
Abstract
Etanercept is a new treatment for moderate to severe psoriasis. In contrast to traditional systemic agents, which can be given orally, etanercept is given by subcutaneous injection. Patient selection, transitioning, dosing, safety, monitoring, duration of therapy, and patient support programs are reviewed.
BIOLOGIC AGENTS are a new distinct treatment class for the management of moderate to severe psoriasis. Large, randomized, controlled studies have shown them to be efficacious, with a significant positive impact on quality of life and a good safety and tolerability profile. 1 The currently available products differ from the traditional systemic agents by their method of administration (injection rather than oral) and possibly safety profile. When considering new therapies, it is important for physicians to understand which patients would be ideal candidates, how to transition patients from other therapies, how the products should be administered, the recommended dosing, expected response, potential adverse events, how to monitor patients, and the circumstances under which treatment should be discontinued. This article explores these issues to assist physicians with the initiation and maintenance of etanercept therapy.
Identifying Appropriate Patients
Approved Indications of Etanercept
Etanercept was first approved by Health Canada in December 2000 for patients with rheumatoid arthritis (RA). It has since received approval for juvenile RA (July 2003), psoriatic arthritis (PsA) (January 2004), ankylosing spondylitis (May 2005), and plaque psoriasis (December 2005). In Canada, it is approved for the treatment of adult patients with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. 2 No universally accepted definition of “moderate to severe” psoriasis exists (Table 1).3–8 The Canadian Psoriasis Expert Panel's definition is outlined in Table 2. 1 This definition, although broader than some, recognizes the importance of quality of life.
Classification of Severity of Psoriasis
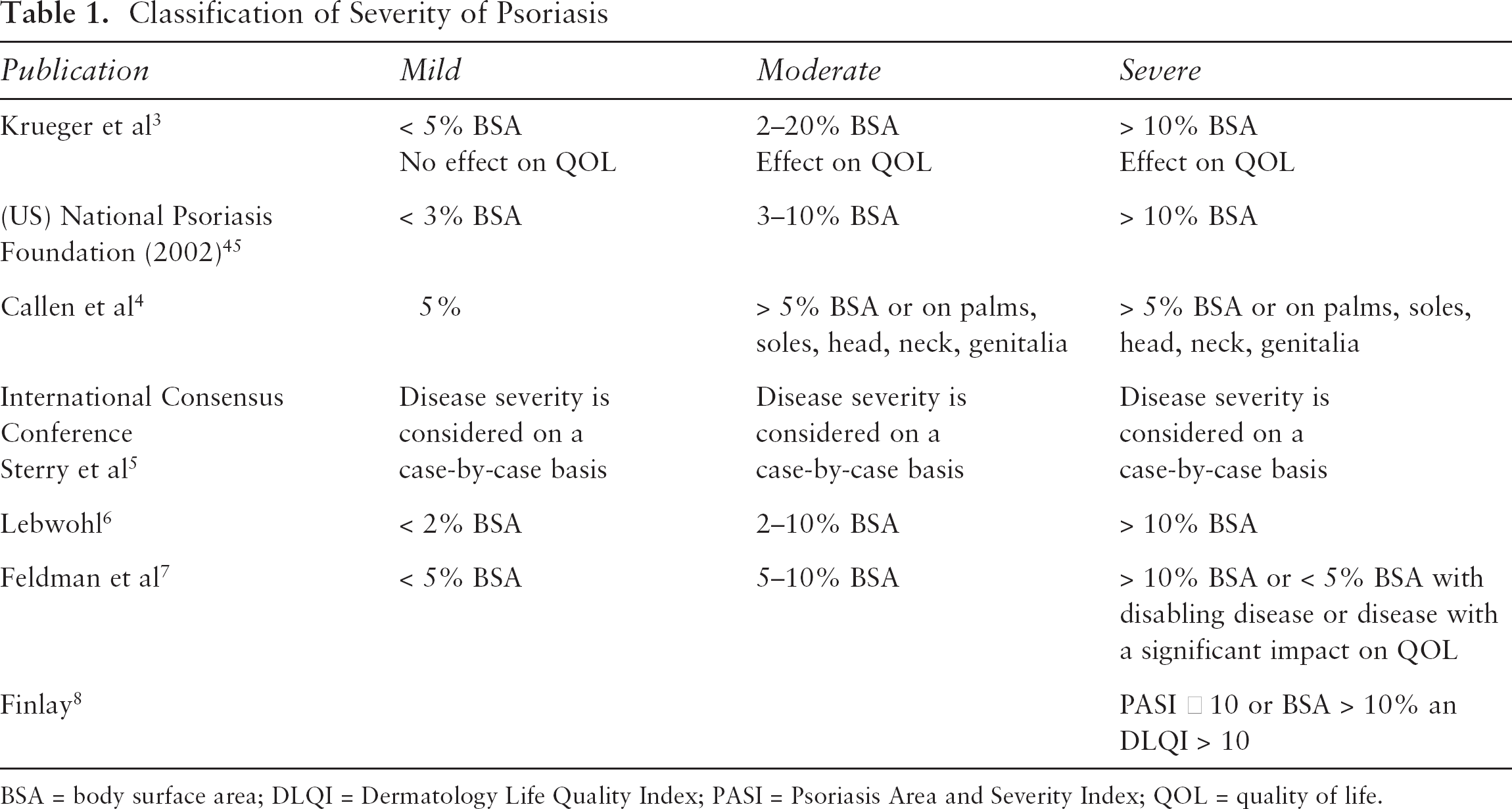
BSA = body surface area; DLQI = Dermatology Life Quality Index; PASI = Psoriasis Area and Severity Index; QOL = quality of life.
Canadian Expert Panel Definition of Moderate to Severe Psoriasis
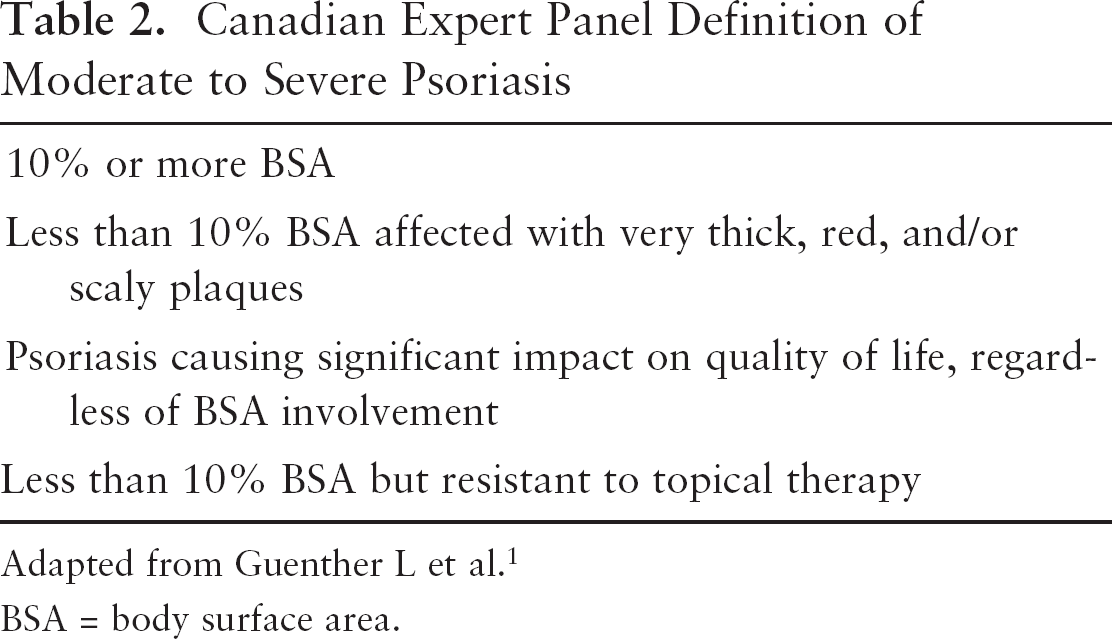
Adapted from Guenther L et al. 1
BSA = body surface area.
As with the other currently indicated biologic treatments for psoriasis in Canada, the approved use specifies patients who are “candidates for systemic therapy or phototherapy.” 2 Etanercept is not appropriate for use in mild psoriasis that may be adequately treated with topical agents. However, in those patients for whom topical therapy is inadequate, the Canadian Psoriasis Expert Panel believes that biologic agents should be considered first-line therapy, on an equal footing with phototherapy and traditional systemics. 1 A decision between the physician and patient may direct choice of treatment among these options.
Age
Etanercept is approved for use in adult patients with plaque psoriasis. 2 It is also indicated for the treatment of juvenile RA (aged 4–17 years), and studies are under way in pediatric psoriasis. However, to date, there are insufficient data on the safe and effective use of etanercept in children with psoriasis.
In clinical trials, 89 psoriasis patients aged 65 years or older were studied; no differences in safety or efficacy were noted in this group, relative to patients younger than 65 years. 2 A retrospective analysis of etanercept in RA patients compared 197 patients □ 65 years old (range 65–86 years) and 931 patients < 65 years old (range 18–64 years). Treatment was found to be effective in both age groups. Etanercept was well tolerated in patients □ 65 years of age, with no consistent differences in rates or types of adverse events compared with the younger group. 2 However, owing to the predisposition of older individuals to infection, greater caution should be used in treating these patients. 2
When choosing the appropriate therapy for moderate to severe psoriasis, comorbidities, contraindications, convenience, response to previous therapy, patient preference, and access also need to be considered.
Psoriatic Arthritis
Etanercept is indicated for reducing the signs and symptoms and inhibiting the progression of structural damage of active arthritis in adult patients with PsA. 2 In Canada, etanercept and infliximab are the only biologics indicated for psoriasis and PsA. As such, identification of patients with PsA may influence the choice of therapy among the biologic agents.
Safety Considerations in Patient Selection
As with any systemic treatment, there are underlying medical conditions that may exclude—or dictate precaution—in the use of etanercept (Table 3).
Safety Consideration in Patient Selection
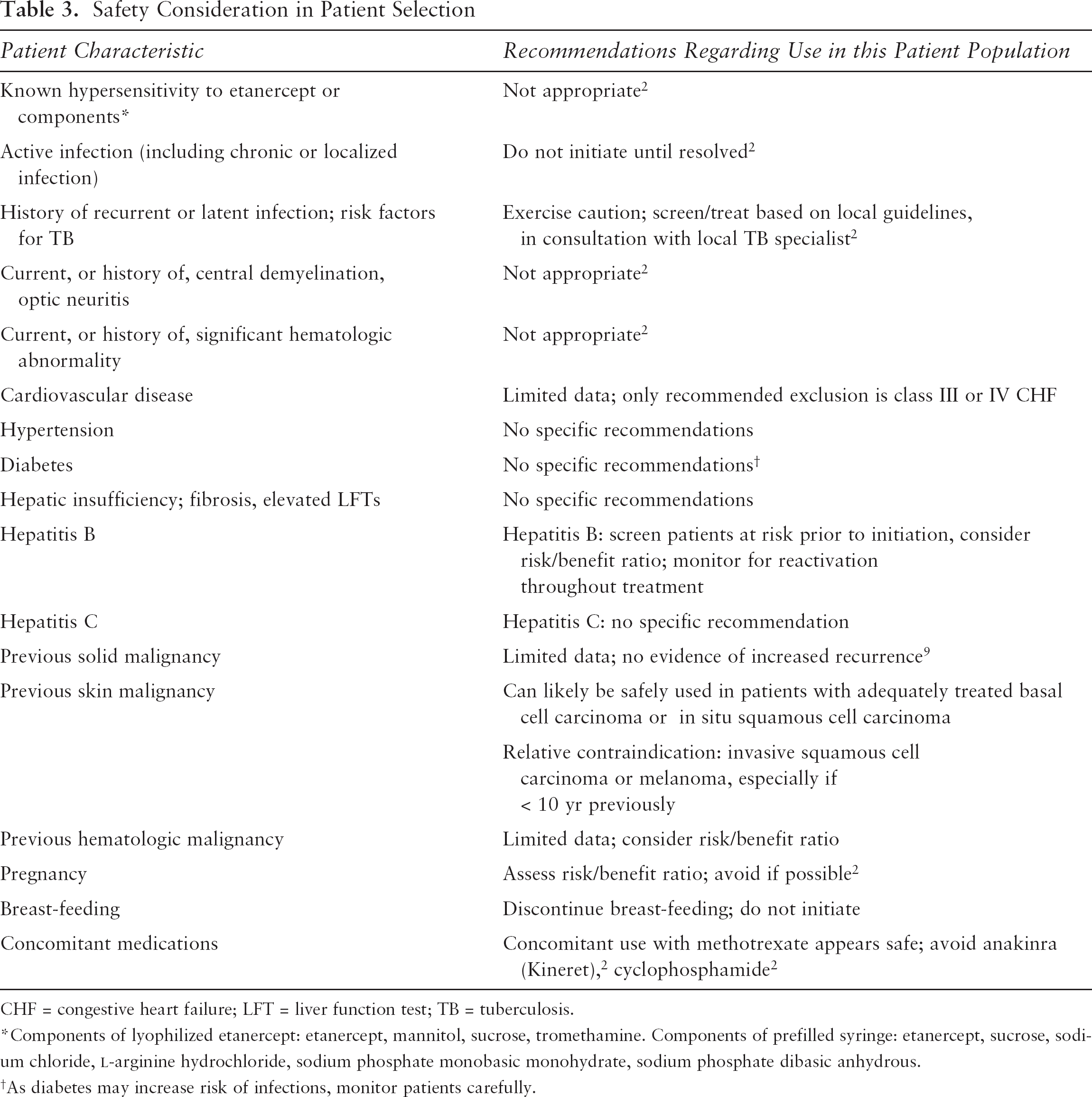
CHF = congestive heart failure; LFT = liver function test; TB = tuberculosis.
Components of lyophilized etanercept: etanercept, mannitol, sucrose, tromethamine. Components of prefilled syringe: etanercept, sucrose, sodium chloride, L-arginine hydrochloride, sodium phosphate monobasic monohydrate, sodium phosphate dibasic anhydrous.
As diabetes may increase risk of infections, monitor patients carefully.
In clinical trials, the incidence of hypertension was low (3%) and was not different from that of placebo-treated patients (3%). 2 Hypercholesterolemia, hyperglycemia, hypotension, myocardial infarction, cardiovascular disorder, and grade 3 or 4 elevations in liver function tests (LFTs) were all reported at frequencies of less than 1%. 2 There does not appear to be an associated increase in cancer recurrence. 9 In a recent study, 20 obese patients with type 2 diabetes were randomized to etanercept (25 mg twice weekly) or placebo for 4 weeks. Endothelial function and metabolic insulin sensitivity remained unchanged with etanercept treatment. 10
There are limited data on the use of etanercept in patients with hepatic or renal insufficiency, and no formal recommendations can be made. A small number of patients (n = 7) in the RA clinical trials tested positive for hepatitis C antibodies. All of these patients continued on etanercept therapy. Only one of the patients had elevated LFTs and was noted to have positive serology for hepatitis C. The patient continued etanercept therapy without a further increase in LFTs (Amgen, data on file, 1999). In five psoriatic patients with hepatitis C, treatment with etanercept was well tolerated, with most patients experiencing decreased viral loads. 11 In a recent double-blind trial, 50 patients with chronic hepatitis C were randomly assigned to receive interferon-α-2b and ribavirin with either etanercept or placebo for 24 weeks. 12 Etanercept, as adjuvant therapy to interferon and ribavirin, resulted in significant improvement in the virologic response and was associated with a decreased incidence of most adverse effects. Of those patients for whom a liver biopsy was conducted at the end of treatment (n = 12), none of the etanercept-treated patients had worsening in the fibrotic stage. 12
Rare cases of hepatitis B virus reactivation have been reported in patients receiving anti-TNF therapy. The risk/benefit ratio should be considered in chronic hepatitis B carriers. If treatment is initiated, patients should be closely followed for signs and symptoms of active infection during treatment and for several months after discontinuation. 13
The pharmacokinetics of etanercept in hemodialysis patients were evaluated in a small study of six patients receiving hemodialysis. Steady-state etanercept levels in these patients were the same when compared with historical values for patients with psoriasis and normal renal function. The authors concluded that hemodialysis did not appear to affect etanercept clearance. 14
Use of Etanercept in Pregnancy and Lactation
Etanercept carries a category B for pregnancy risk in the United States. There are limited data available regarding the use of etanercept in pregnant or lactating women. Although developmental toxicity studies in rats and rabbits show no evidence of harm to the fetus, there are no studies in pregnant women. According to the product monograph, etanercept should not be used in pregnancy unless the benefits outweigh the risks. 2
Preliminary data from the Organization of Teratology Information Services (OTIS) were presented at the American College of Rheumatology annual meeting in October 2004. 15 The observational prospective study, conducted between 1999 and 2004, reviewed outcomes in women with RA who were exposed to anti-TNF therapy during pregnancy. During the study, 29 women were exposed to etanercept. Spontaneous abortion, termination, and malformation rates were similar to those in diseased and nondiseased control groups. The mean birth weight in full-term infants was significantly lower in the anti-TNF group relative to nondiseased controls but was similar to that in RA patients not exposed to anti-TNF treatment. A pregnancy registry has been established in the United States to monitor maternal and fetal outcomes of pregnant women who have been exposed to etanercept. In an April 2005 online survey of 1,023 practicing US rheumatologists, an estimated 493 RA patients became pregnant while on TNF inhibitors and 142 (31.3%) remained on therapy throughout the pregnancy. There were no birth defects, 378 normal deliveries, 9 premature births, 25 miscarriages, and 5 therapeutic abortions. 16
Long-term clinical trials or animal studies have not been conducted to evaluate the effect of etanercept on fertility. Mutagenesis studies, in vitro and in vivo, revealed no evidence of mutagenic activity. 2 Etanercept is not contraindicated in women of childbearing potential; however, risk/benefit should be assessed if the patient becomes pregnant. According to the product monograph, a decision should be made whether to discontinue nursing or to discontinue the drug. 2 It is not known whether etanercept excreted in human breast milk is absorbed systemically after ingestion or whether etanercept interferes with the availability of TNF-α in milk.
Initiating Therapy
Concomitant Therapy
There are limited data on concomitant therapy and transitioning from another psoriatic therapy to etanercept. In clinical trials, traditional systemic psoriasis treatments and phototherapy were terminated prior to study initiation, as were most topical agents. In clinical practice, however, it may not always be ideal to wash out previous systemic therapy.
Transitioning from Cyclosporine, Methotrexate, and other Systemic Therapies
Recently, a retrospective chart review was conducted of patients on a wide range of standard systemic agents. 17 Current therapy at the time etanercept was initiated included cyclosporine (n = 10), methotrexate (MTX) (n = 9), acitretin (n = 18), ultraviolet B (UVB) (n = 13), psoralen plus ultraviolet A (PUVA) (n = 3), mycophenolate mofetil (n = 1), prednisone (n = 1), and alefacept (n = 1). Approximately 50% of patients were able to discontinue their current therapy and be managed on etanercept monotherapy. An additional 23% of patients were able to decrease the dosage of other systemic therapies or phototherapy while being treated with etanercept. The time to discontinuation varied, with a mean of 11 weeks to discontinuation of MTX, 6 weeks for cyclosporine, 14 weeks for acitretin, 10 weeks for UVB, and 18 weeks for PUVA. In another case series of eight patients, etanercept was added to cyclosporine. 18 Cyclosporine was successfully tapered and discontinued in all patients. In a case series of six patients, clinical response was maintained by the addition of etanercept to MTX, allowing the discontinuation of MTX (four patients) or dose reduction (two patients). 19
These reports suggest that etanercept is well tolerated when combined with these agents; however, these studies represent a small number of patients and a short duration of overlap; as such, there are insufficient data to draw conclusions regarding safety.
Studies in PsA and RA have shown that etanercept may be safely used in combination with MTX. Approximately one-third of etanercept-treated patients in RA trials received concomitant MTX. 2 Greater improvement in joint symptoms has been observed by using this combination (compared with monotherapy) in RA, with no clinically relevant pharmacokinetic interactions. It is not known if the combination of MTX and etanercept offers greater efficacy in psoriasis. However, it appears that MTX and etanercept can be safely used in combination; however, there are limited data in psoriasis.
In RA patients, the addition of etanercept to a stable dose of either gold (n = 19), hydroxychloroquine (n = 50), sulfasalazine (n = 50), 20 or leflunomide (n = 11) 21 resulted in greater efficacy. Treatment was discontinued owing to adverse events in 5% on gold (one proteinuria), 10% on hydroxychloroquine (one each of septic wrist and bilateral pneumonia, breast cancer, tongue squamous cell cancer, rash + diarrhea, and optic neuritis), and 10% on sulfasalazine (one each of otitis media, pericarditis, rash, severe gastroenteritis, and increased LFTs). Two patients on leflunomide had serious adverse events (one erysipelas and arthritis flare, one colitis resulting in gastrointestinal gangrene and death). Patients on these disease-modifying antirheumatic agents should be carefully monitored for adverse events.
Concomitant Use with Cyclophosphamide
Concurrent use of etanercept with cyclophosphamide is not recommended. 2 In a study of patients with Wegener's granulomatosis, six patients on cyclophosphamide + etanercept developed noncutaneous solid tumors versus none in the control group (standard therapy with cyclophosphamide or MTX + steroids, without etanercept). 22
Concomitant Use with Phototherapy
A small study (10 severe psoriasis patients) evaluating the safety and efficacy of combination oral PUVA and etanercept 25 mg twice was presented at the American Academy of Dermatology annual meeting in 2005. 23 The interim results suggest that combination PUVA and etanercept may be efficacious and safe. An ongoing phase 4 trial has been designed to evaluate the effectiveness of combination therapy with etanercept and narrowband UVB. 24 Interim results have not yet been presented. An ongoing phase 4, 12-week, open-label, single arm prospective study of 86 patients receiving etanercept (50 mg twice weekly subcutaneously) and narrowband UVB (three times weekly with dose escalation at 10% to 15% of preceding dose, depending on patient's response to preceding dose; initial dosage determined by patient Fitzpatrick skin type) has been designed to evaluate the effectiveness of this combination therapy. 24 Interim results presented by Kircik and colleagues suggested that etanercept and NB-UVB combination therapy was efficacious and generally well tolerated in adults for the treatment of the signs and symptoms of chronic moderate to severe plaque psoriasis. Eighty-five percent of patients achieved a Psoriasis Area and Severity Index (PASI) 75 response, 58% of patients achieved a PASI 90 response, and 26% of patients achieved a PASI 100 response after 12 weeks of combination therapy. 24
Concomitant Use with other Biologics
There is at least one report involving two patients in which enhanced efficacy without additional toxicity was seen when alefacept (Amevive) was added to a treatment regimen of etanercept. 25 However, in general, the data on concurrent use of biologics for the treatment of psoriasis are minimal. Although combinations of certain biologic agents may be rationalized based on their distinct mechanisms of action, the safety of such combinations has not been studied. In fact, recent studies in rheumatology suggest that combining biologic therapies (abatacept combined with other biologics) may be associated with a greater risk of infections, including serious infections. 26 Until sufficient safety data exist, their concomitant use should be cautioned.
One biologic combination that should clearly be avoided is the concomitant use of etanercept with anakinra (Kineret), an interleukin-1 blocker. In a multicenter, double-blind, 24-week study involving 242 subjects with active RA despite MTX therapy, the rate of serious infections was higher in the combination etanercept and anakinra (3.7–7.4%) arms than in those on etanercept alone (0%). 27 Additionally, two patients treated with the combination of etanercept and anakinra developed neutropenia. There was no statistical difference in the efficacy of combination therapy with etanercept plus anakinra versus etanercept alone.
Use in Patients Who Have Failed Previous Systemic Therapy or other Biologics
A post hoc analysis of a large randomized trial was conducted to assess the value of etanercept in patients refractory to other systemic therapies. 28 Of the 521 patients who received previous systemic therapy or phototherapy, 337 patients (65%) failed at least one of those therapies. In these patients, the PASI 75 response rate was similar to that in those who had not failed previous therapy. 29
Recently, a small study (n = 67) examined the response to etanercept (25 mg twice weekly—half the Canadian approved dose) in psoriasis patients who had failed at least one systemic drug. 30 Twenty-four patients had previous therapy with another biologic (either infliximab or efalizumab). Over 40% of these patients achieved a PASI 50 response at week 12. Of note, the response rate was considerably higher in those patients who had failed treatment with the T-cell modulator efalizumab (80% PASI 50) compared with those who had not responded to another anti-TNF agent, infliximab (25% PASI 50).
Dosing
The recommended starting dose of etanercept for adult patients with psoriasis is 50 mg given twice weekly—3 or 4 days apart—for 3 months followed by a reduction to a maintenance dose of 50 mg per week. 2 This step-down dosing approach allows patients to be maintained long term on a lower dose of etanercept. In a clinical trial, 77% of patients maintained their response (□ PASI 75) with this maintenance dosing (at 6 months); 97% maintained at least a PASI 50 response. 28
When deciding what to do for those patients who lose response, it should be noted that a maintenance regimen of 50 mg twice weekly is also efficacious. 2 Long-term treatment at 50 mg twice weekly has been studied and shows sustainability through 2 years of continuous treatment. 31 Increasing the dose to 50 mg twice weekly, following an unsuccessful step-down dosing, has not been assessed. The maximum tolerated dose of etanercept has not been established in humans. No dose-limiting toxicities have been observed during clinical trials. Etanercept is not adjusted for weight, and doses exceeding 50 mg twice weekly were not studied in clinical trials. In psoriasis trials, some patients initiated treatment with a dose of 25 mg twice weekly (equivalent to the maintenance dose, or “psoriatic arthritis” dose). Although a significant skin response was observed in these patients, the response was more rapid in patients who initiated treatment with 50 mg twice-weekly etanercept. 28
Etanercept is administered by subcutaneous injection and is available in two formats: a single-use prefilled syringe and a multiple-use vial. 2 Prefilled syringes and lyophilized etanercept may be kept until the listed expiry dates. Regardless of the format, etanercept should be refrigerated at 2Þ to 8ÞC and not frozen. 2 The 50 mg prefilled syringe was recently introduced for greater convenience. The multiple-use vial contains 25 mg of lyophilized etanercept, which the patient must reconstitute with 1 mL of supplied sterile bacteriostatic water prior to injection. A vial adapter is supplied to help in reconstitution. Unused reconstituted solution should be refrigerated and used within 14 days. It should be noted that the needle cover of the prefilled syringe contains natural rubber (latex), which may cause allergic reactions in individuals sensitive to this substance. 2
Sites for injection include the thigh, abdomen, or upper arm. Sites should be rotated, located at least 1 inch from sites of recent injections. Etanercept should not be injected directly into plaques or skin that is tender, bruised, red, or hard. 2 A patient support program (see below) is available in Canada for initial injection training.
Continuous or Intermittent Therapy
A key advantage to the biologic agents is their safety profile in terms of less evidence of end-organ toxicity compared with some traditional systemic agents. This allows for continuous use of some biologics2,32 rather than the need for rotational therapy. Continuous use is not recommended for all biologic therapies. For example, alefacept is administered as 12-week courses, with minimum 12-week intervals between courses. 33
Etanercept has been well studied for use as a continuous treatment. Maintenance of skin clearance is best achieved by continuous therapy. However, if treatment discontinuation is desired or warranted, etanercept can be safely stopped. The time to relapse (defined as 50% of treatment response) is approximately 12 weeks. 34 In clinical trials, etanercept discontinuation was not associated with rebound. 34 Moreover, during retreatment, the responses were similar to those seen in the initial treatment phase. 34 This provides flexibility in integrating etanercept into a therapeutic strategy.
Combination or add-on therapy may also prove to be effective in patients who lose response. However, the efficacy of specific combinations in these patients has not been well studied.
Expected Response
The time to etanercept response in psoriasis patients has been documented in controlled clinical trials. Statistically significant improvements in PASI scores were noted by 2 weeks (215–18% improvement),28,35 although clinically meaningful improvement may take longer. Among patients who achieved a PASI 75 response, the median time to clinical response as defined by PASI 50 and PASI 75 was approximately 1 and 2 months, respectively. Overall, approximately 50% of patients will achieve a PASI 75 response and 75 to 80% will achieve a PASI 50 response within 12 weeks. 2 The optimal duration of treatment has not been defined, and treatment may be continued at the physician's discretion.
Managing Therapy
Monitoring
Although there is no required laboratory monitoring for etanercept therapy, 2 prior to initiation of any TNF inhibitor, most physicians perform a tuberculosis (TB) skin test (purified protein derivative [PPD]) and order a chest radiograph. 16 If latent TB is confirmed, etanercept therapy may be initiated provided that the patient is started on prophylaxis treatment for TB and that this prophylaxis treatment is continued for the recommended duration according to local guidelines. 36 There have been rare reports of reactivation of TB after a median of approximately 1 year of etanercept therapy, although this may represent acquisition of a new infection. 37 Pretreatment liver enzymes should be considered in patients at risk of hepatic impairment (eg, previous or concurrent MTX treatment, patients at risk of hepatitis). Pretreatment testing for hepatitis B antigen should be considered in high-risk individuals since the viral load might increase if etanercept is given to patients with hepatitis B infection. 13 Laboratory testing may also be useful to assess for hematologic abnormalities. The recently published British Association of Dermatologists guidelines recommend a complete blood count, creatinine, blood urea nitrogen, electrolytes, and LFTs after 3 months of therapy and then every 6 months. 38 Given that rare reports of drug-induced lupus have been reported, 2 a pretreatment antinuclear antibody (ANA) is recommended by some16,38; however, a positive ANA is not considered a contraindication since many healthy individuals may have a positive ANA. One-third of healthy individuals have a titer of 1:40. 39 In addition, there is no evidence that the presence of ANA, anti–double-stranded deoxyribonucleic acid (anti-dsDNA), or anticardiolipin antibodies is associated with an increased risk of development of drug-induced lupus. If, however, a patient develops signs suggestive of lupus erythematosus, lupus serology (eg, ANA, anti-dsDNA, anticardiolipin antibodies) should be considered.
Patients should be informed about possible adverse events that may arise, including those that should be reported to a health care provider (Tables 4 and 5). They should also be told to inform their physician if they have a planned surgery or vaccination.
Checklist for Patient Monitoring during Therapy
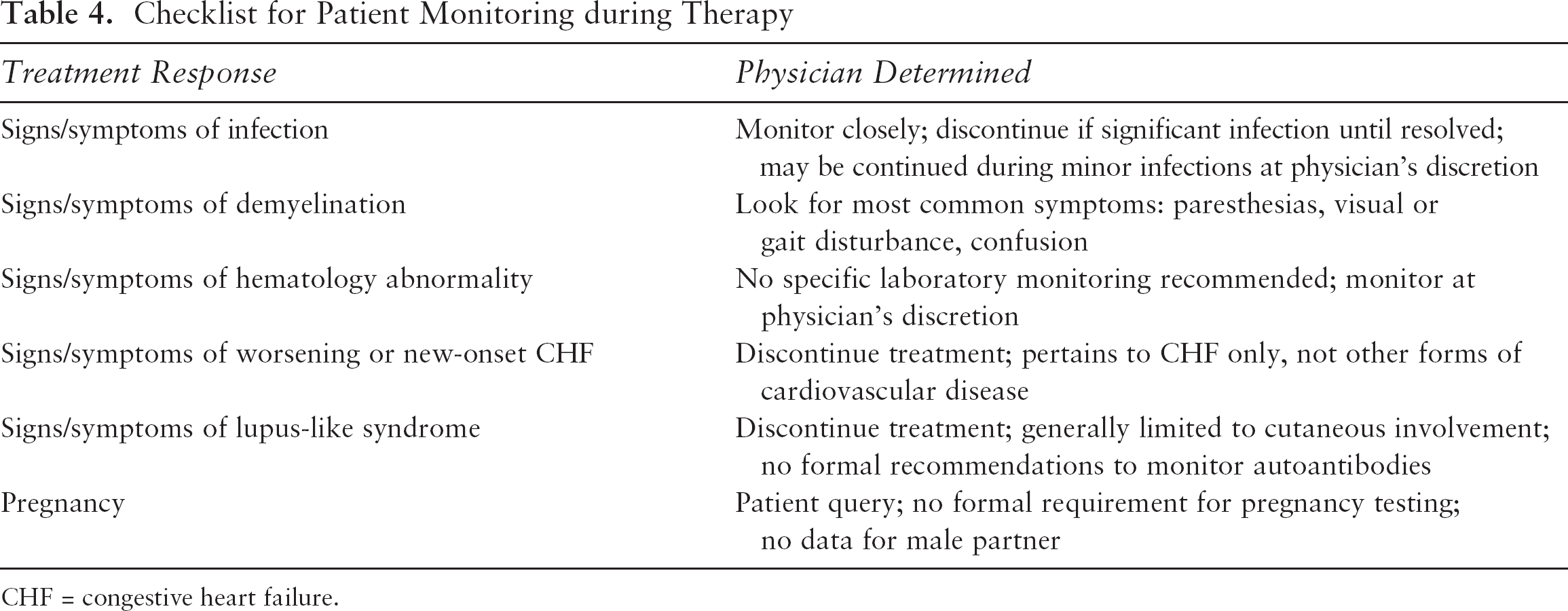
CHF = congestive heart failure.
Events that Should Be Reported to a Physician
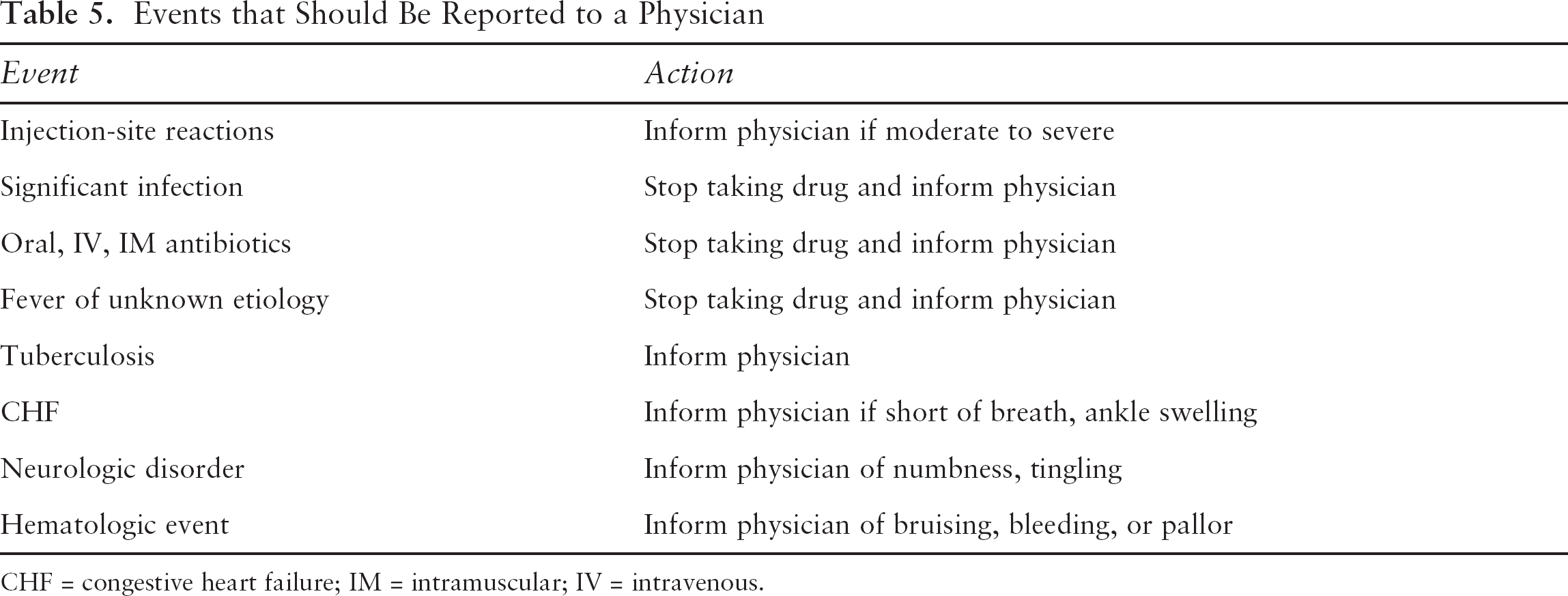
CHF = congestive heart failure; IM = intramuscular; IV = intravenous.
Injection-Site Reactions
During clinical trials in patients with psoriasis, approximately 14% of patients treated with etanercept developed injection-site reactions (ISRs) during the first 3 months of treatment. These ISRs were described as mild to moderate (erythema and/or itching, pain, or swelling) and rarely led to discontinuation. 2 Generally, ISRs are seen in the first month of treatment and last 3 to 5 days. The pattern of ISRs is not consistent with sensitization; the reactions decrease in frequency over time, do not worsen, and are not associated with anaphylaxis (Amgen, data on file 1999). Approximately 90% of ISRs resolve without treatment. Moderate to severe reactions may be treated with oral antihistamines and/or topical corticosteroids. 2
Redness at a previous injection site with subsequent injections was observed in approximately 7% in controlled clinical trials. 2 As with ISRs, these reactions generally occurred in the first month of treatment, lasted 3 to 5 days, were mild to moderate in intensity, and did not necessitate treatment discontinuation.
Discontinuation or Interruption of Treatment
Although skin clearance is best maintained by continuous treatment, there may be circumstances under which it is necessary to temporarily or permanently discontinue therapy (Table 6). If treatment is temporarily discontinued, disease relapse occurs gradually. In clinical trials, the median time to relapse (loss of 50% of improvement) was approximately 3 months. 35 Discontinuation was not associated with rebound (defined as PASI □ 125% of baseline). When treatment is reintroduced, responses similar to those in the initial treatment phase can be expected. 34
Reasons to Consider Discontinuation of Etanercept Therapy
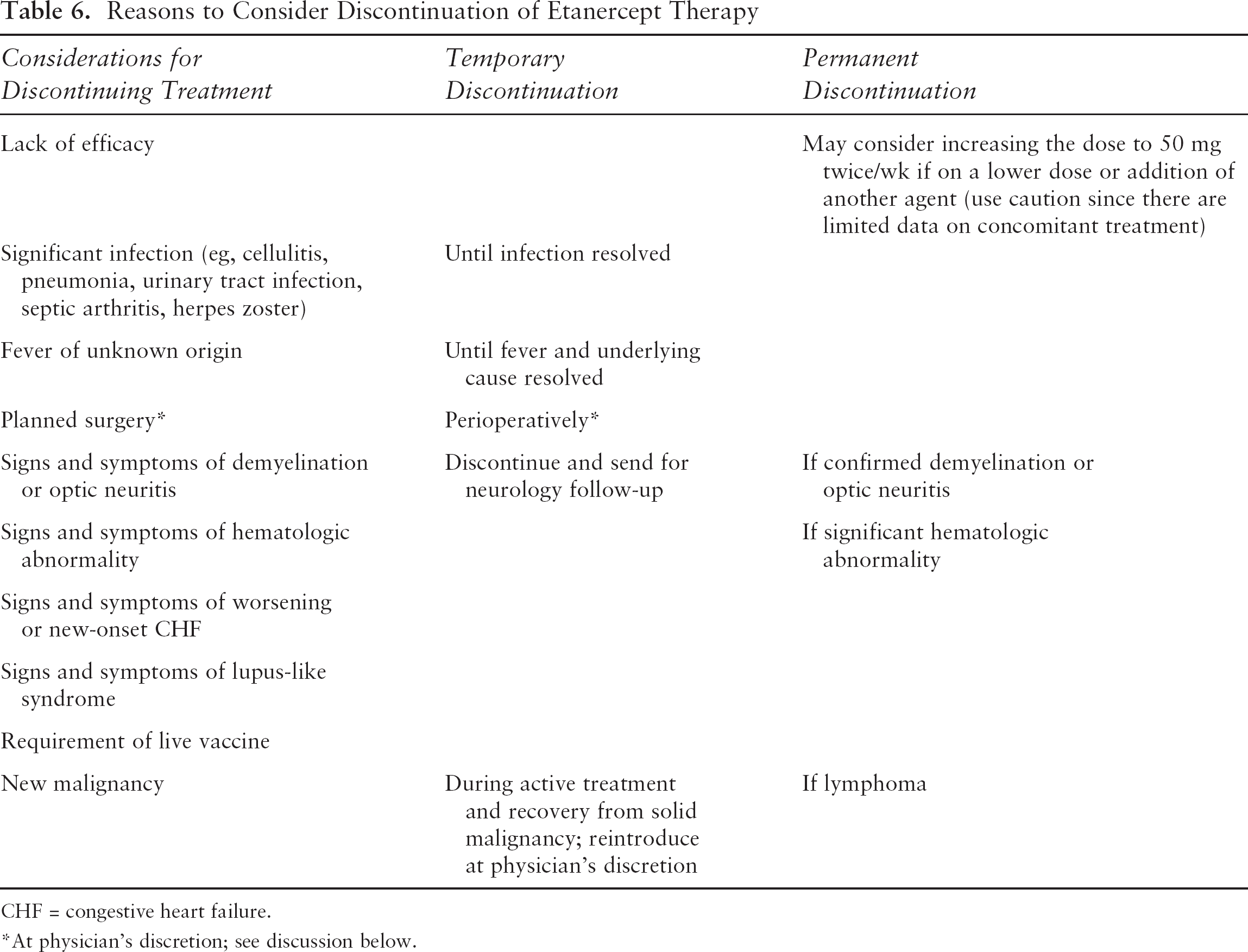
CHF = congestive heart failure.
At physician's discretion; see discussion below.
Etanercept should not be continued in patients who fail to achieve a significant response. The British guidelines recommend discontinuation of biologics after 3 months if there is insufficient efficacy defined as achievement of < PASI 50, less than 50% reduction in body surface area, and < 5-point improvement in the Dermatology Life Quality Index (DLQI). 38 In Canada, these measures are not part of routine clinical practice. Among patients who achieved a PASI 75 response in clinical trials, the median time to clinical response as defined by PASI 50 and PASI 75 was approximately 1 and 2 months, respectively. In clinical trials, it was observed that a subset of patients responded at later time points. Of those patients not yet responding (PASI 75) by 12 weeks, approximately one-third responded by 24 weeks. 28 Although no formal recommendations exist, most patients who respond will do so by 24 weeks. The decision to stop treatment in those not responding should be at the discretion of the treating physician.
Surgery
The effects of etanercept on surgical outcomes are not well defined. Potential complications associated with the use of biologics perioperatively include infections, delayed wound healing, or impaired coagulation. During clinical trials, the decision of whether to continue etanercept perioperatively was left to the discretion of the physician. The safety of surgical procedures in patients receiving etanercept was not specifically evaluated.
Studies of the postoperative complications associated with etanercept and infliximab therapy exist but provide conflicting results; one chart review of 91 patients undergoing an orthopedic procedure suggests a higher risk of postoperative infection, 40 whereas a small prospective orthopedic study showed no increased risk of healing or infectious complications. 41
Although there are no specific recommendations for discontinuing etanercept perioperatively, clinicians should assess each patient individually to determine if it is appropriate to temporarily discontinue therapy. The potential risk associated with the type of surgery should also be considered. In instances in which the surgical field is not sterile and there is a definite risk of infection (eg, bowel surgery), serious consideration should be given to temporary discontinuation of etanercept. Of note, among the available anti-TNF therapies, etanercept has the shortest half-life (24 days), 2 so elimination time is significantly shorter. In response to the question of how long before major surgery anti-TNF therapy be suspended, a recent survey of practicing US rheumatologists reported a mean of 1.7 weeks. 16
Immunizations
Patients treated with etanercept may receive concurrent vaccinations, except for live vaccines. The 23-valent pneumococcal vaccine (Pneumovax), inactivated influenza vaccine (Vaxigrip), and inactivated influenza vaccine surface antigen (Influvac) are killed vaccines that may be safely used, whereas the intranasal FluMist is a live vaccine and should be avoided. No data are available on the secondary transmission of infection by live vaccines in etanercept-treated patients. 2
The data regarding safety and efficacy of vaccine administration in patients receiving etanercept are limited.42–44 In general, the data suggest that patients receiving etanercept can mount an effective immune response to pneumococcal or influenza vaccines, but the antibody titers tend to be lower when compared with patients not receiving anti-TNF therapies. 44 The clinical significance of the lower titers is unknown.
Support Programs
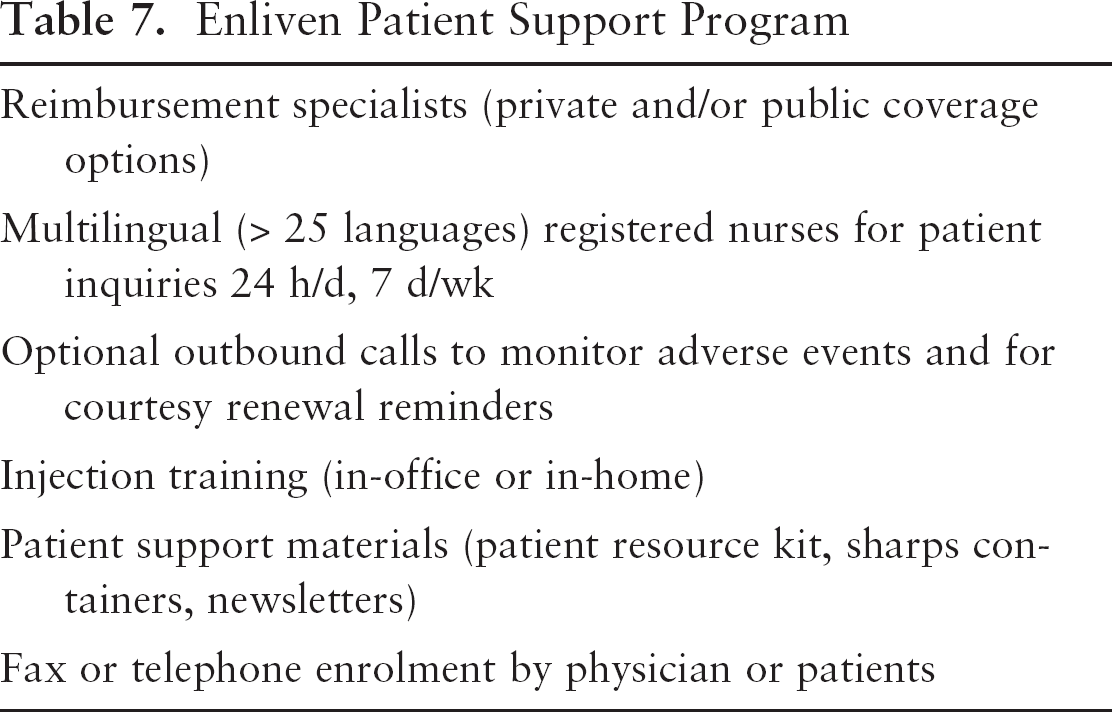
Support programs have been developed by the manufacturers of biologic therapy to assist patients with access, reimbursement, injection training, and drug administration. These programs are intended to help free up physician time while encouraging better patient compliance. A patient support program for etanercept is available in North America (Enliven) and provides assistance (Table 7).
Enliven Patient Support Program
Conclusions
Etanercept should be considered first-line therapy for patients with moderate to severe plaque psoriasis, particularly if they also suffer from psoriatic arthritis. It should be administered by subcutaneous injection in a dose of 50 mg twice weekly for 3 months, followed by dose reduction to 50 mg/wk. A maintenance regimen of 50 mg twice weekly is also safe and efficacious. There are limited data on the use of concomitant therapy with other systemic agents; however, data exist suggesting dose-sparing and safety with cyclosporine, acitretin, and phototherapy. Concomitant therapy with MTX appears to be safe based on limited data. Anakinra and cyclophosphamide should be avoided owing to safety concerns (infections and solid tumors, respectively). Although the product monograph does not recommend routine monitoring, a baseline PPD and chest radiograph should be considered. Screening for hepatitis B in high-risk patients should also be considered. Although there are insufficient data to recommend additional laboratory testing, some physicians may choose to periodically monitor the complete blood count and liver enzymes. Consideration should be given to discontinuation of etanercept perioperatively. Live vaccines should not be administered during therapy, whereas killed ones can be safely administered. A patient support program (Enliven) is available for assistance in reimbursement, injection training, patient support materials, and nursing expertise for patient inquiries.