
Abstract
Background:
Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), collectively referred to as nonmelanoma skin cancer (NMSC), cause significant morbidity and generate a substantial cost to the health care system. Canadian data on the incidence of NMSC are lacking.
Objective:
To study the incidence and characteristics of NMSC in New Brunswick, Canada (population 729,498 people in 2001), by using the Provincial Cancer Registry.
Method:
Data were obtained from 1992 to 2001 from the New Brunswick Provincial Cancer Registry, to which reporting of all cancers is mandatory. Multiple tumors of a given histologic type are recorded only once in the registry per individual per lifetime. A descriptive analysis of incidence rates of BCC and invasive SCC of the skin was performed in relation to gender, age, and anatomic location. The main outcome measures were the age- and sex-specific incidence rates of BCC and SCC. Age standardization was performed using the Canadian, US, and world standard populations.
Results:
When adjusted to the world standard population, the age-standardized incidence rates (ASIRs) per 100,000 population for BCC from 1992 through 2001 were 87 for males and 68 for females. For invasive SCC, the ASIRs per 100,000 population were 34 for males and 16 for females. There was an increasing incidence trend for both BCC and invasive SCC over the 10-year study period, with minimal change in the incidence of SCC in women. The overall ratio of BCC to invasive SCC in the population was 2.8 to 1. The approximate lifetime probabilities of developing BCC and invasive SCC were 13% and 5%, respectively.
Conclusions:
The incidence of NMSC in the province of New Brunswick is similar to that reported from 1973 through 1987 in the province of British Columbia, higher than those reported in most parts of Europe, and lower than all published rates in the United States and Australia. Owing to the inability of the registry to account for tumor multiplicity, the actual annual number of all NMSC lesions in this population is likely much higher.
BASAL CELL CARCINOMA (BCC), estimated to account for more than one-third of all cancers in the United States, has been recognized as the single most common malignancy occurring in the white populations of North America and Australia.1,2 Although less common than BCC, squamous cell carcinoma (SCC) of the skin metastasizes more frequently and has a higher mortality rate. 3 BCC and SCC are collectively referred to as nonmelanoma skin cancer (NMSC). Although the mortality rate of NMSC is low, these malignancies generate considerable morbidity and substantial health care costs. 4
Studies examining the incidence of NMSC vary widely in terms of their methodology, making comparison between populations difficult. 5 Several investigators in the United States and Australia have estimated NMSC incidence using population-based screening methods and surveys.1,2 Worldwide, relatively few cancer registries include NMSC as part of their data collection. It has been argued that cancer registries likely underestimate NMSC incidence owing to incomplete tumor registration, as well as the unknown number of clinically diagnosed skin cancers that are treated destructively and without histologic confirmation. 6 However, population-based cancer registries remain useful resources for estimating the incidence of NMSC, as well as for evaluating changes in disease burden over time. 7
The New Brunswick Provincial Cancer Registry collects information on all cancers, including BCC and invasive SCC, in the form of a province-wide tumor database. The yearly incidence rates for BCC and invasive SCC are herein presented for the province of New Brunswick, Canada, from 1992 to 2001.
Methods
New Brunswick Provincial Cancer Registry
The New Brunswick Provincial Cancer Registry was established in 1952, and data on NMSC have been recorded since 1989. The medical system in New Brunswick is publicly funded, with universal access to health care for all Canadian citizens. Physicians in New Brunswick routinely submit all tissue removed from the body for pathologic examination. In turn, the seven regional pathology laboratories in the province are mandated to submit all pathology reports of tumors to the cancer registry.
Information collected on each patient includes their name, date of birth, provincial health insurance number, demographic information, treating physician, gross and microscopic tumor description, anatomic site, and method of diagnosis. From 1992 to 2000, the registry used the ICD-O2 (International Classification of Diseases for Oncology, Second Edition, World Health Organization) and in 2001 the ICD-O3 classification to code all NMSC reports.
Only patients with newly incident tumors are registered in the database, and only one tumor of a particular type per lifetime is counted per patient. Recurrent and subsequent primary tumors of the same histologic type from individuals with a history of BCC or invasive SCC are excluded from the registry.
Study Population
New Brunswick is a province located on the Atlantic coast of Canada, between latitudes 45 and 48 degrees north, with a population of 729,498 people. 8 The population is predominantly Caucasian, of mixed western European descent, with 3.4% of the residents being aboriginal Canadians. 8 Approximately 50.4% of the residents live in urban areas and 49.6% live in rural areas. 8
Incidence of NMSC
The age- and sex-specific incidence rates for BCC and invasive SCC were calculated using Provincial Cancer Registry data for the years 1992 to 2001. Age-specific incidence rates were determined using standard ascending 5-year age groups (ie, 20–24, 25–29, 30–34 years). Incidence rates were adjusted to the 1991 Canadian, the 2000 US, and the 2000 world standard populations to allow for comparison with other published reports.
All cases of NMSC were checked to ensure that a given individual with BCC or SCC was not included more than once in the database for a given tumor diagnosis. Eight cases of BCC and four cases of invasive SCC were manually removed owing to duplication. Thirty-six patients who had a clinical diagnosis of BCC or SCC at the time of radiotherapy and had a clinical diagnosis sent to the cancer registry but no histologic confirmation were excluded from the data analysis. All cases of SCC in situ were excluded. Individuals with both one BCC and one invasive SCC were included in the data analyses.
Anatomic sites were defined using the ICD-O3 topographic codes C44.0, skin of the lip; C44.1, eyelid; C44.2, external ear; C44.3, skin of other and unspecified parts of the face; C44.4, scalp and neck; C44.5, trunk; C44.6, upper limb and shoulder; C44.7, lower limb and hip; C44.8, overlapping lesion of skin; and C44.9, skin not otherwise specified. Tumors occurring on the skin of the vulva (C51), penis (C60.9), and scrotum (C63.2) were excluded from this study to allow for comparison with other studies of NMSC incidence.9,10
The lifetime probabilities of developing BCC and invasive SCC in the New Brunswick population were calculated with DevCan 6.1.1 from the Surveillance, Epidemiology, and End Results Program, using cross-sectional cancer rates and death rates. 11
Results
Incidence
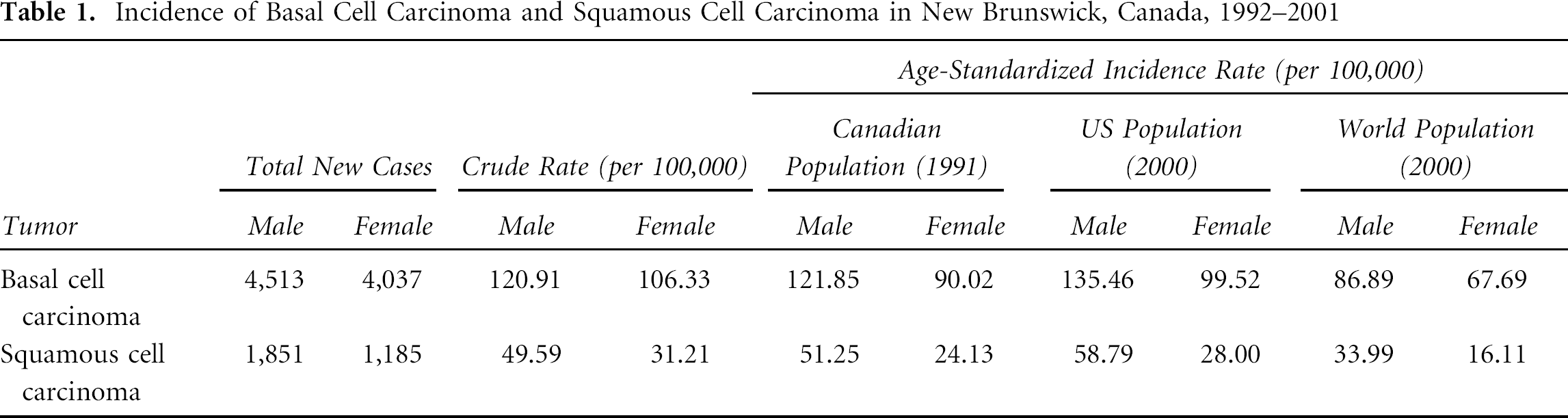
Between 1992 and 2001, 8,550 newly incident cases of BCC (4,513 male, 4,037 female) and 3,036 new cases of invasive SCC (1,851 male, 1,185 female) were registered in the database (Table 1). Table 1 summarizes the crude incidence rates of BCC and invasive SCC in New Brunswick, as well as the age-standardized incidence rates (ASIRs). When age-standardized to the 2000 world population, the incidence rates (per 100,000 population) in New Brunswick of BCC were 86.9 (male) and 67.7 (female) and those of invasive SCC were 34.0 (male) and 16.1 (female). In the population of New Brunswick, this translates into an approximate lifetime probability of 13% of developing BCC and 5% of developing invasive SCC. BCC represented approximately 74% of NMSC in the study population, with an overall ratio of BCC to invasive SCC of 2.8 to 1.
Incidence of Basal Cell Carcinoma and Squamous Cell Carcinoma in New Brunswick, Canada, 1992–2001
Age-Specific Rates
In New Brunswick, the median age at first diagnosis of BCC was 67 years in both men and women. The median age at first diagnosis of invasive SCC was 72 years in men and 76 years in women. The incidence of both BCC and invasive SCC increased with age (Figure 1). BCC was slightly more common in women than men between the ages of 30 and 44 years, after which the incidence of BCC rose much more steeply in men. Invasive SCC was more common in men than women in all age groups.
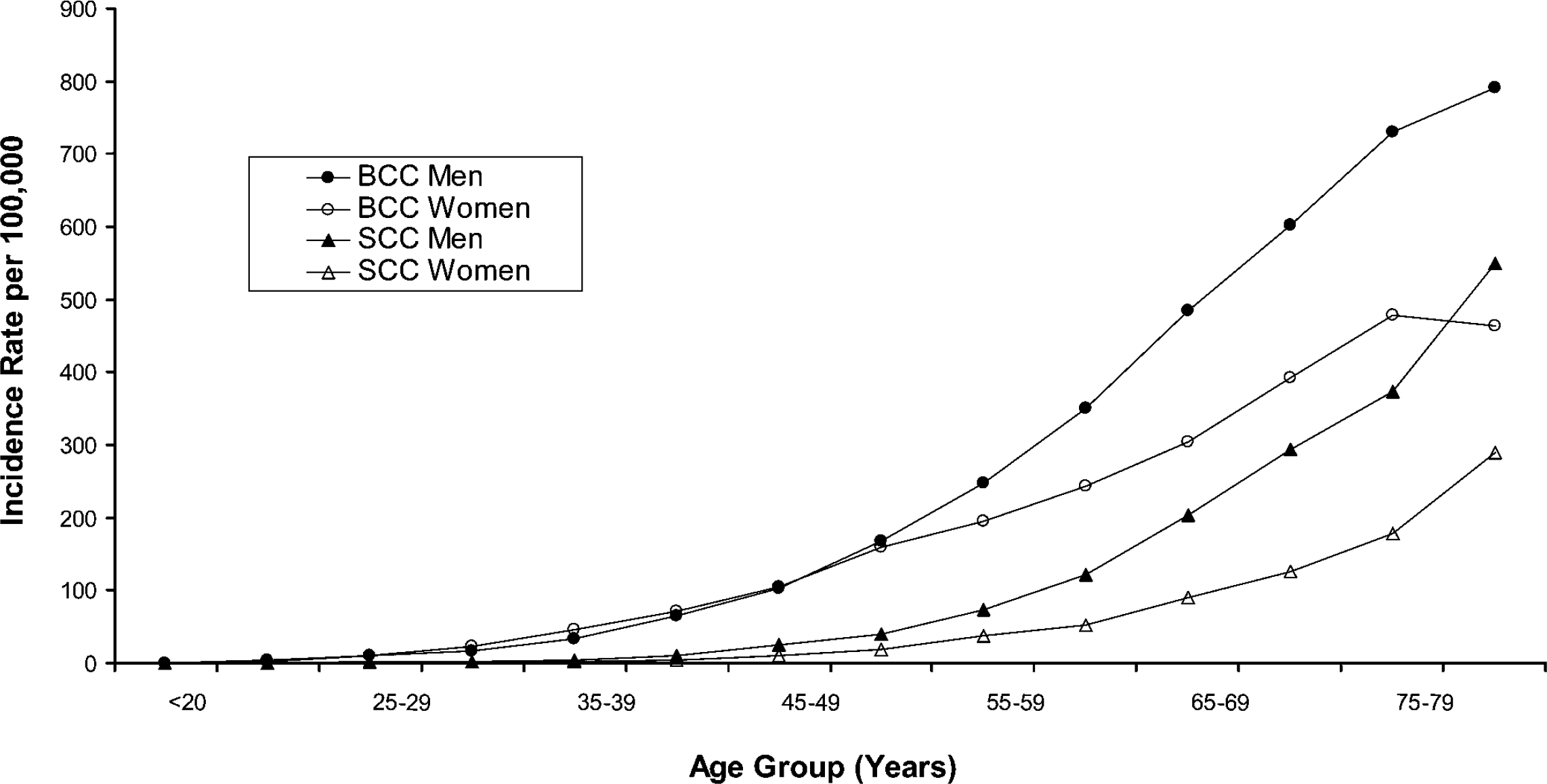
Age-specific incidence rates for basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) in New Brunswick, Canada, 1992–2001.
Incidence Rates, 1992–2001
There was an increase in the incidence of BCC in New Brunswick among both men and women over the 10-year study period (Figure 2). The incidence of SCC in men increased modestly, whereas the incidence of SCC in women remained relatively stable (see Figure 2).
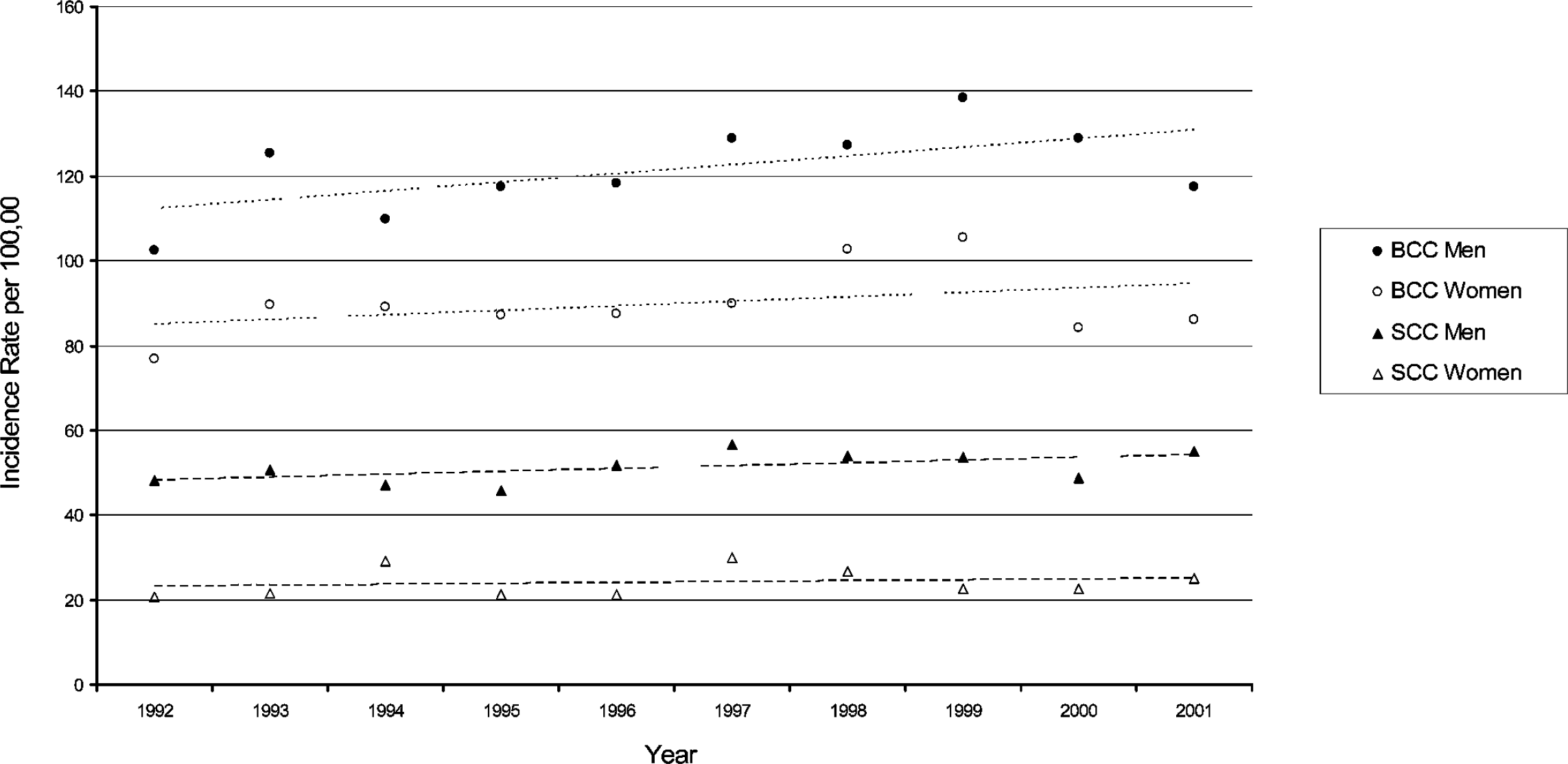
Trends in incidence rates of basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) in New Brunswick, Canada, 1992–2001 (age-standardized to 2000 world population).
Anatomic Distribution
For men and women, the most frequent anatomic location of both newly incident BCC and invasive SCC was the face (Table 2). For BCC, the trunk was the next most common tumor site in both sexes. BCC was disproportionately more common on the ear in men (11.6% of tumors) than women (2.2% of tumors). Among men, invasive SCC on the ear was the second most commonly diagnosed tumor (20.6%), followed by the upper limb or shoulder (16.9%). Among women, invasive SCC was relatively uncommon on the ear (2.6% of tumors); instead, the second most common site of SCC in women was the upper limb or shoulder (20.6% of tumors). For both BCC and SCC, the lower limb was a disproportionately more frequent tumor location in women (6.5% and 11.1% of tumors, respectively) than men (1.4 and 1.9% of tumors, respectively).
Body Site Distribution of Basal Cell Carcinoma and Squamous Cell Carcinoma in New Brunswick, Canada, 1992–2001
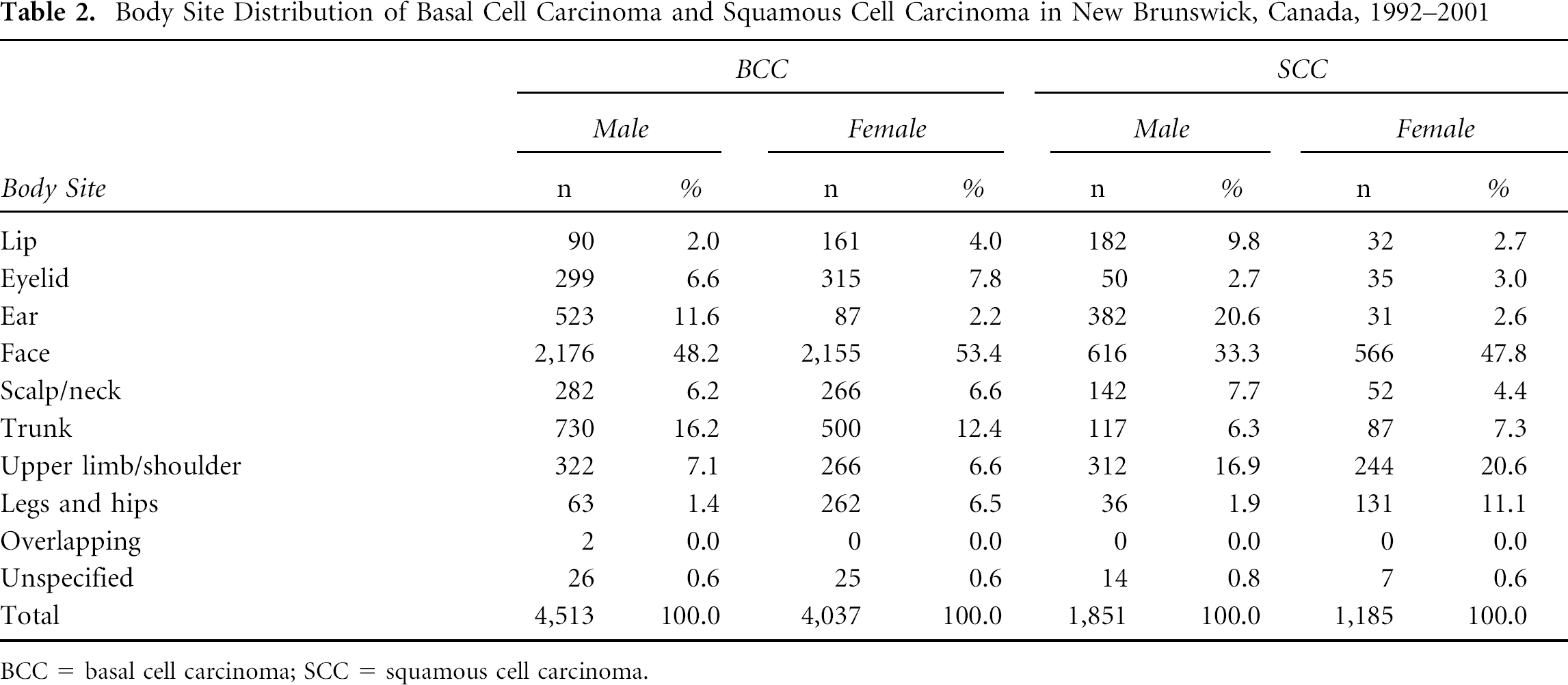
BCC = basal cell carcinoma; SCC = squamous cell carcinoma.
Discussion
The incidence rates for BCC (122 male, 90 female) in New Brunswick from 1992 to 2001, when age-standardized to the 1991 Canadian population, were remarkably similar to those reported in the province of British Columbia (120 male, 92 female) from 1973 through 1987. 9 The incidence rates of invasive SCC in New Brunswick, however, were higher (51 male, 24 female) than those in British Columbia (31 male, 17 female). Both provinces have temperate climates and similar annual cumulative ultraviolet irradiance. Importantly, the British Columbia Cancer Registry is notably different in that it counts more than one primary tumor of a given type per patient, whereas the New Brunswick Cancer Registry tabulates only one tumor of a given type per patient per lifetime. 9
There was a gradual increase in BCC incidence in New Brunswick over the 10-year study period, a modest increase in SCC incidence in men, and minimal change in the incidence of SCC in women. The average annual percent change for BCC was +0.7% for males and +1.0% for females and for SCC was +0.5% for males and +0.8% for females.
The Manitoba, Cancer Registry, with similar criteria to New Brunswick for NMSC registration, showed a steady increase in NMSC incidence rates from 1960 to 2000. 12 The more gradual increase in NMSC incidence in New Brunswick versus British Columbia may be real, reflect the smaller study population (729,000 in New Brunswick versus 3.91 million people in British Columbia), or reflect the fact that the British Columbia Cancer Registry counts multiple primary BCCs and SCCs per individual patient. 8
Our study likely underestimates the disease burden of NMSC in the province in several ways. First, the requirement for histologic confirmation means that tumor registries miss NMSC that has not been brought to medical attention. Second, a tumor registry cannot take into account the unknown number of NMSCs, such as superficial BCC, that are treated destructively, such as with cryotherapy, and without histologic confirmation. Buettner and Raasch estimated that 10 to 20% of clinically diagnosed skin cancers in Townsville, Australia, were treated without histologic confirmation. 13 Third, by counting only one BCC and invasive SCC per person per lifetime, this registry cannot account for the significant number of individuals who develop multiple primary NMSC over their lifetime. Finally, the completeness of the Provincial Cancer Registry in terms of NMSC reporting has never been confirmed by means of an audit.
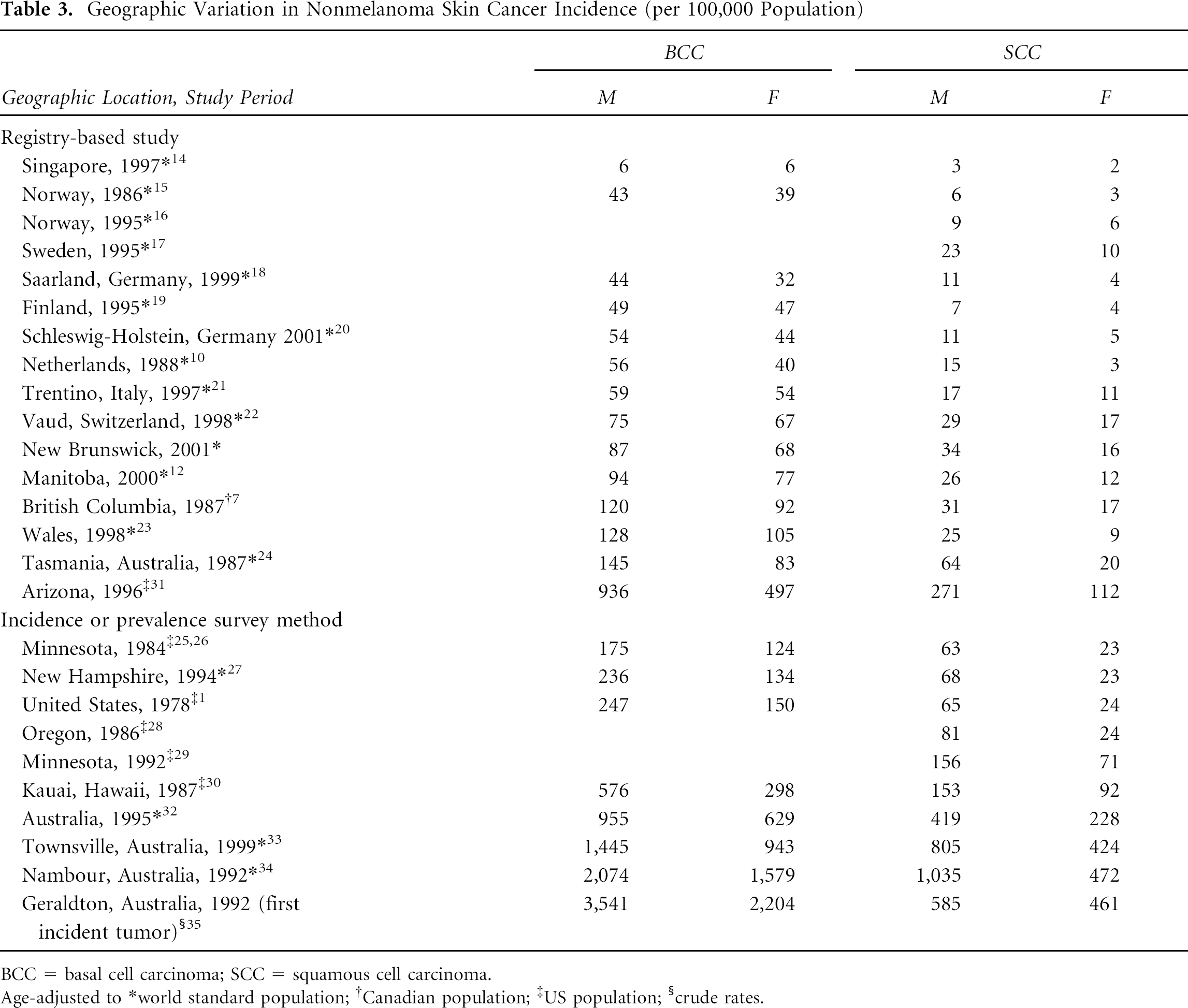
The incidence rates of NMSC in New Brunswick are similar to those in Switzerland and higher than all other countries in Western Europe and Scandinavia (Table 3).14–35 A notable exception is South Wales, United Kingdom.23,36 The incidence rates of NMSC in New Brunswick are lower than those published from all regions of the United States and Australia. When age-matched to the world standard population, the incidence rates of BCC were approximately 15 times higher in Townsville, Australia, than in New Brunswick, and the rates of SCC were approximately 26 times higher. 33
Geographic Variation in Nonmelanoma Skin Cancer Incidence (per 100,000 Population)
BCC = basal cell carcinoma; SCC = squamous cell carcinoma.
Age-adjusted to world standard population;
Canadian population;
US population;
crude rates.
There is marked geographic variation in the incidence of NMSC, with nearly 50-fold differences in the incidence of BCC and 100-fold differences in SCC between the Caucasian populations of Finland and Australia.13,37 Although differences in study methodology may account for some variation in NMSC incidence among different populations, other factors likely play a more important role. 37 Geographic differences in sun exposure likely play a major role in terms of the long-term risk of NMSC. Intermittent high-dose sun exposure during childhood has been proposed as a risk factor for BCC, whereas cumulative sun exposure has been identified as a risk factor for SCC.38–40 Regions such as northern Australia, where a predominantly Caucasian population lives for its entire lifetime in close proximity to the equator, have the highest rates of NMSC in the world and a higher ratio of SCC to BCC than areas such as northern Europe.32–35,41
Relatively few cancer registries worldwide currently track NMSC, with notable exceptions being Finland, Tasmania, and a handful of European regions.10,19,42 Several factors make the registration of NMSC difficult. Owing to the sheer frequency of NMSC in the population, tumor registries may be overwhelmed with the number of lesions requiring registration.6,10,43–47 In countries such as the United States, complete registration of NMSC may be difficult owing to the number of private facilities involved in clinical care and pathology. In the United States and Australia, investigators have largely relied on either special population-based incidence surveys or directed screening of defined populations (repeated prevalence studies) to estimate the disease burden of NMSC.1,7,34,48–52 The last major survey of NMSC incidence in the United States took place from 1977 to 1978, when the National Cancer Institute ascertained the rates of NMSC in eight distinct geographic areas. 1 In 1994, these data were combined with the rising incidence trends of NMSC in two populations, British Columbia, Canada, and a health management organization in Oregon, to estimate a lifetime risk in the United States for BCC of 28 to 33% and for SCC of 7 to 11%.9,28,53
A fundamental difficulty when comparing epidemiologic studies of NMSC is the varying definition of incidence and the issue of tumor multiplicity. 5 Unlike most solid tumors, many individuals experience multiple primary NMSCs, particularly BCC, over their lifetime.53,54 The 3-year cumulative risk of developing a new subsequent BCC after being diagnosed with an index BCC is 44%, which represents at least a 10-fold increased risk when compared with the general population. 55 The 3-year cumulative risk of a subsequent SCC after an index SCC is 18%. 55 Several tumor registries, including ours, define incidence as the number of individuals who develop a single newly incident tumor of a given histologic type over a defined time period; patients with a history of skin cancer are excluded.14,18,19 Only considering the first lesion of BCC and invasive SCC in a patient's lifetime may be an inadequate way to describe the burden of NMSC in a population. Other registries include persons who have had that type of tumor prior to the study period.24,31 Some survey and screening-based studies count each independent primary skin cancer separately.13,33,35,56
In Townsville, Australia, a region with an extremely high rate of skin cancer, 38.5% of patients with NMSC had multiple tumors, with a median number of three excised tumors over a 33-month study period. 33 When the total number of NMSC lesions was taken into account, the ASIRs for BCC increased by 2.1 times in men and 1.6 times in women, whereas the ASIRs for SCC increased by 1.8 times in men and 1.4 times in women. 33 Raasch and Buettner emphasized the importance of reporting both the incidence rates of NMSC and the total number of primary NMSC lesions that are treated, with long-term follow-up of at least 5 to 10 years, to assess the “true” burden of NMSC. 33
Our data, although subject to the same biases as other NMSC registries, are likely an accurate reflection of the incidence of individuals newly diagnosed with BCC and SCC in both the province of New Brunswick and the rest of Canada. If one were to extrapolate the Canadian ASIRs of NMSC from the New Brunswick Cancer Registry to the entire Canadian population (31,752,842), there would be approximately 33,637 newly incident cases of BCC per year and 11,968 cases of newly diagnosed SCC per year nationwide. 8 If one were able to account for recurrent and subsequent primary NMSC lesions, the true incidence of disease would likely be much greater.
Reliable, reproducible means of longitudinally evaluating the incidence of NMSC in specified populations over time, whether in the form of tumor registries or surveys, are essential to assess the effectiveness of primary prevention and early detection programs. 57 A recent nationwide Australian survey noted that although rates of NMSC continue to rise, the incidence of BCC is decreasing in people under the age of 50 years. 32 This suggests that in Australia, a country with a 20-year history of extensive public education on skin cancer and sun protection, primary prevention may be having an impact on the reduction of disease.58,59 Tumor registries, such as those in New Brunswick, are particularly valuable in their ability to monitor NMSC incidence over time. In the future, tumor registries should endeavor to track both the total number of BCCs and SCCs in the population, in addition to the number of individuals with newly incident tumors, to estimate the true burden of NMSC.