in the BP group. This was also without statistical significance (p = .27). These results confirm equal effectiveness of the two types of patch material regarding the rates of postoperative stroke. The percentages for the GSV group are comparable to those in other reports 3 or even lower. 2,12 The rate of neurologic complications in the BP group in the first 30 days (4%) was comparable to that of other groups. 10,14,16 Matsagas and colleagues reported 6.1% neurologic complications during the postoperative course of their patients (n = 138). 14 Hines and colleagues and Neuhauser and Oldenburg achieved no neurologic complications in 61 and 59 patients, respectively. 10,16 Biasi and colleagues showed lower rates of postoperative complications (3.6%) after 323 procedures. 15
Among other variables in the attempt to identify predictors for neurologic outcome we have also determined the pre- and postoperative RS using the modified version of the Rankin scale of Bonita and Beaglehole. 9 The preoperative RS proved to be the only significant positive predictor for postoperative neurologic deterioration in both groups (p = .001). The postoperative increase in RS was, however, statistically not significantly different between the two groups (p = .16), which further supports equality in neurologic outcome for the two types of patch material.
The limitations of our study are the absence of long-term results regarding restenosis and stroke rates and the retrospective nature of the work. Thus, we focused primarily on the 30-day procedural risk for stroke and death, leaving the equally important issues of restenosis and stroke freedom to be addressed.
Conclusions
The study confirms the absence of any significant difference between the GSV and the BP patch following CEA regarding short-term (< 24 hours) or midterm (30 days) postoperative neurologic complications and increase in RS. The preoperative RS positively predicts postoperative neurologic deterioration.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.
Presented at the Annual Meeting of the German Society for Thoracic and Cardiovascular Surgery, February 15–18, 2009, Stuttgart, Germany.