
Abstract
Background:
Mycosis fungoides (MF) is the most common clinicopathologic subtype of primary cutaneous T-cell lymphoma.
Objective:
The therapy of MF is highlighted in this overview.
Results and Conclusions:
Skin-directed MF therapies include topical corticosteroids, nitrogen mustard, carmustine (BCNU), topical bexarotene gel, imiquimod cream, radiotherapy, total skin electron beam therapy, and phototherapy. Systemic therapies include extracorporeal photopheresis, interferon, oral bexarotene, denileukin diftitox, monoclonal antibodies and cytokine therapy, and other systemic chemotherapy. Finally, some investigative therapeutic modalities are presented.
PRIMARY CUTANEOUS LYMPHOMAS are a group of T- and B-cell neoplastic conditions that, although having the potential for systemic involvement, manifest primarily in the skin. Classification of cutaneous lymphomas is complex; auspiciously, the combined World Health Organization and European Organisation for Research and Treatment of Cancer classification system of cutaneous lymphomas was recently published. 1 Mycosis fungoides (MF) is the most common clinicopathologic subtype of primary cutaneous T-cell lymphoma. The term mycosis fungoides came into use in 1806 by Jean-Louis Marc Alibert, a French dermatologist, when he described a severe disorder in which large necrotic tumors resembling mushrooms presented on a patient's skin. However, the designation is a misnomer since no association with a fungus exists. 2
The choice of the best treatment modality largely depends on the clinical staging of MF, which is depicted in Table 1. 3 The concept of “stage-directed therapy” guides therapeutic choices, and the management modalities can be divided into (1) skin-directed therapies, which are primarily effective in early disease, and (2) systemic therapies, used in advanced cases. These are summarized in Table 2. The effectiveness of skin-directed therapy stems from the fact that neoplastic skin-homing T cells localize primarily to epidermis and superficial dermis, whereas biologic response modifiers serve to potentiate the host's immune response to neoplastic T cells. Importantly, the combination therapy often works best. Besides the clinical stage, other factors need to be taken into consideration in guiding treatment: the patient's age and general health, availability of treatment modalities, cost, and physician's expertise. Depending on the stage of the disease, the management of MF can take place in dermatologists' private offices or, as with more extensive tumor burden, in tertiary referral centers. Many patients with extensive skin involvement (ie, plaques, tumors, or erythroderma) frequently require a combination of topical and well-tolerated systemic therapy to attain a long-term response. The objective of this review is to highlight therapeutic modalities of MF, with the focus on evidence from the reported studies. The management of other forms of cutaneous T-cell lymphoma is not discussed here.
Clinical Staging of Mycosis Fungoides

Adapted from Girardi M et al. 3
Overview of Mycosis Fungoides Therapies
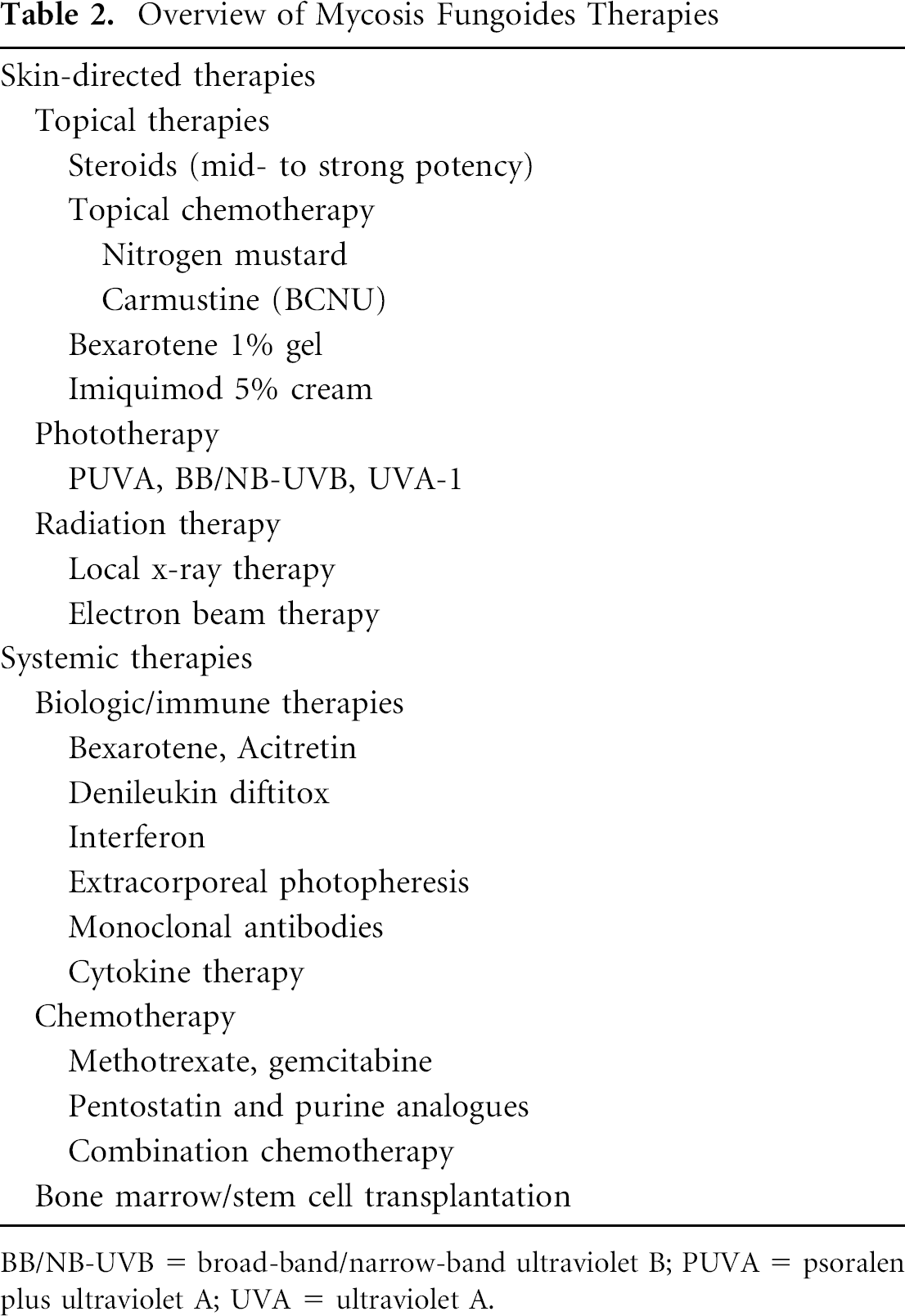
BB/NB-UVB = broad-band/narrow-band ultraviolet B; PUVA = psoralen plus ultraviolet A; UVA = ultraviolet A.
Skin-Directed Therapies
Topical Corticosteroids
Topical corticosteroids, particularly high-potency (class I) compounds, are often used as the first-line therapy for patch-stage MF. 4 Zackheim and colleagues reviewed the effectiveness of topical steroids in MF in a series of 79 patients, with a median follow-up period of 9 months. 5 Thirty-two (63%) stage T1 patients achieved complete remission and 16 (31%) achieved partial remission, for a total response rate of 48 (94%). The comparable figures for stage T2 patients were 7 (25%), 16 (57%), and 23 (82%), respectively. Parenthetically, these response rates are similar overall to those achieved with other forms of skin-directed therapies. In more advanced stages of MF, topical steroids hold a role as adjuvant therapy, and intralesional corticosteroids can also be used for thicker MF lesions.
Nitrogen Mustard
Nitrogen mustard (NM) is a deoxyribonucleic acid (DNA) alkylating agent used in the therapy of primarily patch- and plaque-stage MF. 6 Topical NM can be used in an aqueous (10–20 mg/dL) or ointment-based preparation. A small amount of NM is first applied by the patient to a selected test area once daily for 7 to 10 days; if well tolerated, the treatment is continued with once- or twice-daily application to all lesions. In a series of 203 patients with clinical stage I–III MF treated with topical NM as initial therapy, the overall response rate was 83%, with a complete response rate of 50%. 7 The median time to achieve a complete response was 12 months, and the median time to relapse was 12 months. Overall and complete response rates of 93% and 65% were observed in stage T1 disease and of 72% and 34% in stage T2 disease, respectively. Freedom from progression rates in T1 disease at 5 and 10 years were 92% and 85%, respectively, and in T2 disease, 83% at 5 and 10 years. A large proportion of patients treated with aqueous NM can develop contact hypersensitivity reactions; however, in the above-mentioned series, fewer than 10% of patients experienced this complication when NM ointment was used. Other side effects of NM include localized bullous and urticarial reactions, hyperpigmentation, and an increased risk of development of squamous and basal cell carcinomas. 8 NM is contraindicated in pregnancy.
Carmustine
Topical carmustine (BCNU) is another alkylating agent that is effective for patch- and early plaque-stage MF. The University of California, San Francisco, experience with topical BCNU in the treatment of approximately 200 patients with MF was recently published. 9 BCNU is available in solution or ointment form, which can be used daily or on alternate days. Similar efficacy to NM has been reported, with a complete response rate of around 86% in T1 disease. The main side effects include development of telangiectasias and irritation, which are not a major deterrent to continuation of therapy. Less hypersensitivity than with NM therapy is observed. Myelosuppression may occasionally develop; hence, the complete blood count should be monitored every 2 weeks. A course of therapy usually lasts 2 to 6 months.
Topical Bexarotene Gel
Topical bexarotene 1% gel has been approved by the US Food and Drug Administration (FDA) for the treatment of early-stage MF. 10 It can be used in patients resistant or intolerant to other topical therapies, usually with less than 15% body surface area involvement. Bexarotene is a retinoid that binds to retinoid X receptors (RXRs), inducing apoptosis of abnormal T cells. Oral bexarotene is also available for the treatment of MF and is reviewed below. Nightly application of topical bexarotene for 1 week is followed by twice-daily application, with, overall, 12 to 16 weeks of therapy recommended. Side effects include local irritation in up to 70% of patients and pruritus. Irritant response can be reduced by decreasing the frequency of application. Clinical complete response rates of 25 to 28% are observed. 11 The estimated median response duration from the start of therapy was 99 weeks. Both topical and systemic bexarotene belong to pregnancy category X, and the use of topical bexarotene together with diethyltoluamide (DEET) insect repellent is not recommended as the toxicity of the former may be increased.
Imiquimod
Given that systemic interferon is an established form of biologic therapy in MF, topical imiquimod cream may hold promise in the treatment of individual lesions. A recent open-label pilot study reported six patients with stage IA to IIB MF who were treated with topical imiquimod 5% cream three times per week for 12 weeks. 12 Three of six patients had histologic clearance of disease, and a fourth patient had two of four lesions respond clinically. Further studies are needed to assess the efficacy of this modality.
Radiotherapy
Radiotherapy is an easily available and practical modality of therapy in MF as the disease is highly radiosensitive. There are well-defined dose-response relationships for achieving a complete and durable response. 13 Radiotherapy is often used alone for single tumors in patients with plaque-stage disease or in combination with other modalities (ie, psoralen plus ultraviolet A [PUVA]). A complete response rate of 98% is observed for plaques and 36% for tumors. Thick plaques and eroded tumors can be treated with low-dose superficial radiotherapy in several fractions. Relapse usually occurs within 5 years.
Total Skin Electron Beam Therapy
Total skin electron beam (TSEB) radiation has been in use for several decades in the treatment of virtually all stages of MF, and a consensus statement on methods and clinical indications for TSEB radiation in the treatment of MF was recently published. 14 The patient stands 7 m from a linear accelerator that delivers 4 to 6 MeV of energy per session. The total dose of radiation is important: over 30 Gy (3,000 rad) is needed to achieve a complete response, with fractions of 1.5 to 2 Gy for 8 to 10 weeks given. In a series of 60 patients with MF, the overall response rate was 96.6%, with a complete response in 50 of 60 patients (83.3%) and a partial response in 8 cases (13.3%). 15 Responses are stage dependent. Recently, Ysebaert and colleagues reported their experience in the treatment of 57 patients with T1 and T2 MF with TSEB radiation. 16 Three months after completion of TSEB radiation, the overall response rate was 94.7%. The 5-, 10-, and 15-year overall survival rates were 90%, 65%, and 42%, respectively. TSEB radiation can be given as adjuvant therapy, initiated after complete remission, in conjunction with topical NM or PUVA for at least 6 months. The side effects of TSEB radiation are usually mild and include reversible alopecia, erythema, desquamation, xerosis, onychomadesis, and anhidrosis lasting for 6 to 12 months after treatment. The combination of radiation therapy and PUVA is highly carcinogenic.
Phototherapy
Phototherapy for cutaneous T-cell lymphoma was reviewed by Baron and Stevens. 17 PUVA is one of the most effective therapies for early disease and is often used as standard first-line therapy. Therapy is usually given two to three times per week until clearance or best partial response. A complete response rate of up to 80 to 90% can be observed in patients with T1 or T2 stage disease, although the tumors are less responsive. In a recent retrospective cohort analysis of stage IA to IIA MF patients treated with PUVA monotherapy, 30 to 50% remained disease free for 10 years, but late relapses did occur. 18 Some centers use maintenance PUVA (treatment every 2 to 4 weeks) to prolong remission. Broad-band and narrow-band ultraviolet B have also been used, which are safer than PUVA but not as effective, especially for plaques and tumors. In patients with patch-stage MF, a complete response rate of up to 75% can be observed. 19 Furthermore, a monochromatic excimer laser (308 nm) has been used in the treatment of early-stage MF. 20
Systemic Therapies
Extracorporeal Photopheresis
Extracorporeal photopheresis (ECP) involves reinfusion of PUVA photoirradiated blood, stimulating a CD8+ cell-mediated immune response against mutated CD4+ T-cell clones. The therapy takes place 2 consecutive days per month (3 hours' duration) for 4 to 6 months. ECP is considered first-line therapy for Sézary syndrome, the leukemic form of MF. The combined overall response rate to ECP for all stages of cutaneous T-cell lymphoma is 55.7%, with 17.6% achieving a complete response. 21 A clinical response is usually seen in the first 6 to 8 months of treatment. ECP given concurrently with or immediately after TSEB radiation (32–40 Gy) has also been shown to significantly improve progression-free and cause-specific survival in MF compared with TSEB radiation alone. 22 Photopheresis therapy was recently reviewed in the Journal of Cutaneous Medicine and Surgery. 23
Interferon
Interferon (IFN)-α2a is a well-established biologic therapy in MF and can be administered in interleukin (IL), subcutaneous, or intramuscular forms. Subcutaneous IFN-α2a is given three times a week or daily for 6 to 9 months. Fifty percent partial response and 17% complete response rates are observed. Combination therapy with PUVA or photopheresis is often used as well. In a series of 39 patients with MF and Sézary syndrome treated with combined phototherapy and systemic IFN-α2a, 36 patients achieved a complete response (62%) or a partial response (28%) to therapy. The median response duration was 28 months. 24 The side effects of IFN include flu-like symptoms, depression, cytopenia, and increased hepatic enzymes. Quality of life questionnaires are an important utility during IFN therapy.
Oral Bexarotene (Targretin)
Bexarotene is a synthetic retinoid that selectively binds to RXRs, inducing apoptosis of malignant T cells. It can be used in all stages of refractory cutaneous T-cell lymphoma and is administered at a dose of 300 mg/m2/d for a course of 3 to 5 months. As a single oral agent, the efficacy of oral bexarotene is roughly similar to that of IFN-α2a. Response rates of 54% for stage IA and IIA and of 45% for stage IIB-IVB are observed. Oral bexarotene is excellent in combination therapy, for instance, with PUVA (ie, Re-PUVA), as lower PUVA cumulative dose and fewer treatments are required. 25 In a retrospective chart review analysis by Singh and Lebwohl, eight patients with MF stage Ia to IIb who failed multiple single-agent treatment regimens were treated with low-dose oral bexarotene and PUVA combination therapy. 26 An initial response in all patients and complete remission in five of the patients treated were observed, with pruritus being the most common adverse event. 26 The side effects of oral bexarotene include hypercholesterolemia (60% of patients), hyperlipidemia (70%), hypothyroidism (60%), and leukopenia (18%), necessitating close blood monitoring. Hyperlipidemia occurs primarily within 2 to 4 weeks of therapy and can be associated with serious but reversible pancreatitis. The use of lipid-lowering agents is recommended in conjunction with bexarotene therapy.
Denileukin Diftitox
Denileukin diftitox (Ontak) is a recombinant fusion protein of diphtheria toxin and IL-2. It binds avidly to IL-2 receptors expressed on tumor cells, inhibiting tumor-cell protein synthesis and leading to tumor cell lysis. Denileukin diftitox was FDA approved for the treatment of resistant or recurrent cutaneous T-cell lymphoma. 27 Daily infusions of 18 μg/kg/d for 5 days are given, with the cycle repeated every 3 weeks. A response is usually observed after two to six cycles. The results of a pivotal phase III trial of two dose levels of denileukin diftitox for the treatment of cutaneous T-cell lymphoma were reported in 2001. 28 An overall response rate of 30% and a complete response rate of 10% were observed, with a median duration of response of 6.9 months. The side effects include constitutional symptoms, hypersensitivity reactions, myelosuppression, and vascular leak syndrome, which occurred within 14 days in 25% of patients. The latter is characterized by hypotension, hypoalbuminemia, and peripheral edema and is treated with systemic corticosteroids.
Monoclonal Antibodies and Cytokine Therapy
Host immune response plays an exceedingly important role in effecting the progression of MF, and a number of monoclonal antibodies and cytokines have been used in the management of the disease, recently reviewed by Rook and colleagues. 29 Campath-H1 (alemtuzumab) is an anti-CD52 antibody used mostly in advanced MF. In a series of 22 patients with predominantly stage III or IV disease treated with alemtuzumab, the overall response rate was 55%, with 32% of patients achieving complete remission and 23% partial remission. 30 The median time to treatment failure was 12 months. Chimeric anti-CD4 monoclonal antibody (HuMax) has also been used. 31
Systemic Chemotherapy
Systemic chemotherapy is given to patients with lymph node or visceral involvement or for progressive skin tumors not controlled with skin-directed treatment. 32 The major challenge is that malignant T cells are similar to other mature T cells in sensitivity to cytotoxic agents. The initial regimen of chlorambucil 4 mg and prednisone 40 mg daily is often used, with subsequent augmentation of chlorambucil dose and taper of prednisone. Methotrexate was approved by the FDA for the treatment of advanced MF. 33 The weekly dosage of 20 to 60 mg is used for 2 to 4 months. CHOP (cyclophosphamide, doxorubicin, Oncovin [vincristine], prednisone) chemotherapy results in 80 to 90% partial response rates, but relapses are common. Other forms of chemotherapy used in the treatment of MF include combination regimens, as well as the monotherapy agents bleomycin, doxorubicin, etoposide, and fludarabine. Gemcitabine (Gemzar) is a pyrimidine antimetabolite that has been used in the treatment of MF refractory to other therapies. In a series of 44 such patients, overall, 70% responded to treatment and 10% achieved a complete response. The median durations of complete response and partial response were 15 months and 10 months, respectively. Treatment was well tolerated, with only mild hematologic toxicity and no nausea or vomiting or organ toxicity recorded. 34
Therapies under Investigation
Bone marrow and stem cell transplantation may represent potentially successful treatment modalities for patients resistant to currently available modalities, although further studies are needed. 35 Immunotherapy and vaccination therapy (ie, peptide-loaded dendritic cell vaccines) hold promise in the therapy of MF; however, unlike in melanoma, useful associated antigens remain to be identified. Histone deacetylase inhibitors (ie, suberoylanilide hydroxamic acid) are broad anticancer agents 36 that are under investigation in MF. Also, a National Cancer Institute stage I trial of forodesine (BCX-1777), a tumor growth enzyme blocker, in MF is under way. Given that MF is a T helper 2 condition, it can be theoretically reversed by T helper 1 cytokine induction, which is an avenue for future therapies. For instance, CpG DNA sequences are known to target dendritic cell Toll-9 receptors and to induce a T helper 1 profile. Enhancement of the host immune responses in MF by CpG oligodeoxynucleotides and IL-15 was recently reported by Wysocka and colleagues. 37
Maintenance Therapy
On remission, various modalities can be used as maintenance therapy, including topical NM, topical steroids, extracorporeal photopheresis, and IFN. Some centers use PUVA or ultraviolet B weekly for 1 year, followed by treatment every 2 weeks for 2 years and then monthly for 2 years. It has been hypothesized that malignant cutaneous T cells can recirculate for up to 5 years without producing visible lesions. After remission off treatment for 5 to 8 years, relapse is very rare, and cure is often defined as 8 years without any therapy.
Conclusions
A variety of factors need to be taken into consideration in deciding on therapeutic options in MF. These include the stage of the disease, treatment availability, and the benefits and toxicity of therapy, as well as the patient's wishes. When the disease is confined to the skin, skin-targeted therapies are preferred. Biologic response modifiers and chemotherapy, often in combination with skin-directed therapy, are used for more advanced disease with lymph node or systemic involvement. The therapy for MF is evolving owing to better molecular understanding of the disease. Patients should be considered for clinical trials when these are available.